
Abstract
Adrenocortical cancer (ACC) is a rare disease that is difficult to treat. Surgery remains the primary treatment modality and the only chance for cure in these patients. Since the early 1990s, laparoscopic adrenalectomy (LA) has replaced open adrenalectomy (OA) as the gold standard for addressing adrenal disorders of benign origin; however, the oncologic effectiveness of laparoscopic adrenalectomy for resection of primary adrenocortical malignancies remains unclear. Since the initial consensus statement from the International Adrenal Cancer Symposium held in Ann Arbor, MI in 2003, a number of studies have investigated the question of equivalence of LA compared to OA for ACC. Several controversial topics were debated during the 3rd International Adrenal Cancer Symposium held in Wurzburg, Germany in 2011. This debate sought to review the advantages and disadvantages of OA versus LA and review findings of recent studies related to the topic. As all studies involving this topic have methodological flaws, some more than others, the results of each study must be interpreted with caution. In conclusion, this debate will undoubtedly continue well into the future; however, it is clear that an oncologically appropriate surgical resection is of the utmost importance for the treatment of ACC and there is only one chance to achieve this. Poor outcomes will result from inadequate surgery, whether performed by an open or laparoscopic approach. Therefore, there is no doubt that surgery for suspected ACC should only be performed in specialized centers.
Similar content being viewed by others

Introduction
Adrenocortical cancer (ACC) is a rare disease that is difficult to treat. Surgery remains the primary treatment modality as progress in finding new treatments has been slow [1]. Two major determinants of long-term survival are tumor stage at presentation and curative resection by an experienced surgeon [2]. With a soft consistency, thin capsule and little available adjacent soft tissue to obtain wide margins, deviations from oncologically sound technique for ACC are followed by local and/or peritoneal recurrence. Of the entire multidisciplinary team involved in treating the ACC patient, it is the surgeon who is most able to positively or negatively impact recurrence rates in the tumor bed and peritoneal cavity. Until the advent of laparoscopic surgery and development of the technique for laparoscopic adrenalectomy (LA), open adrenalectomy (OA) was the standard operation performed for all adrenal disorders. Since the early 1990s, LA has replaced OA as the gold standard for addressing adrenal disorders of benign origin [3–5]; however, the oncologic effectiveness of laparoscopic adrenalectomy for resection of primary adrenocortical malignancies remains unclear.
Published data comparing the efficacy of LA versus OA for ACC are limited. Larger series include less than 200 patients with the majority of reports including less than ten patients who have limited or no follow-up. The vast majority of studies, including the larger series and those referenced in this current article, are hampered by referral bias and the fact that they are retrospective in nature. Often, patients included in series from tertiary referral centers have not had their initial care or surgical resection performed at the referral center which introduces additional confounding factors. Recommendations published after the 1st International Adrenal Cancer Symposium [6] held in Ann Arbor, MI, USA in 2003 with regard to surgical approach stated there was no role for laparoscopic removal of a known or likely ACC, but controversy existed regarding the role of laparoscopic removal of indeterminate lesions that could be ACCs. The recommendations further suggested that despite the small gains of laparoscopic surgery in terms of morbidity and ease of recovery from the procedure, an open approach is quite safe and successful with low morbidity and mortality, especially for tumors that would be amenable to a laparoscopic approach. Other formal recommendations published by recognized endocrine societies recommend an OA by an experienced surgeon as the procedure of choice [7]. An en bloc resection including any attached surrounding tissues (kidney, liver, inferior vena cava, pancreas, spleen, and stomach) should be performed along with regional lymphadenectomy. Violation of the tumor capsule is the most obvious of oncologic resection failures and is believed to increase the possibility of local recurrence; marginal resection without the benefit of excising surrounding tissue is also likely to decrease the effectiveness of the only curative option as ACC is commonly found to grow through the capsule of the gland in a microscopic fashion and lack of excision of surrounding tissue may lead to positive margins [2].
Since the initial consensus statement from the International Adrenal Cancer Symposium in 2003, a number of studies have investigated the question of equivalence of LA compared to OA for ACC. Since the answer remains unclear, this debate, as one of several controversial topics debated during the 3rd International Adrenal Cancer Symposium held in Wurzburg, Germany in 2011, sought to review the advantages and disadvantages of both approaches and review the findings of recent studies related to the topic. Dr. Gerard Doherty argued from the point of view that OA is superior to LA, and Dr. Francesco Porpiglia argued that LA is equivalent to OA with regard to oncologic outcome. The following material reflects the data and thought processes used to express the two opinions during the debate.
Open Adrenalectomy is Oncologically Superior to Laparoscopic Adrenalectomy for Resection of ACC—The Ann Arbor View
Examination of any surgical technique for malignancy must consider the ability to perform the operation using appropriate oncologic principles of resection. For ACC this in part entails: (1) a no touch technique as much as possible; (2) preservation of the intact peritoneum on the anterior surface of the adrenal gland to maintain the anterior margin if the tumor has not invaded through the overlying peritoneal layer; (3) removal of the tumor in an en bloc fashion with a wide margin of surrounding benign tissue to encompass microscopic extension of tumor outside the tumor capsule (which may or may not include adjacent organs or vessels); (4) preservation of the entirely intact tumor capsule; (5) exclusion of the remainder of the peritoneal cavity as much as possible using some sort of barrier (laparotomy pads, plastic barriers/drapes, etc.); (6) minimization of bleeding and amount of fluid allowed to escape into the rest of the peritoneal cavity; and (7) gloves, gowns, and instruments should be changed after removal of the tumor and prior to closure of the abdomen. An open approach is the optimal technique in which to carry out these principles. A laparoscopic approach excludes items 5, 6, and 7. In addition, tactile sensation is limited compared to an open approach with regard to the pressure applied to the tumor if it has to be manipulated. This is important since these tumors typically have an extremely thin capsule that is prone to rupture. The ability to resect the retroperitoneal fat surrounding the tumor is more difficult using laparoscopic techniques, as the fat tends to fall away from the tumor. This is important when microscopic extensions of the tumor invade the surrounding peri-adrenal fat. It is not possible to recognize these extensions at the time of resection by either approach. These extensions upstage the patient to stage 3 and are likely an important source of tumor cells remaining in the abdomen and spread elsewhere in the peritoneal cavity. The ability to assess adherence of the tumor to adjacent structures without uncovering the tumor and potentially spreading cells is also more difficult laparoscopically.
Of the studies evaluating LA versus OA for ACC that have been published since the 1st International Adrenal Cancer Symposium, several merit further discussion and are summarized in Table 1. In 2010, Porpiglia et al. reported evidence that LA may be comparable to OA in patients with stage 1 and 2 ACC based on no significant difference in recurrence-free survival [8]. A significant limitation of the study, however, was the fact that patients who did not have radical resections or who had macroscopically incomplete resection, tumor capsule violation, conversion from laparoscopic to open surgery, and those found to have microscopic peri-adrenal fat invasion based on final pathology (stage 3 after surgery) were excluded from the study. It is precisely these types of patients who should be included when evaluating the equivalence of the two techniques. Many stage 3 patients have only microscopic extension of tumor, and this cannot be identified by preoperative imaging or by the surgeon during the operation. It is imperative that these tumors be resected intact with surrounding tissue to assure negative margins. By excluding these patients based on final pathology, the question of the decision to perform surgery laparoscopically and assure an oncologically equivalent outcome cannot be thoroughly assessed. Local recurrence, which was not defined, was reportedly equivalent (6/25 LA, 6/18 OA, p = 0.5), but no specific comment was made regarding peritoneal recurrence, which as an initial site of recurrence is associated with shorter survival than other initial sites of recurrence. Additionally, the length of follow-up in some patients was less than 1 year, potentially not allowing for identification of recurrence. It is not possible from these data to conclude that LA is oncologically equivalent to OA.
A study from the German Adrenocortical Carcinoma Registry Group reported no difference in survival, disease-free recurrence, tumor capsule violation, or peritoneal carcinomatosis among 117 patients undergoing OA and 35 patients undergoing LA for stage 1–3 ACCs less than 10 cm [9]. Patients undergoing LA were also matched with a patient having undergone OA according to stage, tumor size, adjuvant therapy, age, and presence of glucocorticoid excess. While matching LA and OA patients is appropriate, details regarding the specific technique of resection with respect to the many facets of an oncologically appropriate resection were not detailed. If the resection techniques from an oncologic standpoint were compromised, a difference between the two techniques would likely not be apparent. Three times as many patients in the OA group had stage 3 disease. Four patients (11%) undergoing LA were found to have stage 3 disease. Whether this was known at the time of surgery and these patients underwent en bloc resection of adjacent organs and tissue to allow for negative margins is unknown. It is unknown whether this was microscopic or macroscopic invasion of adjacent tissues. In five or more cases, it appears that the tumor may have been exposed or violated during the laparoscopic portion of the case meaning it is possible that oncologic principles may have already been violated leading to a different outcome than if the case had been performed open from the beginning. No specific data related to those patients undergoing OA who had R1 and R2 resections is given to allow insight into why fairly manageable tumors from a size standpoint were unable to be resected completely, especially since all of these tumors were less than 10 cm. R2 resections likely should have been further investigated as to whether this was intentional or not. If the tumor was intentionally left behind, these patients should have been excluded from the study as the intent of resection has become palliative rather than curative. Additionally, data were not available regarding resection status for 33% of OA and 26% of LA patients (37% of the entire study group) limiting the conclusions that may be drawn about equivalence of the two techniques. Tumor capsule violation appeared similar for LA and OA, but these occurrences were not delineated as to tumor stage, as tumors are more difficult to resect intact as the stage increases. Again, as in all of the other studies, follow-up in some patients was short.
Leboulleux et al. investigated whether or not the surgical approach was a risk factor for the development of peritoneal carcinomatosis [10]. Their report included 64 patients with stages 1–4 disease. Median follow-up was 35 months. Fifty-eight patients underwent OA and six underwent LA. Peritoneal carcinomatosis occurred in 18 (28%) patients and it occurred during follow-up in 12 cases after operation for potential cure. Peritoneal carcinomatosis was found in three of five patients undergoing LA and 9/36 undergoing OA. The only risk factor of peritoneal carcinomatosis occurring during follow-up for the entire study group was the surgical approach (p = 0.016).
Data reported from MD Anderson Cancer Center in 2005 revealed a high risk of peritoneal carcinomatosis after LA [11]. All six patients who underwent LA had recurrence, with peritoneal carcinomatosis as a component of initial failure in 83% (five of six) versus 8% in 133 undergoing OA. While limited by a small number of patients in the laparoscopic group and potential referral bias being at a tertiary referral center, they concluded that OA should remain the standard of care. In follow-up to that publication, in 2010, they showed that resection at a facility other than their own was associated with worse outcome [12]. This applied only to OA, as LA for ACC is not performed by this group.
Researchers at the University of Michigan showed in a study published in 2008 that 17 patients undergoing LA experienced significantly faster local recurrence in the tumor bed, a significantly higher incidence of violation of the tumor capsule, margin positive resections, and greater rates of peritoneal recurrence than 71 patients undergoing OA [13]. Overall recurrence including all sites was similar; however, studies of surgical quality should first and foremost concentrate on local and peritoneal recurrence as the quality of surgical resection definitely impacts the above factors, but likely has a much smaller role in distant metastases. Seventy-nine percent of operations were performed at outside facilities, and no laparoscopic operations for ACC were performed at the University of Michigan, again potentially introducing a referral bias; however, ACC patients were referred at all time-points in their disease course, not just after recurrence was identified. The authors commented that any guidelines created should be directed to those practicing as general surgeons and urologists, not just to those who truly are experts in a small subspecialty field, as the majority of adrenal cancers are resected by general surgeons and general urologists and not by subspecialists having a particular interest and significant expertise in treating ACC. In addition, the argument of allowing experts in LA to resect ACCs laparoscopically is flawed as no one has defined what an expert is for ACC [13].
Becoming facile performing LA for benign tumors is entirely different than performing an oncologically precise resection for ACC. ACC is rare and most physicians do not understand its unforgiving nature compared to other malignancies if a poor quality resection is performed. One inadvertent maneuver during surgery can lead to a completely different outcome. Newly updated results (personal communication) from a larger study group of patients undergoing OA and LA for ACC have shown a significant difference in overall survival (p = 0.03), with 31 patients undergoing LA having a shorter survival (20.6 months) than 82 patients undergoing OA (40.2 months) despite those in the LA group having significantly smaller tumors and lower stage disease at the time of resection and receiving mitotane and external beam radiation therapy more often.
While some malignancies can be resected with equivalent oncologic outcomes employing a laparoscopic approach, those tumors are not ACC, which in most patients is an aggressive tumor with a soft capsule, has limited adjacent margins for resection, and poor options for adjuvant therapy. With essentially no progress having been made in the past 30 years, surgical technique must be optimized. It is the opinion of these authors that many open resections may not be performed in a fashion that adheres to oncologic principles, and this may be the reason why no differences are seen between laparoscopic and open approaches in some studies. The group at MD Anderson follows the principles of oncologic resection as do the UM group. Both have shown outcomes in their own patients, superior to those patients referred for care after resection at outside facilities. This may also be due to selection bias. The lack of adherence to oncologic principles of resection likely leads to increased incidence of local and peritoneal recurrence.
In summary, ACC is a tumor that can be locally aggressive as well as distantly metastatic for which we have very limited curative options. The only current approach that is potentially curative is an initial expertly performed operation using oncologically sound principles. We believe that there are important practical reasons why this may be best achieved by an open resection, and that there are imperfect data to support this. Our own clinical experience with local and peritoneal recurrence patterns in patients who have had lethal outcomes following laparoscopic resection of ACC appropriately bias us. These patients have one chance to have a complete resection. We should not compromise our efforts on their behalf by undertaking an approach for which the only advantages are fleeting, but the disadvantages may cost them their life.
Laparoscopic Adrenalectomy is Oncologically Equivalent to Open Adrenalectomy for Resection of ACC—The Turin View
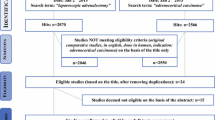
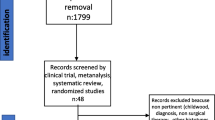
We searched in PubMed database all the papers focusing on surgical treatment for adrenal masses. We selected only cases treated with laparoscopic approach and with pathological diagnosis of ACC. As a result, in these series, 1,783 patients have been treated with LA and the number of patients with ACC was 114 (6.4%). The median follow up was 32 months, and the tumor size was 6.95 cm. The recurrence rate of the 114 patients with ACC was 21.5%, the death rate was 31.5%, and the disease-free rate was 43%.
Concerning these data, more recent reports demonstrate that oncological outcomes of LA are similar to open surgery [8, 9, 14], when laparoscopy is performed in referral centers with a minimum number of LA per year >20 [15–17]. In a multicentric study, Brix et al. [9] compared two groups of patients: the first one treated with LA and the second one treated with OA.
One hundred fifty-two patients were included, after a median follow-up of 39.3 months. The authors reported a recurrence rate of 77% in the LA group and 69% in the OA group (p = 0.36), with a death rate of 37% and 41%, respectively (p = 0.68). Overall and recurrence-free survival was not different between the 23 patients treated with LA and the subgroup of 23 matched OA controls. They registered 12 LA converted to OA but the outcome was not different compared to the 23 completed LA. The authors concluded that LA is not inferior to OA in localized ACC ≤10 cm with regard to oncologic outcome; therefore, LA performed by an experienced surgeon is justified for potentially malignant adrenal incidentalomas and for selected cases of stages 1 and 2 ACC.
Porpiglia et al. [8] studied 43 patients with stages 1 and 2 ACC treated with open or laparoscopic approach, with a median follow-up of 35 months. They registered a recurrence rate of 64% in the OA group and 50% in the LA group. The percentage of surviving patients after 3-year follow-up was 84% in the OA group and 100% in the LA group (p = 0.3). In the multivariate analysis, treatment modality was not an independent prognostic factor of recurrence-free survival. The conclusion of the paper was that laparoscopic and open approaches are comparable for stages 1 and 2 lesions when the principles of oncologic surgery are respected.
Nevertheless, many authors emphasize that the risk of local recurrence and positive margins after LA is higher than after OA [10, 11, 13].
Gonzalez et al. [11] registered a local recurrence rate of 100% (six of six patients), but all six patients underwent LA before referral and the paper does not provide the adrenalectomy volume of the laparoscopic centers. Moreover, a technical error occurred (tumor fracture during attempted bag extraction) and one conversion to OA was necessary (laparoscopic or surgical seeding?).
Miller et al. [13] described over 17 patients, treated with LA for ACC, a rate of positive margins or intraoperative tumor rupture of 50%, but 2/17 patients had preoperative biopsy which is discouraged in patients with presumed ACC due to the risk of tumor spread.
Regarding the laparoscopic approach, in the contemporary series [8, 9, 14, 18], only 12/94 patients with ACC have been treated by retroperitoneal LA and there are no studies focusing on the comparison between trans- versus retro-peritoneal approach.
In summary, LA is criticized in the literature on the grounds that its oncologic efficacy is considered limited, but these conclusions are based on small series of patients treated by centers where the technique was probably not refined.
In recent years, the knowledge and technology have changed greatly and the treatment of this rare disease is increasing in referral centers. In these centers, data are often prospectively collected and authors are able to analyze and publish.
Two European referral centers have studied this topic and have concluded that in the early stages of the disease and in selected cases, there are not significant differences in terms of oncological efficacy between OA and LA [8, 9].
The merit of these papers is not only to demonstrate that the results of LA, in selected cases, are similar to those of OA, but to support that LA is a correct approach for incidental adrenal masses that are potentially malignant (ACC).
Starting from these works, we can critically evaluate whether the statement of the conference on 2003 is still well founded. We believe that this statement should be reviewed because we think that LA for ACC is feasible, safe, and effective but should be performed only when two criteria are respected:
-
1.
Surgery for suspected ACC should be limited to referral centers with experience in this kind of oncological surgery and with more than 20 LA per year, independently of the access;
-
2.
Surgery must include meticulous preservation of tissue planes and avoidance of tumor violation during dissection and specimen extraction; moreover, the specimen has to be extracted without fragmentation.
If these two criteria are respected and a surgical excision is indicated, LA can be considered for the following adrenal lesions:
-
1.
Indeterminate small incidentaloma;
-
2.
Indeterminate large incidentaloma, without necrosis or evidence of invasion; and
-
3.
Likely small ACC.
Debate Conclusion
Without doubt, this debate will continue well into the future; however, it is clear that an oncologically appropriate surgical resection is of the utmost importance for the treatment of ACC and there is only one chance to achieve this. Poor outcomes will result from inadequate surgery, whether performed by an open or laparoscopic approach. As all studies involving this topic have methodological flaws, some more than others, the results of each study must be interpreted with caution.
References
Bilimoria KY, Shen WT, Elaraj D et al (2008) Adrenocortical carcinoma in the United States: treatment utilization and prognostic factors. Cancer 113(11):3130–3136
Allolio B, Fassnacht M (2006) Clinical review: adrenocortical carcinoma; clinical update. J Clin Endocrinol Metab 91:2027–2037
Janetschek G (1999) Surgical options in adrenalectomy: laparoscopic versus open surgery. Curr Opin Urol 9:213–218
Gill SI (2001) The case for laparoscopic adrenalectomy. J Urol 166:429–436
Porpiglia F, Garrone C, Giraudo G et al (2001) Transperitoneal laparoscopic adrenalectomy: experience in 72 procedures. J Endourol 15:257–259
Schteingart DE, Doherty GM, Gauger PG, Giordano TJ, Hammer GD, Korobkin M, Worden FP (2005) Management of patients with adrenal cancer: recommendations of an international consensus conference. Endocr Relat Cancer 12(3):667–680
Zeiger MA, Thompson GB, Duh QY, Hamrahian AH, Angelos P, Elaraj D et al (2009) American Association of Clinical Endocrinologists and American Association of Endocrine Surgeons Medical Guidelines for the Management of Adrenal Incidentalomas. Endocr Pract 15(Suppl 1):1–20
Porpiglia F, Fiori C, Daffara F, Zaggia B, Bollito E, Volante M et al (2010) Retrospective evaluation of the outcome of open versus laparoscopic adrenalectomy for stage I and II adrenocortical cancer. Eur Urol 57:873–878
Brix D, Allolio B, Fenske W, Agha A, Dralle H, Jurowich C et al (2010) Laparoscopic versus open adrenalectomy for adrenocortical carcinoma: surgical and oncologic outcome in 152 patients. Eur Urol 58:609–615
Leboulleux S, Deanderis D, Al Ghuzian A, Auperin A, Goere D, Dromain C et al (2010) Adrenocortical carcinoma: is the surgical approach a risk factor of peritoneal carcinomatosis? Eur J Endocrinol 162:1147–1153
Gonzalez RJ, Shapiro S, Sarlis N, Vassilopoulou-Sellin R, Perrier ND, Evans DB et al (2005) Laparoscopic resection of adrenal cortical carcinoma: a cautionary note. Surgery 138(6):1078–1085, discussion 85–6
Grubbs EG, Callender GG, Xing Y, Perrier ND, Evans DB, Phan AT, Lee JE (2010) Recurrence of adrenal cortical carcinoma following resection: surgery alone can achieve results equal to surgery plus mitotane. Ann Surg Oncol 17:263–270
Miller BS, Ammori JB, Gauger PG, Broome JT, Hammer GD, Doherty GM (2010) Laparoscopic resection is inappropriate in patients with known or suspected adrenocortical carcinoma. World J Surg 34:1380–1385
McCauley LR, Nguyen MM (2008) Laparoscopic radical adrenalectomy for cancer: long-term outcomes. Curr Opin Urol 18:134–138
Park HS, Roman SA, Sosa JA (2009) Outcomes from 3144 adrenalectomies in the United States: which matters more, surgeon volume or specialty? Arch Surg 144:1060–1067
Murphy MM, Witkowski ER, Ng SC, McDade TP, Hill JS, Larkin AC et al (2010) Trends in adrenalectomy: a recent national review. Surg Endosc 24:2518–2526
Kazaure HS, Roman SA, Sosa JA (2011) Adrenalectomy in older Americans has increased morbidity and mortality: an analysis of 6,416 patients. Ann Surg Oncol 18(10):2714–2721
Greco F, Hoda MR, Rassweiler J, Fahlenkamp D, Neisius DA, Kutta A et al (2011) Laparoscopic adrenalectomy in urological centres—the experience of the German Laparoscopic Working Group. BJU Int 108(10):1646–1651
Conflicts of interest
There are no conflicts of interest for any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
Francesco Porpiglia and Barbra S. Miller contributed equally as first authors, and Cristian Fiori and Gerard M. Doherty contributed equally as senior authors to this manuscript.
Rights and permissions
About this article
Cite this article
Porpiglia, F., Miller, B.S., Manfredi, M. et al. A debate on laparoscopic versus open adrenalectomy for adrenocortical carcinoma. HORM CANC 2, 372–377 (2011). https://doi.org/10.1007/s12672-011-0095-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12672-011-0095-1