
Abstract
The nutrition transition literature has generally drawn on epidemiologic and demographic changes to make its argument, because in many cases broader data are not available on the drivers of nutrition change. Going further, this paper draws on wider food systems literature, and includes food price and expenditure data, to join the dots from macroeconomic and food system change to food sources, production, and price; to household-level expenditures; to changing diets and nutrition and health outcomes, illustrated through the case of Zambia. Many of the economic and demographic drivers of the nutrition transition are present in Zambia, including rising GDP, high urbanization and increasing supermarket penetration. Food supply data show a reduction in calories available per capita over several decades, and low levels of nutrient-rich plant and animal source foods which make up a diverse, nutritious diet. National food price data show that while the cost of food has reduced overall, nutrient-rich foods are more expensive relative to staple foods over time. Expenditure on staple foods has reduced in the past two decades while spending on fruits and vegetables, animal source foods, fats and sugars, and processed foods has increased, with these change greater in rural areas in recent years, but already more advanced in urban areas. Finally, while undernutrition is reducing slowly from very high levels and hunger persists, overweight and obesity and non-communicable chronic diseases are increasing; and data are strikingly lacking on modern Zambian diets. The Zambia case study is placed within regional and global trends to illustrate nutrition transition changes that are now happening in rapidly changing lower-middle income countries. Policy responses include promoting the availability of diverse nutrient-dense foods, and concurrent attention to preventing under- and over-nutrition in surveillance and policy. This paper also sheds light on the gaps in information that would greatly improve our understanding of the food system drivers of the nutrition transition, and hence our ability to create relevant policy.
Similar content being viewed by others


1 Introduction: Drivers of a nutrition transition
Researchers have for decades been studying a process of demographic and epidemiological change associated with changing nutrition and health outcomes, described as a ‘nutrition transition’ (Popkin 1994). Despite regional, national and local nuances, the original observers of the nutrition transition have been remarkably accurate in their predictions of how changes in social and economic forces connecting populations would impact diets, and how - combined with the impacts of changing built environments and working patterns on activity levels - these would manifest as altered nutrition and health outcomes globally (Popkin 1994).
Classical work on nutrition transition has focused on linked demographic and epidemiological transitions. Our work brings into focus food systems as a key driver of the nutrition transition that complements these other dimensions of change. Broad drivers of food system changes largely stem from processes of global economic and demographic change, including the shift in agriculture practices after the green revolution, providing more and cheaper grain products for global markets; changes in the types of foods produced by the food system, to include more processed foods on the one hand and greater ability to distribute fresh foods on the other; increasing globalization of value chains reaching well beyond the agricultural production system; trade and investment liberalization providing access to more tradable, less perishable inputs particularly through the emergence of fast food outlets and supermarkets; urbanization of populations due to land and employment pressures, and changes to food acquisition options in urban areas; and changing preferences stemming from increased incomes, a growing interconnectedness of the global middle class, and broader reach of advertising and media marketing comparably cheap industrialized products (Pingali 2004, Ruel et al. 2008, Baker and Friel 2014, Rischke et al. 2015, Global Panel on Agriculture and Food Systems for Nutrition 2016, Cook 2017). Generally, it is those low- and middle-income countries whose food systems are highly penetrated by transnational food companies that are experiencing the fastest change in exposure to unhealthy processed foods (Stuckler et al. 2012). Trade liberalization policies have been a key factor contributing to dietary changes associated with growing incidence of obesity and NCDs (Thow et al. 2017).
These different supply- and demand-side pressures within food systems are mutually reinforcing the alteration of diets at a rapid pace (Hawkes 2008). Diets have been changing around the world for decades, and while countries experience these changes at different times and different paces, the patterns of change are similar across contexts. From traditional food regimes largely comprising seasonal consumption of coarse grains, pulses, fruits, vegetables and meat, a more uniform global diet is emerging, with increasing levels of animal foods, fat, sugar and processed foods; though some populations are moving back towards local and plant-based diets, most are moving away (Kennedy et al. 2004, Pingali 2004, Mehio Sibai et al. 2010, Misra et al. 2011, Baker and Friel 2014). This changing food intake is subsequently related to risk of nutrition-related chronic diseases such as obesity, type 2 diabetes, dyslipidemia, hypertension and cardiovascular diseases, and some cancers, with stagnating high burdens of micronutrient deficiency (Popkin 1994, Gillespie and van den Bold 2017a, 2017b).
The analyses below detail how global, regional and national economic and demographic changes are playing out in Zambia’s food supply, food prices, household expenditures, and diet and nutrition outcomes, to extend a growing literature on the nutrition transition in Africa into an analysis of the role of food systems.
2 Methods
This paper explicitly tries to go beyond the scope of many epidemiologically-focussed papers on the nutrition transition by including broader food system drivers in the analysis. In doing this, we lose some precision (because in general, epidemiological indicators are not found in the same datasets as food system indicators (Gillespie and van den Bold 2017a, 2017b)), but trade off for a broader understanding of the food system factors driving change, which we argue is necessary if we are to get to useful policy responses.
This paper draws on several sources of data to bring together an analysis of the changes in food and nutrition in Zambia over several decades (Fig. 1). Changes in food supply, food prices, and household food expenditures were calculated using available data for major foods and food groups relevant to food security and nutrition; then changes in diets and nutrition and health were assessed for nutritionally-vulnerable population groups. Throughout the paper, secondary data were used to paint a broad picture of the food system factors known to drive the nutrition transition and their presence in Zambia and in the southern African region, to describe the broader context of food and nutrition change that is occurring and which policies need to be addressed.

Data sources used in this paper. Source: Authors’ own creation
To look at changing food supply, the FAO Statistical Database on Food Balance (http://www.fao.org/faostat/en/#data/FBS) was used to calculate changes in food supply measured as kilograms/capita/year (kg/c/y). These food supply data, compiled by FAOSTAT, represents the per capita supply of food items (or food groups) available for human consumption. FAOSTAT provides several aggregate food categories (eg. cereals). For example, the FAOSTAT food groups of meat and offal were combined into “meat” and vegetable and animal fats were combined into “oils and fats”. Three year averages were calculated to demonstrate change over time using 1961–1963 as baseline and comparing with 2011–2013. The kg/c/y availability was compared to data also compiled by FAO on kcal/c/day and is displayed in the results section where it adds value to the analysis.
To look at changing food prices, we undertook a novel analysis of a price dataset compiled by the Zambian Central Statistical Office (CSO) showing prices of different food commodities from 1996 to 2015. Individual foods representing common purchases were chosen as markers of price change in each of the 12 FAO food groups (with the exception of ‘miscellaneous’ foods). For each of these foods, two price analyses were undertaken: Assessment of absolute change in price over time, deflated using the Consumer Prices Index (CPI), to get a sense of overall household food purchasing power; and assessment of price change relative to maize, to get a sense of the cost of diversifying food purchases away from the major staple.
To look at changing expenditure patterns, we undertook a novel analysis of changes in household food consumption over two decades in rural and urban Zambia using four rounds of the Zambian Living Conditions Monitoring Survey (LCMS 1996, 1998, 2010 and 2015). Changes in the patterns of consumption are largely driven by changes in income, urbanisation and population. In Zambia’s case all these factors have recorded positive growth in the last two decades. The method used was guided by the fact that Zambia experienced rising income, rapid urbanisation and population growth, which resulted in changes in households’ dietary preferences. Borrowing from Bennet’s law which postulates that the proportion of starchy staples in the diet decreases with increasing income, as income grows, consumers choose to spend it on foods that are more desirable. Cereals become less important and the share of high-value crops, such as fruits and vegetables, dairy and animal products, and fish, in the food expenditure basket increases (Wilde 1989, Hassen et al. 2016). Due to data deficiencies, we used expenditures shares in the total food basket, focussing on analysis of expenditures within the 12 FAO food groups, and expenditures on food with different levels of processing, the analysis being disaggregated by income group and by rural/urban areas. We used the expenditure share of each food item out of total food expenditure (expressed as a percentage) as an indicator of consumption. We acknowledge that increase in expenditure can result from price changes and increase in actual consumption, therefore, we undertook an analysis of trends in prices over time in real terms for the identified food groups. See the working paper by Chisanga and Mbata-Zulu (2017) for more detail on methods for calculating household food expenditure..
To look at changing diets, findings from several large publicly-available surveys were synthesized: The Zambian Demographic and Health Survey (DHS) collects regular data on the dietary diversity of young children (6–24 months) and so provides a snapshot of an aspect of diet quality among this age group (Central Statistical Office, Ministry of Health et al. 2014); several recent dietary surveys have been conducted among urban populations in Zambia; and the Zambia food consumption and micronutrient survey collected data on dietary patterns and micronutrient status in rural areas of two of Zambia’s ten provinces in 2008 (NFNC 2013). These various dietary data are presented as snapshots of the Zambian diet, but notably tell us little about differences between rural and urban or richer and poorer households, and little about change over time.
Finally, to assess changing nutrition and related health outcomes in Zambia, data on child stunting and overweight, and female underweight and overweight, were taken from the Zambian DHS between 1992 and 2014 (Central Statistical Office, Ministry of Health et al. 2014). A snapshot of changing nutrition-related chronic diseases (NCDs) was taken from a repeated World Health Organization survey of common NCDs in Lusaka city in 2007–8 and 2017–18 (WHO 2008).
Each of these sources of data has potential issues and sources of bias, as in any study, but each is accepted data in its field, and each can tell us something important about the food system drivers of nutrition transition. Notably, this paper cannot link each of these changes - to food system context, to food supply and price, to household food expenditures, and to changing diets and nutrition outcomes - into a single model of change; the data simply do not exist at all of these different levels in a form that would allow for standard statistical analysis. What this paper does instead is provide an overview of changes in key aspects of food and nutrition in Zambia, and sheds light on the gaps in information that would greatly improve our understanding of change, and hence our ability to create relevant policy.
3 Changing economic and demographic drivers
Sub-Saharan Africa (SSA) is one of the last global regions to go through the nutrition transition process as the forces of globalization have been slower to reach into the continent (Reardon, Tschirley et al. 2015). In 2011 it was reported that more than half of the countries in SSA were in the early stage of the nutrition transition, while a few had reached a position where changes in dietary patterns were affecting health outcomes in a significant proportion of the population (Abrahams et al. 2011). More recent assessments suggest that patterns understood to drive the nutrition transition are becoming entrenched: Globalization in terms of rates of market penetration by large-scale food businesses is growing fastest in the African region (Global Panel on Agriculture and Food Systems for Nutrition 2016), and the urbanization rate in Africa is higher than in most other regions (Reardon, Tschirley et al. 2015), both factors that affect the food environment for resident populations. From around 1975 to date, urbanization has been increasing steadily in SSA accompanied by a massive growth of industry, especially that of food manufacturing in urban areas of Africa (UNIDO 2013).
Zambia is seeing many of these changes play out within its borders, with many of the key drivers of the nutrition transition in place today. The KOF measure of globalizationFootnote 1 places Zambia as more politically and economically connected to world markets than its nearest neighbours, Zimbabwe and Malawi (though less so than an upper-middle income country such as South Africa). Zambia’s population has almost tripled since 1970, currently at around 16.2 million people (CSO 2012, CSO 2016), though the country remains quite sparsely populated due to its large landmass, making service provision and market access difficult in rural areas. The urban population reached 40% in the 1980s, stagnated and declined to about 35% by 2000 during a phase of counter-urbanization (Potts 2005) and then resumed its growth trajectory with the urban population doubling in number between 2000 and 2010 (CSO 2012). The 2010 Census put the urban population at 39% of Zambia’s total population (or around 5.1 million urban-dwellers) (CSO 2012).
Urban does not necessarily mean rich, though certainly many in urban areas are increasingly affluent. Zambia’s overall economic growth rate is high (with GDP growthFootnote 2 of between 3 and 10% throughout the twenty-first century), but it is also one of the most unequal countries in the world, with a GINI coefficientFootnote 3 of 57.5 placing the country 141st out of 187 countries on income equality. While urban dwellers on average have seen an increase in income over the past two decades, rural incomes have declined, and inequitable wealth distribution is also seen in urban areas, with urban poverty standing at around 23% and rural poverty at around 78% (CSO 2016). Zambia’s economic and demographic situation therefore suggests that the stage is set for a nutrition transition to occur.
4 Changing food sources
A change seen in many food system studies is the source of household food, away from subsistence agriculture and traditional wet-markets, and towards supermarkets and associated international supply chains and processed foods with longer shelf-life (Bloem and de Pee 2017). Supermarket chains have been overtaking traditional retailers in many countries for some time, and this is more common in urban areas with economies of scale (Reardon et al. 2003). In the more globalized nations in Africa such as South Africa and Kenya, supermarkets hold a significant share of food retail sales, and their national stores have spread into the market shares of surrounding nations (Weatherspoon and Reardon 2003), with evidence growing for the effect of supermarkets on the purchase of highly processed foods at the expense of unprocessed foods in parts of urban Africa (Rischke et al. 2015). Supermarkets in Africa initially targeted middle and high-income consumers and the urban middle-class (Weatherspoon and Reardon 2003). In many Southern African cities however it is clear that supermarkets increasingly figure into the food-sourcing strategies of poor urban households as well (Crush and Frayne 2011, Mulenga 2013). Supermarket penetration is a feature of urban life, but not all urban residents can afford supermarket prices, with mixed effects on access to fresh and processed foods. Analyses in Africa find that supermarkets and large-scale food manufacturers tend to affect different kinds of foods differently, spurring a reduction in highly processed food prices in particular (Reardon et al. 2003), meaning that traditional staples are often more expensive in urban areas than rural, whereas more processed foods are cheaper (Ruel et al. 2008). An additional change highlighted by much of the nutrition transition literature is an increasing proportion of ‘fast food’ or convenience foods obtained from restaurants or take-away vendors (Popkin 1994, Feeley et al. 2009). Food eaten away from home tends to be less healthy than home-prepared food, and change towards this more convenient, processed, energy-dense food tends to happen first in urban areas (Chicago Council on Global Affairs 2011) and among both high and low income consumers.
Subsistence and semi-subsistence farming is still a major source of livelihood and food for many Zambians, and many wealthier urban households maintain links to family maize production in rural areas. Large land area with low population density has meant that rural infrastructure and markets have had limited reach, with own-production and local trade more accessible than rural integration into national markets (Chapoto et al. 2012). Rainfall and seasonality play a large part in subsistence food production and there are certain times of year when even largely subsistence households need to purchase food, making most farming households both producers and consumers at different times. In Zambia in 2010, an average of 70% of food was purchased, 25% was home produced, and 5% gifted, by monetary value (though not by volume) (Global Panel on Agriculture and Food Systems for Nutrition 2016). Food acquisition is highly varied in Zambia, and recent surveys have shown that urban Zambians in particular use a combination of food outlets (small neighbourhood shops (kantemba), local shops, local markets, supermarkets and street vendors) for their food purchases, with different foods obtained from different outlet types (World Food Programme 2018); while there are differences between richer and poorer urban households, all used a variety of shops.
The growing role and impact of modern supermarkets is evident in Zambia, where South African stores in particular have captured a share of the richer urban market (Abrahams 2009). Zambia’s first international supermarket opened in 1995, and there are currently 48 such stores in urban centres,Footnote 4 selling fresh goods, partially processed foods such as maize meal, and ultra-processed convenience and snack foods. Concurrent with the rise in urban supermarkets, there has been a rapid increase in fast food chains and access to convenience food in Zambia, including through kantemba catering mostly to lower socio-economic groups, and a proliferation of fast food restaurants in Lusaka and other urban areas serving fried foods and meats, pizza, and other convenience foods. In a 2008 survey in two rural Zambian provinces, just over 20% of meals were eaten outside the home (NFNC 2013), and a 2018 survey found that 62% of wealthier urban households ate regularly from modern fast-food chains (World Food Programme 2018). Overall then, while Zambia is still a nation of farmers, the majority of Zambians purchase food, at least in some seasons. In urban areas an increase in supermarkets, fast food chains, and neighbourhood shops selling snack foods has meant a change in food sources for rich and poor.
5 Changing food supply
The foods available in a given food environment are largely what will be consumed by its inhabitants – and what is available to buy or grow has narrowed significantly in recent years, particularly in Sub-Saharan Africa (Herforth and Ahmed 2015). While supply of fruits, vegetables and pulses globally and in Africa are not sufficient to meet estimated requirements for healthy diets, supply of staple cereals, oils and animal foods has risen significantly (Herforth and Ahmed 2015). With demand shaping supply and supply shaping demand, it is important to understand trends in production in order to understand where to intervene.
The major staple food in Zambia is maize, and Zambian food policy aims at achieving national self-sufficiency in this staple crop, with large input and output subsidies for its production taking up around 80% of the agricultural budget (Chapoto et al. 2015). Despite record maize harvests in recent agricultural seasons, food availability in most food groups (kg/capita/day) has declined significantly in Zambia since the 1960s, and even with an increase in availability of roots (largely cassava, under cassava promotion policies) these declines have led to Zambia being classified as one of the three most undernourished countries in the world, with 46% of the population said to be hungry at certain times of the year (IFPRI, Welthungerhilfe et al. 2017). Though these data have previously been questioned by the government, the numbers have been found to be broadly correct given available data, with the most likely explanation being high population growth outstripping agricultural production capacity (Mukuka and Mofu 2016).
The proportion of total dietary energy derived from starchy staples in Zambia has dropped from 78 to 71% since the 1960s, though this is still very high. Well over half of the calories available per person in Zambia come from cereals, largely from maize. Total energy available in Zambia has fluctuated between 1961 and 2013 with the trend suggesting that energy intake per capita per day has been consistently below the recommended 2000 kcal per person per day since the 1990s (Fig. 2). By 2011, cereals (63%), starchy roots (17%), fat and oils (8%), and sugars and sweeteners (6%) were the four leading contributors to energy supply nationwide (Mwanamwenge and Harris 2017). The same national study showed that the availability of calories from fat and oils, and starchy foods had doubled at the expense of legumes, fruits and vegetables, and meat.

Zambian total dietary energy, 1992–2013. Source: FAOSTAT data for 1961–2013
As important as overall calorie availability is for hunger, availability of nutrient-dense non-staple foods is central to diet quality, and availability of many of these foods has also declined compared to population (Fig. 3). Per capita supply of vegetables, fruits, pulses, meat, fish and milk all declined overall between 1961 and 2011. Many of these declines in nutrient-dense non staple foods have been from an already low baseline. Fruit and vegetable availability has steadily declined from 33 and 13 kg/c/year (1961–63) to 27 and 10 kg/c/year (2011–2013) respectively, translating into a daily availability of 101 g per capita per day of fruit and vegetables, far below the WHO/FAO recommendation of 400 g (World Health Organisation 2003). Availability of pulses and nuts hit a low point in the early 1980s; since then per capita availability has fluctuated between 1.8 kg/c/y and 2.4 kg/c/y. In the category of animal source foods, there has been a decline in per capita yearly availability for meat, milk, and fish. The decline in meat is formed from a decrease in supply of beef balanced by an increase in supply of chicken, coinciding with a sharp increase in per capita availability of eggs in the 1970s, with the chicken and egg industry remaining buoyant in Zambia.

Percent change in food supply (kg/capita/year), 1961–2013. Source: Authors’ own analysis, based on FAO Food Balance Sheet data 1961–2013
At the same time as declines have been seen in the availability per capita of many nutrient-dense foods, availability of sugars, fats and oils has increased (Fig. 3). Over the past two decades in particular (1995–2013) there has been a sharp increase in vegetable oil availability per capita, rising from 1.52 kg/capita/year (1995) to 4.86 kg/capita per year (2013), translating to current daily caloric availability per capita of 116 kcal/day/capita (averaged over 2011–2013). A similar increase in sugar has taken place, where availability per capita per year has risen from 6 to 11 kg/c/y, translating into a daily kilocalorie of 102 kcal/c/d (2011–2013), and increase of 41 kcal/c/d from the baseline 3 year average (1961–1963) of 61 kcal/c/d.
Thus the nutrient-rich animal and plant foods have barely kept pace or fallen behind population growth in Zambia, while availability of sugars and fats has leapt ahead. Despite issues with the collection of these data, with non-commercial or subsistence-level production usually under-represented in a country such as Zambia,Footnote 5 we can see that the food system is broadly heading away from a diverse and healthy food supply.
6 Changing food prices
Changing supply is one determinant of people’s access to food, as it modulates physical availability. Another key determinant of food access is price, as it modulates economic access. Price is, in turn, affected by factors such as the availability of different foods through agriculture and food systems; production costs such as labour and transport; demand both locally and globally; exchange rates and macroeconomic policies for imports and exports; and the effects of any subsidies or trade policies on different food types (Ruel et al. 2008, Green et al. 2013). Where food markets are weak, as is the case in many low-income country contexts, food prices tend to be higher and more vulnerable to fluctuation (Ruel et al. 2008); in more globalized markets, supermarkets and large-scale manufacturers catalyse a secular reduction in food prices within those outlets, with lower prices paid per calorie particularly on processed foods, though no studies have reported prices per nutrient (Reardon et al. 2003, Rischke et al. 2015). Different foods are priced differently, with nutrient-dense, less processed foods such as fruits and vegetables and meats tending to cost significantly more than staple foods (Chicago Council on Global Affairs 2011, Crush et al. 2011, Miller et al. 2016), and in some urban areas, ultra-processed snack foods costing significantly less (Ruel et al. 2008, Jones 2015), meaning it is relatively less expensive to shift toward diets based on highly processed foods rather than fresh food.
Food prices are often different between rural and urban areas, and in general foods are more expensive in rural areas (Miller et al. 2016). Policies deliberately keeping foods cheaper for an urban workforce have been employed for many years in many countries (though structural adjustment policies reversed these in many low-income countries, with adverse consequences for many urban poor) (Ruel et al. 2008). On the other hand in some rural contexts households may have access to home- or locally-grown foods and so be less affected by price fluctuations (Chicago Council on Global Affairs 2011). It is also worth noting that many poor rural farming households are both buyers and sellers of food, so the consequences of changes in food prices for families are difficult to predict. In either rural or urban contexts, the poor are most affected by food price rises, and an increase in either staple or non-staple food prices has been shown to have a negative impact on ability to access adequate diets in poorer households (Chicago Council on Global Affairs 2011, Green et al. 2013).
In Zambia, food prices have changed significantly between 1996 and 2015. In absolute terms, the prices of most of the food groups we assessed have reduced substantially (Fig. 4). In particular maize, chicken and vegetable oils reduced by over 50% over that time; and cassava, tomatoes, milk, and sugar reduced by over 30%. This has increased the purchasing power of Zambian households of a given income for many foods, both nutrient-dense and highly processed. Notably however, the price of two of the most nutritious foods, fish and eggs, rose in absolute terms over this time.

Prices of foods - % change (absolute) 1996–2015. Source: Authors’ analysis of FAO Food Balance Sheet data
In relative terms, the price data show that many foods became more expensive over time in relation to maize (Fig. 5). While the price of tomatoes, chicken and cooking oil remain reduced over time relative to maize, the price of other foods has increased substantially. In particular, the price of fish, eggs and beef increased by over 70%, and the price of oranges, beans and milk by over 20%.

Prices of foods - % change (relative to maize) 1996–2015. Source: Authors’ analysis of FAO Food Balance Sheet data
Thus while the overall purchasing power of households may be increased for some foods, the cost of diversifying away from maize has become greater. While the cost of food has reduced overall, many of the key nutrient-rich foods in the Zambian diet have become more expensive relative to staple foods over time.
7 Changing household food expenditures
The proportion of food purchased rather than produced varies by location and income. Not all rural dwellers are poor, nor are all urban dwellers rich, with 55% of Africa’s middle class being rural (Tschirley, Reardon et al. 2015). Thus two key factors – level of income and level of urbanization – combine with food prices to determine impact on the affordability of nutritious diets (Frayne et al. 2014). Purchased food is 43% of the value of food consumption on average in rural areas in eastern and southern Africa but in urban areas it is closer to 90% and rises sharply with rising income (Dolislager 2014). So the urban rich in particular purchase most of their food, while the rural poor grow a larger proportion, but purchases account for a significant proportion of food acquisition even in rural areas of Africa; within the middle class (rural and urban), 60–80% of food or more is purchased (Tschirley, Reardon et al. 2015). Even for major staples such as maize, the share of net buyers is striking.
The availability of different foods, and their absolute and relative prices, are key determinants of what households choose to buy – alongside factors such as convenience, tastes and aspirations (Herforth and Ahmed 2015). Rising urbanization and income growth combine to create changes in what households spend their money on for consumption. As incomes rise, the choice of foods varies across food groups depending on the elasticity associated with each food commodity. Intuitively, this income elasticity of demand reflects whether a commodity is a necessity or a luxury, as well as a reflection of households’ consumption tastes and preferences (Cirera and Masset 2010).
In rural Zambia, about 39% of rural households are net buyers of maize (Chapoto et al. 2015). Within these broad trends, our analysis of nationally-representative data show clear changes to household food expenditure patterns in Zambia over time, and these have been different in rural and urban areas. Overall, between 1996 and 2015, household expenditure share on starchy staple foods reduced, while expenditure share on fruits and vegetables increased substantially, and share on animal-source foods and fats and sugars increased slightly (data not shown here), despite prices reducing in absolute terms for a majority of these food groups. Many of these changes were more pronounced in rural areas (Fig. 6), where expenditure share on staple foods reduced more significantly than in urban areas and expenditure share on fruits and vegetables increased more significantly, with much higher expenditure on both of these food groups overall in rural areas. Expenditure on animal source foods increased slightly in both rural and urban areas, with urban areas spending more on these foods overall. Expenditure on fats and sugars increased in rural areas but slightly decreased in urban areas, with expenditure on these foods being at similar levels in rural and urban areas by 2015.

Rural and Urban Household Expenditure shares on different Food Groups. Source: Authors’ Computation from: CSO, 1996.b; CSO, 1998; CSO, 2010 and CSO, 2015
A similar pattern plays out in differences between richer and poorer households (Fig. 7), where expenditure share in the bottom 25% of households (by income) decreased substantially on starchy staple foods between 1996 and 2015, from over 50% to under 30%; while expenditure by the richest 25% of households fell only slightly, from just over 30% to just under. At the same time, expenditure in the poorest households on fruits and vegetables and animal source foods increased substantially, while expenditure on these foods increased less significantly in richer households. Expenditure on sugars and especially on vegetable oils increased more substantially in poorer households than in richer, with around 10% of expenditure on these food groups in both richer and poorer households by 2015.

Richer and Poorer - Household Expenditure shares on different Food Groups
While it is impossible within the limitations of available data to separate out the price and consumption aspects of these changing household expenditures, we propose some tentative findings. Of note, overall decline in prices combined with rising per capita income have been major drivers of expenditures and indeed consumption patterns. The falling share of starchy staples and the rising share of animal source foods and vegetables conforms to Bennet’s law. Overall, expenditure on staple foods has reduced in Zambia, while spending on fruits and vegetables, animal source foods and fats and sugars has increased. This has occurred even in the context of falling absolute prices for most of these foods. All changes have been more marked in rural and poorer population groups since 1996, but with richer urban household expenditures, already much higher on animal source foods, fats and sugars, and processed foods than their poorer rural counterparts, have further increased. These data therefore paint a picture of changes in the types of foods that households have accessed, with a trend towards foods commonly seen in the nutrition transition.
Within each of these food groups, and not captured by conventional FAO food availability tracking, foods may be unprocessed, minimally processed, or highly processed, with noted effects on nutrition and health. Globally, there is increasing polarization to healthy and unhealthy dietary patterns, with food systems increasingly able to distribute nutrient-rich but easily perishable fresh foods, but also producing, marketing and distributing ultra-processed foods that are low in nutrients and high in fats, salt and sugar (Monteiro et al. 2010). Both healthy and unhealthy choices are generally increasing for the rich, while mostly unhealthy choices are accessible for the poor in low and middle income countries such as Zambia (Imamura et al. 2015, Chicago Council on Global Affairs 2011). Processed foods in general tend to comprise a sharply higher budget share in urban than rural areas of Eastern and Southern African countries (Dolislager 2014). The role of income and the food environment interact in options for food purchases, with higher-income urban residents spending more than double on processed foods than the poorest urban dwellers in six African countries (Global Panel on Agriculture and Food Systems for Nutrition 2016).
Assessment of food expenditures in Zambia by the level of processing of food again show rural-urban differences (Fig. 8).Footnote 6 Overall, the amount of processed food purchased has risen between 1996 and 2015, from just over 30% to well over 50% (data not shown here). This has risen more slowly, and from a lower base, in rural areas than in urban. In rural areas, still less than 50% of food expenditures were on any kinds of processed foods in 2015, while in urban areas this stands at over 65%. In both rural and urban areas, unprocessed foods have been replaced largely by low-processed foods between 1996 and 2015. In urban areas levels of expenditure on highly-processed foods are significantly higher than in rural areas. Highly processed foods still comprise a small share of Zambian expenditures, but these are higher in urban than rural areas.

Expenditure Shares on Processed and Unprocessed Food, by rural and urban population. Authors’ Computation from: CSO, 1996.b; CSO, 1998; CSO, 2010 and CSO, 2015
8 Changing diets
What households are buying has a bearing on what individuals are eating – but it is not possible to directly calculate individual diets from household expenditures because of imbalances in the sharing of food among household members (Haddad et al. 1996, Berti 2012). To understand diets, data must be collected at individual level across populations, but due to the intensive nature of these data they are rarely collected, and when they are, they generally cover young children and women of reproductive age, as they are assumed to be at greatest nutritional risk (Ruel et al. 2014). Where dietary data have been collected over time in different populations, they show a trend of change from traditional to modern diets (increase in meat, vegetables, fats and sweets; and decrease in cereals) with a move to urban areas (Steyn et al. 2006) and with rising income (Popkin et al. 2001), depending on context. More commonly, a proxy for dietary data is used, such as dietary diversity scores which capture consumption of different food groups, rather than foods, and are statistically associated with nutrient adequacy (Ruel et al. 2014).
A summary of studies undertaken on the urban–rural transition of diet in SSA has shown that, generally, the modern urban diet is less healthy than the traditional rural one: intakes of fat, sugar, and red meat are higher in urban areas, while people residing in rural areas consume more carbohydrates and fibre, and less protein and fat (Steyn and Mchiza 2014). In terms of household food access in African cities, Lusaka was around the middle of the pack in a 2011 study across 11 SADC cities, with around 60% of households having access to fewer than five food groups in the past 24 h (range: 35–84% across cities), and no household having access to more than 9 of 12 food groups (Crush et al. 2011). Within these food groups, there is a large diversification into processed foods in both urban and rural Africa, alongside diversification away from grains into non-staple foods (Reardon et al. 2015).
Traditional diets in Zambia are high in starches and largely vegetarian (with less than 10% of energy supplied by foods of animal origin for women and children in rural areas), and a diet based on Nshima (maize meal porridge) is still eaten for preference by a majority of Zambians, with side dishes (relishes) changing throughout the year with the seasons; rural diets in particular are characterized by monotony and seasonal periods of scarcity (Nyirenda et al. 2007, NFNC 2013). This traditional diet has been largely unchanged over the past century in many rural areas (Richards 1939), though in particular some traditional coarse grains such as millets have been replaced with maize; some wild meats with commercially-produced chicken and beef; and some local vegetables with their international cousins in some areas over time (NFNC 2013).
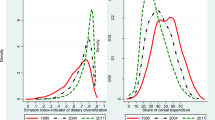
In the most recent Zambia Demographic and Health Survey only 22% of children aged 6–23 months received foods from four or more food groups out of 7, which is the cut-off for a minimally adequate diet (Fig. 9). Again the rural-urban divide and the role of inequality is marked: 18% of rural children and 31% of urban children had at least minimally diverse diets, and while only 15% of children in the lowest income households achieved this marker, 41% in the richest households did so (Central Statistical Office, Ministry of Health et al. 2014). This is still strikingly low even for richer households, however.

Percent of children aged 6-24 months receiving minimum dietary diversity. Source: Zambia DHS 2014
A recent survey in urban areas of Zambia found that among men and women, fruit was consumed on an average of two days per week (around 0.7 serving); vegetables 6 days per week (around 2 servings); and over 90% of individuals consumed less than the recommended five servings of fruits and vegetables per day, with little variation among age groups but slightly higher consumption of fruit in urban areas (Mutale and Chilengi 2018). Further work in urban Lusaka found differences between richer and poorer households, with a survey showing that 27% of richer but only 6% of poorer households eat fruits (largely citrus and locally-produced fruits) at least once per day, and that 23% of poorer and 9% of richer households never do; most households (64% of poorer and 71% of richer) eat vegetables (largely rape, chinese cabbage and indigenous vegetables) at least once per day, but 9% of each report never eating vegetables (World Food Programme 2018). Of protein sources, groundnuts and beans are most eaten, followed by fish, chicken, eggs, beef, and soya protein products, though again richer households consumed these more regularly; and 71% of households reported ever consuming dairy (largely liquid milk) (World Food Programme 2018).
Beyond dietary diversity, consumption of sugar and salt are tracked sporadically, as both are fortified with micronutrients in Zambia (vitamin A and iodine, respectively), and their use therefore implicitly promoted. In 2002, 45% of urban households and 14% of rural households had refined sugar present, while 64% of households owned iodized salt. More recently, the proportion of adults who ‘always or often add salt’ to their plate when eating was reported as around 40%, with average salt intake estimated at 10 g per day (very high) (Mutale and Chilengi 2018). In a recent study, 41% of urban Zambian children aged 6–23 months, and 14% of rural children, consumed sugary foods the previous day, at the higher end of the range for African countries studied (Huffman et al. 2014).
A 2017 survey among urban Lusaka households of varying socio-economic status found that ‘fast foods’ from international restaurant chains (particularly fried chicken or sausage and chips, as well as pizza and shawarma) are consumed ‘some days’ by 62% of the richest households, and never by 91% of poorest households; and that snack foods (particularly bread, scones, fritters, cookies and fried maize crisps) are consumed every day by 25% of the richest and never by 62% of the poorest households (World Food Programme 2018).
The World Food Programme (2018) report concludes that there is sufficient knowledge on healthy and unhealthy foods among urban households, though information was largely gained from family and friends as well as health personnel, radio and TV, and packaging labels, and poorer households found it harder to identify healthy foods. Major barriers to healthy foods were identified by respondents as cost-related; availability was less of an issue according to respondents, though many cited that after affordability, easy accessibility would encourage them to pick healthy foods, as well as ease of preparation and clear labelling. Around half of respondents in this study knew that too much salt would raise blood pressure.
9 Changing nutrition outcomes
Undernutrition remains the most prevalent nutrition issue in children both globally and in Africa, with 59 million children in the region (32% of children) stunted and 14 million (7%) wasted (UNICEF, WHO et al. 2017). As with other food and diet issues, undernutrition is related in part to wealth, with a study in eleven African cities finding approximately 15% of children amongst the richest households being stunted, compared with 35% amongst the poorest households (Frayne et al. 2014). In addition to stunting and wasting in children under five, deficiencies in micronutrients such as vitamin A, iron and iodine are commonly measured to be high in various populations, and deficiency in other nutrients that are rarely measured is likely to be a similar problem.
It is now well established that alongside undernutrition and micronutrient deficiency, low- and middle-income countries have an emerging problem of obesity, which tends to become evident first in the urban rich and in women when countries are at a lower level of wealth, but that as countries develop becomes an issue in the general population, and later largely a problem of the poor (Martorell et al. 2000). The nutrition profile is changing at a rapid pace in parts of Africa, with a review of seven countries in West and East Africa finding that the prevalence of urban overweight and obesity increased by nearly 35% between 1992 and 2005, with the increase higher among the poorer (50% rise) than the wealthier (7% rise) (Ziraba et al. 2009). A detailed study in South Africa similarly found that while the problem of underweight in children is more prevalent in rural areas, obesity is more serious in urban areas (Crush et al. 2011), but while overweight is highest in urban areas, the issue is increasing fastest in rural areas in many countries (Jaacks et al. 2015). Thus while the urban rich are setting the trend in these negative nutrition changes, the rural poor are not far behind, and catching up fast.
Chronic disease related to diet and nutrition is now a larger issue for adults than undernutrition in a majority of the world, with non-communicable diseases (NCDs) having become the leading cause of death globally, and over 75% of deaths from NCDs occurring in low- and middle-income countries (Imamura et al. 2015, Cook 2017). While levels of NCDs are still lower in poorer than richer countries, they have emerged in Africa at a faster rate and at a lower economic level than in industrialized countries (Vorster et al. 2011). Currently in Africa, the combined burden of NCDs is 21% of disability-adjusted life years.Footnote 7 Prevalence rates for type 2 diabetes mellitus and cardio-vascular disease in particular have seen a 10-fold increase in sub-Saharan Africa in the last 20 years (Amuna and Zotor 2008), and NCD deaths are projected to increase by 15% globally between 2010 and 2030, with a large proportion of increases occurring in Africa where they are expected to increase by more than 20% (WHO 2011). Indeed, in 2008, age-standardized NCD mortality rates were highest in the African region for females (724 per 100,000) and males (844 per 100,000) (WHO 2011). Finally, a typical feature of the nutrition transition is the coexistence of both maternal overweight and child malnutrition in the same household or community (Vorster et al. 2011), and this has become a feature of a significant number of SSA countries (Steyn and Mchiza 2014).
Mirroring the global and regional trends, Zambia has both a high (though decreasing) prevalence of stunting in children and a high (and increasing) prevalence of overweight and obesity in women (Fig. 10). Child stunting rose from 46% in 1992 to a high of over 50% of children in 2002, falling back to 40% in the most recent national survey. Micronutrient deficiencies are also found to be very prevalent, with a 2014 survey in two northern provinces finding that among women 98% are deficient in vitamin B12, 92% in folate, 55% in zinc, and 19% in iron; while in children 97% were deficient in vitamin B12, 84% in folate, up to 34% in zinc, and 26% in vitamin A (NFNC 2013).

Trends in selected nutrition-related outcomes. Source: DHS datasets 1992–2014; WHO STEPWISE studies 2007–8 and 2017–18
Child overweight has varied between 4 and 8% over the past decades. At the same time, overweight in women in urban areas has risen from 19.7% in 2002 (of whom 5.7% were obese), to 31.9% in 2014 (of whom 10.8 were obese); numbers were not disaggregated by rural/urban before 2002, but overall 10.6% of women nationally were overweight or obese in 1992. A recent study in urban Zambia found an average body mass index (BMI) of 22.5 in men and 24 in women, with 16% (3%) of males and 33% (12%) of females defined as overweight (obese) respectively (Mutale and Chilengi 2018). The same survey found around 45% of adults not engaging in in sufficient physical activity (including 35% who do not engage in vigorous activity at all), with women tending to be less active than men (Mutale and Chilengi 2018).
These changes in activity, diet and overweight are expected to accompany an increase in related NCDs such as hypertension and diabetes. A cross-sectional 2007 study suggested that these were already an issue among Lusaka’s urban middle class, with adult hypertension standing at 49% and glucose intolerance at 9% in this population (Goma et al. 2011, Yan et al. 2015) (Fig. 10). A recent follow-up to this survey shows raised blood pressure in around 20% of adults; high cholesterol in 5% of men and 10% of women; and glucose intolerance at 8% of men and 10% of women (Mutale and Chilengi 2018).
10 Discussion and conclusions
Our analyses in Zambia have focused on the period from the early 1990s to present, going back further where the available data would allow. This spans important decades in the nation’s history, from the introduction of sweeping liberal economic reforms in the country from 1991, through a time of increasing globalization of food systems - from primary production and processing to retail and preferences - that has not left Zambia or the region untouched. Our use of multiple sources of data, while limited in the kinds of analysis that may be performed, has illustrated that while Zambia may only be at the start of this transition, the changes predicted under the nutrition transition hypothesis are happening and should be acknowledged and addressed through food system policy.
A nutrition transition is occurring in Zambia, and has multiple dimensions. Urbanization and increasing incomes in some sections of the population are interacting with changing ways of sourcing food (in supermarkets and fast food restaurants), resulting in higher consumption of animal foods, fat, sugar, salt and highly processed foods – and leading to increases in overweight and chronic diseases in these populations. While change is happening more slowly in poorer and rural populations without the income and access of richer households, the increase in the price of fruits and vegetables and animal foods relative to staples is of concern, and dietary diversity measures along with food frequency surveys reveal a lack of these nutrient-dense foods in the diets of these populations.
Zambia’s nutrition transition is a story of inequality to the detriment of both ends of the spectrum, with hunger and deficiency persisting among the rural and urban poor, and overweight and NCDs emerging particularly among the urban rich but touching rural areas also. Persistently high levels of undernutrition in children and micronutrient deficiencies in women and children co-exist with moderately high and rapidly rising levels of overweight and obesity in women and significant levels of NCDs in adults, notably hypertension associated with salt use, creating a quadruple burden of malnutrition within the population.
The findings presented above indicate to a plausible extent that these changing nutrition outcomes are a reflection of changing diets in parts of the population, in particular richer urban residents. These diets are in turn built on changing household food expenditures, with an increasing proportion of expenditures of the urban rich spent on animal foods, fats, sugar and processed foods; and nutritious foods such as perishable fruits and vegetables as well as fish and eggs costing more over time in relation to staple foods. Food supply at a national level is broadly heading away from recommendations for diverse and healthy diets in terms of available foods, with many of the most nutritious foods less available per capita than they were in previous decades. Changing food sources for the urban rich, towards supermarket shopping and fast food outlets, are reflected in recent dietary data which shows highly processed snacks and fast foods common in the diet.
10.1 Study limitations and research needs
While this paper has been able to thread together important data on multiple stages of the food system and its relation to nutrition, there are some evident data gaps that limit our ability to research the nutrition transition both in Zambia and more broadly.
The first caveat with this work is that much of these data has known flaws, particularly the food balance sheet data that provides our understanding of food availability. This has been specifically questioned in Zambia because of its bearing on the very high undernourishment figures, which are rejected by the government.
Second, different foods or food groups are captured under each dataset for food availability, prices and expenditures. For many foods, the data for each capture a slightly different concept: for instance dried beans or pulses, or fruits and vegetables in different permutations. This limits our ability to link the data in useful ways. Although imperfect (and imperfectly linked), we do have data here on food production, prices, and expenditures, and nutrition and health outcomes, which add to our understanding of the Zambian food system.
Third, it will be useful to be able to tease out whether changes in household food expenditures are driven by change in prices, or change in amounts purchased. Economic surveys aiming to understand food systems should keep the distinction in mind.
Fourth, data were not collected over the same time periods for the same households, or the same foods or food groups, and often, particularly for diets and nutrition and health indicators, the data came from only one point in time. This provides indicative data, but these gaps should be followed up in subsequent work.
Fifth, what is missing in particular to join these findings up for the creation of relevant policy is data on the diets of individuals. Dietary intake data are needed for key population groups to link the food and nutrition stories, and data on differences between urban and rural, and richer and poorer groups. A pressing data gap in Zambia is the diets of urban citizens. Even better would be combining individual dietary data into datasets addressing upstream food expenditures and downstream nutrition outcomes.
Sixth, while the 2008 and 2018 WHO studies on chronic disease in Lusaka are welcome, further documentation of nutrition-related disease is needed, perhaps using clinical records where these are available to give a picture of the pace of change. DHS should continue to document overweight and obesity in women and children, to illustrate the pace of change and keep these dimensions of nutrition on the policy agenda.
Seventh, the role of ultra-processed foods in the nutrition transition is evident, and ultra-processed foods are now proposed as a marker for unhealthy diets. Data need to be collected on availability and intake of ultra-processed foods at different points along the food system (Monteiro et al. 2018).
Finally, nutrition transition work since the 1990s has focussed on the demographic and epidemiologic transitions, and has established that these are occurring as national economies and societies change. What remains to be fully integrated into these assessments is how our rapidly transitioning food systems are contributing to changes in diets and nutrition, so more characterization is needed of these in both richer and emerging economies, and the connections between them in a world of globalized food systems. It has been noted that the private sector might hold key data on many of the issues along the pathways to nutrition transition, albeit not at a standard for epidemiological or economic analyses, but useful and revealing nonetheless if these data can be harnessed.
10.2 Policy implications
The emerging changes in Zambia’s food system are not well reflected in current national food and nutrition policy, which maintains a focus on child stunting and micronutrient deficiencies as key outcomes, and on maize production as the key agricultural strategy (Harris et al. 2017). One implication of not addressing the nutrition transition is a negative impact in the near future on an already constrained national health budget.
Thankfully, the actions needed for averting undernutrition, overweight, micronutrient deficiencies and NCDs are similar, involving enhancing availability, affordability and desirability of diverse nutritious diets. Diet quality in Zambia needs to be tackled at both ends of the spectrum, increasing access to nutrient-rich foods and limiting consumption of nutrient-poor and ultra-processed foods. Joined-up food and nutrition policy that tackles both is warranted to limit the detrimental sides of Zambia’s nutrition transition.
On the supply side, action will involve promoting diversity in the production of nutrient-rich foods such as fruits, vegetables and pulses (beyond soya for animal feed or export), and supporting supply chains which make these accessible and affordable. This requires an agricultural transformation, characterised as systematic changes in farm production and food markets observed alongside economic development, seen at a similar stage of economic change to the nutrition transition (Masters et al. 2016). How to address the negative forces of globalization and commerce in a changing food landscape while maintaining the positive forces is still not fully understood, even in high-income countries which are further along the nutrition transition. But those involved in setting the nutrition agenda in Zambia should not ignore these broader structural and market influences on diet and nutrition change, both as a tool for leveraging action on undernutrition, and as important issues to address for the future of the Zambian health system and the health of the Zambian people.
On the demand side, this involves public health messages and increasing ‘nutrition literacy’ among all sections of the population. Some key messages about the negative effects of excess weight (and salt) will have to contend with different norms in Africa however, with higher social acceptability of overweight and obesity than is seen in many Western countries (Prentice 2006), and a desire for so-called ‘status’ or ‘aspirational’ foods - which may include processed foods and meat - as a powerful driver of food choices (Frayne et al. 2014).
A recent assessment of Zambia’s policy options for improving diet and nutrition concluded that as a low-income country with high urbanization and high market liberalization, the country should place high policy priority on incentivizing fruit and vegetable production, reducing ultra-processed foods, and tackling food safety issues; a medium priority on addressing the calorie shortfall and hunger issues, incentivizing animal source food production, and reducing sugar and salt intakes; and a lower priority on reducing intake of red meats and excess calories (Global Panel on Agriculture and Food Systems for Nutrition 2016). The analysis above, which brings significant national and regional detail to the food system determinants of nutrition transition in Zambia, would broadly agree with this assessment. Zambia needs to acknowledge its changing food environment in policy before poor nutrition outcomes become entrenched.
Notes
Konjunkturforschungsstelle (KOF) Globalization Index of the economic, social and political dimensions of globalization: http://globalization.kof.ethz.ch/media/filer_public/2016/03/03/rankings_2016.pdf
World Bank data, accessed May 2017. http://data.worldbank.org/indicator/NY.GDP.MKTP.KD.ZG?locations=ZM Gross Domestic Product (GDP) represents the sum of value added to an economy by all its producers. Growing GDP means an economy is gaining value. Average global GDP change has been between −1.7 and + 4.5 in the same period.
UNDP Human Development Report 2016. http://hdr.undp.org/en/content/income-gini-coefficient GINI coefficient is a measure of the deviation of the distribution of income among individuals or households within a country from a perfectly equal distribution. A value of 0 represents absolute equality, a value of 100 absolute inequality.
Figure derived from a review of supermarket websites
Food items were firstly identified as non-perishable (i.e., food items with a long shelf life such a maize grains or wheat), and perishable (i.e., food items with short shelf life such as fruits, vegetables, fresh meat, and fish). The food items were then identified by the processing level: unprocessed (e.g., whole maize grains, cassava, sweat potatoes, rice); low processing (processing that involves less value addition such as ground maize meal); and high processing (processing which involves much value addition such as breakfast cereals, beverages, and sugar).
References
Abrahams, C. (2009). Transforming the region: Supermarkets and the local food economy. African Affairs , 109(434), 115–134.
Abrahams, Z., Mchiza, Z., & Steyn, N. P. (2011). Diet and mortality rates in Sub-Saharan Africa: stages in the nutrition transition. BMC Public Health , 11(1), 801.
Amuna, P., & Zotor, F. B. (2008). Epidemiological and nutrition transition in developing countries: impact on human health and development: The epidemiological and nutrition transition in developing countries: evolving trends and their impact in public health and human development. Proceedings of the Nutrition Society , 67(1), 82–90.
Baker, P., & Friel, S. (2014). Processed foods and the nutrition transition: evidence from Asia. Obesity Reviews , 15(7), 564–577.
Berti, P. R. (2012). Intrahousehold distribution of food: a review of the literature and discussion of the implications for food fortification programs. Food and Nutrition Bulletin , 33(3_suppl2), S163–S169.
Bloem, S. & de Pee, S. (2017) Developing approaches to achieve adequate nutrition among urban populations requires an understanding of urban development. Global Food Security, 12: 80–99
Central Statistical Office, Ministry of Health, Tropical Diseases Research Centre, University of Zambia and Macro International Inc. (2014). Zambia Demographic and Health Survey 2013–14. Calverton: CSO and Macro International Inc..
Cirera, X., & Masset, E. (2010). Income distribution trends and future food demand. Philos Trans R Soc Lond B Biol Sci, 365(1554), 2821–34.
Chapoto, A., Haggblade, S., Hichaambwa, M., Kabwe, S., Longabaugh, S., Sitko, N., & Tschirley, D. (2012). Agricultural Transformation in Zambia: Alternative Institutional Models for Accelerating Agricultural Productivity Growth, and Commercialization (IAPRI working paper 064). Lusaka: IAPRI.
Chapoto, A., Zulu-Mbata, O., Hoffman, B. D., Kabaghe, C., Sitko, N., Kuteya, A., & Zulu, B. (2015). The Politics of Maize in Zambia: Who holds the Keys to Change the Status Quo? (IAPRI Working Paper 99). Lusaka: IAPRI.
Chicago Council on Global Affairs. (2011). Bringing Agriculture to the Table: How Agriculture and Food Can Play a Role in Preventing Chronic Disease. Chicago Council on Global Affairs: Chicago.
Chisanga, B., & Mbata-Zulu, O. (2017). The Changing Food Expenditure Patterns and Trends in Zambia: Implications on Agricultural Policies (Indaba Agricultural policy Research Institute Working Paper No. 119). Lusaka: IAPRI.
Cook, S. (2017). Nourishing diversity: A five-point plan to enrich our food systems (Hivos Briefing Paper). London: HIVOS and IIED.
Crush, J., & Frayne, B. (2011). Supermarket expansion and the informal food economy in Southern African cities: implications for urban food security. Journal of Southern African Studies, 37(4), 781–807.
Crush, J., Frayne, B., & McLachlan, M. (2011). Rapid urbanization and the nutrition transition in Southern Africa (Urban Food Security Series No. 7). Kingston and Cape Town: Queen’s University and AFSUN.
CSO. (2012). Zambia 2010 census of population and housing: National analytical report. Lusaka: CSO.
CSO. (2016). Living Conditions Monitoring Survey Report for 2015. Lusaka: CSO.
Dolislager, M. (2014). Diet Change in East and Southern Africa: Projecting Food Demand through 2040, Michigan State University.
Feeley, A., et al. (2009). Fast-food consumption among 17-year-olds in the Birth to Twenty cohort. South African Journal of Clinical Nutrition , 22(3), 118–123.
Frayne, B., Crush, J., & McLachlan, M. (2014). Urbanization, nutrition and development in Southern African cities. Food security , 6(1), 101–112.
Gillespie, S., & van den Bold, M. (2017a). Agriculture, Food Systems, and Nutrition: Meeting the Challenge. Global Challenges , 1(3), 1600002.
Gillespie, S. & van den Bold, M. (2017b). Agriculture, food systems, and nutrition: meeting the challenge. Global Challenges.
Global Panel on Agriculture and Food Systems for Nutrition. (2016). Food systems and diets: Facing the challenges of the 21st Century. London: Global Panel.
Goma, F. M., Nzala, S. H., Babaniyi, O., Songolo, P., Zyaambo, C., Rudatsikira, E., Siziya, S., & Muula, A. S. (2011). Prevalence of hypertension and its correlates in Lusaka urban district of Zambia: a population based survey. International Archives of Medicine. https://doi.org/10.1186/1755-7682-4-34.
Green, R., Cornelsen, L., Dangour, A. D, Turner, R., Shankar, B., Mazzocchi, M. & Smith, R. (2013). The effect of rising food prices on food consumption: Systematic review with meta-regression.
Haddad, L. J., C. Peña, C. Nishida, A. R. Quisumbing and A. T. Slack (1996). Food security and nutrition implications of intrahousehold bias, International Food Policy Research Institute (IFPRI).
Harris, J., Drimie, S., Roopnaraine, T., & Covic, N. (2017). From coherence towards commitment: Changes and challenges in Zambia's nutrition policy environment. Global Food Security , 13, 49–56.
Hassen, I. W., Dereje, M., Minten, B., & Hirvonen, K. (2016). Diet Transformation in Africa: The Case of Ethiopia (ESSP Working Paper No. 87). Washington, DC and Addis Ababa: International Food Policy Research Institute and Ethiopian Development Research Institute.
Hawkes, C. (2008). Dietary Implications of Supermarket Development: A Global Perspective. Development and Policy Review, 26(6), 657–692.
Herforth, A., & Ahmed, S. (2015). The food environment, its effects on dietary consumption, and potential for measurement within agriculture-nutrition interventions. Food Security , 7(3), 505–520.
Huffman, S. L., Piwoz, E. G., Vosti, S. A., & Dewey, K. G. (2014). Babies, soft drinks and snacks: a concern in low- and middle-income countries? Maternal & Child Nutrition , 10(4), 562–574.
IFPRI, Welthungerhilfe and Concern Worldwide (2017). Global Hunger Index: The inequalities of hunger. Global Hunger Index. Bonn, Washington DC, Dublin.
Imamura, F., Micha, R., Khatibzadeh, S., Fahimi, S., Shi, P., Powles, J., & Mozaffarian, D. (2015). Dietary quality among men and women in 187 countries in 1990 and 2010: a systematic assessment. The Lancet Global Health , 3(3), e132–e142.
Jaacks, L. M., Slining, M. M., & Popkin, B. M. (2015). Recent underweight and overweight trends by rural–urban residence among women in low- and middle-income countries. The Journal of Nutrition.
Jones, A. D. (2015). Household Food Insecurity is Associated with Heterogeneous Patterns of Diet Quality Across Urban and Rural Regions of Malawi. World Medical & Health Policy, 7(3), 234–254.
Kennedy, G., Nantel, G., & Shetty, P. (2004). Globalization of food systems in developing countries: a synthesis of country case studies (Globalization of food systems in developing countries: impact on food security and nutrition). FAO: Rome.
Martorell, R., Khan, L. K., Hughes, M. L., & Grummer-Strawn, L. M. (2000). Obesity in women from developing countries. European Journal of Clinical Nutrition , 54(3), 247–252.
Masters, W. A., Rosenblum, N. Z., Alemu, R. G., Fund, O. A. & Rubengera, R. (2016). Agricultural transformation, nutrition transition and food policy in Africa: Preston Curves reveal new stylized facts, Tufts University working paper.
Mehio Sibai, A., Nasreddine, L., Mokdad, A. H., Adra, N., Tabet, M., & Hwalla, N. (2010). Nutrition Transition and Cardiovascular Disease Risk Factors in Middle East and North Africa Countries: Reviewing the Evidence. Annals of Nutrition and Metabolism , 57(3–4), 193–203.
Miller, V., Yusuf, S., Chow, C. K., Dehghan, M., Corsi, D. J., Lock, K., Popkin, B., Rangarajan, S., Khatib, R., Lear, S. A., Mony, P., Kaur, M., Mohan, V., Vijayakumar, K., Gupta, R., Kruger, A., Tsolekile, L., Mohammadifard, N., Rahman, O., Rosengren, A., Avezum, A., Orlandini, A., Ismail, N., Lopez-Jaramillo, P., Yusufali, A., Karsidag, K., Iqbal, R., Chifamba, J., Oakley, S. M., Ariffin, F., Zatonska, K., Poirier, P., Wei, L., Jian, B., Hui, C., Xu, L., Xiulin, B., Teo, K., & Mente, A. (2016). Availability, affordability, and consumption of fruits and vegetables in 18 countries across income levels: findings from the Prospective Urban Rural Epidemiology (PURE) study. The Lancet Global Health , 4(10), e695–e703.
Misra, A., Singhal, N., Sivakumar, B., Bhagat, N., Jaiswal, A., & Khurana, L. (2011). Nutrition transition in India: secular trends in dietary intake and their relationship to diet- related non-communicable diseases. J Diabetes 3.
Monteiro, C. A., Cannon, G., Moubarac, J.-C., Levy, R. B., Louzada, M. L. C., & Jaime, P. C. (2018). The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutrition , 21(1), 5–17.
Monteiro, C. A., Levy, R. B., Claro, R. M., de Castro, I. R. R., & Cannon, G. (2010). Increasing consumption of ultra-processed foods and likely impact on human health: evidence from Brazil. Public Health Nutrition , 14(1), 5–13.
Mukuka, R. M., & Mofu, M. (2016). THe status of hunger and malnutrition in Zambia: A review of methods and indicators (IAPRI working paper: Draft). Lusaka: IAPRI.
Mulenga, C. (2013). T he state of food insecurity in Lusaka. Southern African Migration Programme: Zambia.
Mutale, W., & Chilengi, R. (2018). STEPS survey results for Zambia. Lusaka: World Health Organisation, Ministry of Health (Zambia), Central Statistical Office (Zambia).
Mwanamwenge, M., & Harris, J. (2017). Sustainable diets for all: Agriculture, food systems, diets and nutrition in Zambia. Lusaka: HIVOS and IIED.
NFNC. (2013). Micronutrient and Food Consumption Survey. UNICEF: Lusaka.
Nyirenda, D. B., Musukwa, M. & Mugode, R. H. (2007). The common Zambian foodstuff, ethnicity, preparation and nutritient composition of selected foods Ministry of Health, Zambia and Boston University, USA.
Pingali, P. (2004). Westernization of Asian Diets and the transformation of food systems: Implications for research and policy. ESA Working Paper No. 04–17. Rome, The Food and Agriculture Organization of the United Nations.
Popkin, B. (1994). The nutrition transition in low-income countries: an emerging crisis. Nutrition Reviews, 52(9), 285–298.
Popkin, B. M., Horton, S., Kim, S., Mahal, A., & Shuigao, J. (2001). Trends in diet, nutritional status, and diet-related noncommunicable diseases in China and India: the economic costs of the nutrition transition. Nutrition Reviews, 59(12), 379–390.
Potts, D. (2005). Counter-urbanisation on the Zambian copperbelt? Interpretations and implications. Urban Studies, 42(4), 583–609.
Prentice, A. M. (2006). The emerging epidemic of obesity in developing countries. International Journal of Epidemiology, 35(1), 93–99.
Reardon, T., Timmer, P., Barrett, C., & Berdegué, J. (2003). The Rise of Supermarkets in Africa, Asia, and Latin America. American Journal of Agricultural Economics, 85(5), 1140–1146.
Reardon, T., Tschirley, D., Minten, B., Haggblade, S., Liverpool-Tasie, S., Dolislager, M., Snyder, J., & Ijumba, C. (2015). Transformation of african agrifood systems in the new era of rapid urbanization and the emergence of a middle class. ReSAKSS Annual Conference “Beyond a Middle Income Africa”, Addis Ababa.
Richards, A. (1939). Land, Labour and Diet in Northern Rhodesia: An Economic Study of the Bemba Tribe. Oxford: Oxford University Press.
Rischke, R., Kimenju, S. C., Klasen, S., & Qaim, M. (2015). Supermarkets and food consumption patterns: The case of small towns in Kenya. Food Policy, 52, 9–21.
Ruel, M., J. Garrett and L. Haddad (2008). Rapid Urbanization and the Challenges of Obtaining Food and Nutrition Security. Nutrition and Health in Developing Countries (Second edition). R. Semba and M. Bloem. USA, Humana Press.
Ruel, M., Harris, J., & Cunningham, K. (2014). Measuring dietary quality in developing countries: A review of the usefulness of individual dietary diversity indicators. Diet Quality: An Evidence-Based Approach. V. R. Preedy. New York, Springer.
Steyn, N. P., Bradshaw, D., Norman, R., Joubert, J. D., Schneider, M., & Steyn, K. (2006). Dietary changes and the health transition in South Africa: implications for health policy (The double burden of malnutrition: Case studies from six developing countries). FAO: Rome.
Steyn, N. P., & Mchiza, Z. J. (2014). Obesity and the nutrition transition in Sub-Saharan Africa. Annals of the New York Academy of Sciences, 1311(1), 88–101.
Stuckler, D., McKee, M., Ebrahim, S., & Basu, S. (2012). Manufacturing epidemics: the role of global producers in increased consumption of unhealthy commodities including processed foods, alcohol, and tobacco. PLoS Medicine, 9(6), e1001235.
Thow, A. M., Jones, A., Hawkes, C., Ali, I., & Labonté, R. (2017). Nutrition labelling is a trade policy issue: lessons from an analysis of specific trade concerns at the World Trade Organization. Health Promotion International. https://doi.org/10.1093/heapro/daw109.
Tschirley, D., Reardon, T., Dolislager, M., & Snyder, J. (2015). The Rise of a Middle Class in East and Southern Africa: Implications for Food System Transformation. Journal of International Development, 27(5), 628–646.
UNICEF, WHO and The World Bank (2017). Joint child malnutrition estimates - Levels and trends in malnutrition.
UNIDO, T. U. N. I. D. O. (2013). Sustaining employment growth: the role of manufacturing and structural change. United Nations Industrial Development Organization Report. Geneva: United Nations.
Vorster, H. H., Kruger, A., & Margetts, B. M. (2011). The Nutrition Transition in Africa: Can It Be Steered into a More Positive Direction? Nutrients 3(4).
Weatherspoon, D. D., & Reardon, T. (2003). The rise of supermarkets in Africa: implications for agrifood systems and the rural poor. Development and Policy Review, 21(3), 333–355.
WHO. (2008). WHO STEPS chronic disease risk factor surveillance fact sheet. Lusaka: WHO.
WHO. (2011). Global status report on noncommunicable diseases 2010. Geneva: WHO.
Wilde, P. (1989). Changing Food Consumption Patterns in Sub-Saharan Africa. Washington, DC: USAIDFVA/PPM.
World Food Programme. (2018). Food Consumption Patterns in Lusaka: A Perception Survey. Lusaka: Consumer Unity Trust Society (CTS) & Scaling Up Nutrition (SUN) Business Network.
World Health Organisation. (2003). Diet, nutrition and the prevention of chronic diseases (WHO technical report series 916). Geneva: WHO.
Yan, L. D., Chi, B. H., Sindano, N., Bosomprah, S., Stringer, J. S., & Chilengi, R. (2015). Prevalence of hypertension and its treatment among adults presenting to primary health clinics in rural Zambia: analysis of an observational database. BMC Public Health. https://doi.org/10.1186/s12889-015-2258-4.
Ziraba, A. K., Fotso, J. C., & Ochako, R. (2009). Overweight and obesity in urban Africa: A problem of the rich or the poor? BMC Public Health, 9, 465.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest in the preparation of this paper.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Harris, J., Chisanga, B., Drimie, S. et al. Nutrition transition in Zambia: Changing food supply, food prices, household consumption, diet and nutrition outcomes. Food Sec. 11, 371–387 (2019). https://doi.org/10.1007/s12571-019-00903-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12571-019-00903-4