
Abstract
Purpose
The purpose of this study was to assess the relationship between 99mTc-MIBI and 99mTc-MDP bone scintigraphy and clinical or pathological variables, including preoperative serum PTH levels and tumor diameter, in patients with newly diagnosed PHPT.
Methods
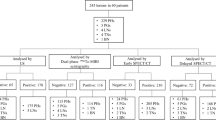
Dual-phase 99mTc-MIBI planar scintigraphy was performed in 244 patients with PHPT. Of these patients, 155 underwent 99mTc-MDP bone scintigraphy to detect bone changes before parathyroidectomy. Factors influencing 99mTc-MIBI scintigraphy and 99mTc-MDP bone scintigraphy detection rate were assessed using univariate and multivariate logistic regression analysis; optimal cutoff values for predicting positive 99mTc-MIBI and 99mTc-MDP bone scintigraphy were evaluated using ROC analysis.
Results
Among 244 patients, 174 (71.31 %) patients with 181 foci had a positive 99mTc-MIBI planar scintigraphy; delayed neck and thorax SPECT/CT could identify and locate the 99mTc-MIBI lesions but could not find more lesions than planar scintigraphy. 70 (28.69 %) patients had a negative 99mTc-MIBI planar scintigraphy. Tumor diameter, serum PTH level and symptoms were statistically significant predictive factors in predicting positive 9mTc-MIBI scintigraphy both univariate and multivariate logistic regression analyses. The optimal thresholds for tumor diameter and serum PTH by ROC analysis were 1.03 cm and 127.60 ng/L, respectively. Among 155 patients with bone scintigraphy, 99mTc-MDP bone scintigraphy showed positive finding in 80 (51.61 %) patients and negative finding in 75 patients. Univariate logistic regression analysis showed that patient age, sex, tumor diameter and PTH level (≥150 ng/L) were statistically significant in predicting positive 99mTc-MDP bone scintigraphy. Multivariate logistic regression analysis showed both tumor diameter and PTH ≥ 150 ng/L were statistically significant in predicting positive 99mTc-MDP bone scintigraphy. The optimal thresholds for tumor diameter and serum PTH by ROC analysis were 1.96 cm and 163.85 ng/L, respectively.
Conclusions
The utility of delayed neck and thorax SPECT/CT over dual-phase 99mTc-MIBI planar scintigraphy is that it can identify and locate a parathyroid tumor in about more than 70 % of patients in PHPT and provide the assistance for surgical planning. These studies also suggest that 99mTc-MIBI scintigraphy and 99mTc-MDP bone scintigraphy are closely correlated with tumor diameter and PTH; which may show negative results when tumor diameter is small and serum PTH level is low.



Similar content being viewed by others


References
Wermers RA, Khosla S, Atkinson EJ, Achenbach SJ, Oberg AL, et al. Incidence of primary hyperparathyroidism in Rochester, Minnesota, 1993–2001: an update on the changing epidemiology of the disease. J Bone Miner Res. 2006;21:171–7.
Mihai R, Wass JA, Sadler GP. Asymptomatic hyperparathyroidism—need for multicentre studies. Clin Endocrinol (Oxf). 2008;68:155–64.
Khan AA, Bilezikian JP, Potts JT Jr, Guest Editors for the Third International Workshop on Asymptomatic Primary Hyperparathyroidism. The diagnosis and management of asymptomatic primary hyperparathyroidism revisited. J Clin Endocrinol Metab. 2009;94:333–4.
Patten BM, Pages M. Severe neurological disease associated with hyperparathyroidism. Ann Neurol. 1984;15:453–6.
Silverberg SJ, Shane E, Jacobs TP, Siris E, Bilezikian JP. A 10-year prospective study of primary hyperparathyroidism with or without parathyroid surgery. N Engl J Med. 1999;341:1249–55.
Rubin MR, Bilezikian JP, McMahon DJ, Jacobs T, Shane E, Siris E, et al. The natural history of primary hyperparathyroidism with or without parathyroid surgery after 15 years. J Clin Endocrinol Metab. 2008;93:3462–70.
Lorberboym M, Minski I, Macadziob S, Nikolov G, Schachter P. Incremental diagnostic value of preoperative 99mTc-MIBI SPECT in patients with a parathyroid adenoma. J Nucl Med. 2003;44:904–8.
Neumann DR, Esselstyn CB, Maclntyre WJ, Go RT, Obuchowski NA, Chen EQ, et al. Comparison of FDG-PET and sestamibi-SPECT in primary hyperparathyroidism. J Nucl Med. 1996;37:1809–15.
Bhatnagar A, Vezza PR, Bryan JA, Atkins FB, Ziessman HA. Technetium-99m-sestamibi parathyroid scintigraphy: effect of P-glycoprotein, histology and tumor size on detectability. J Nucl Med. 1998;39:1617–20.
Im HJ, Lee IK, Paeng JC, Lee KE, Cheon GJ, Kang KW, et al. Functional evaluation of parathyroid adenoma using 99mTc-MIBI parathyroid SPECT/CT: correlation with functional markers and disease severity. Nucl Med Commun. 2014;35(6):649–54.
Cecchin D, Motta R, Zucchetta P, Bui F, Basso SM, Lumachi F. Imaging studies in hypercalcemia. Curr Med Chem. 2011;18:3485–93.
Delbeke D, Coleman RE, Guiberteau MJ, Brown ML, Royal HD, Siegel BA, Society of Nuclear Medicine (SNM), et al. Procedure guideline for SPECT/CT imaging 1.0. J Nucl Med. 2006;47:1227–34.
Kim YI, Jung YH, Hwang KT, Lee HY. Efficacy of mTc-sestamibi SPECT/CT for minimally invasive parathyroidectomy: comparative study with mTc-sestamibi scintigraphy, SPECT, US and CT. Ann Nucl Med. 2012;26:804–10.
Dasgupta DJ, Navalkissoor S, Ganatra R, Buscombe J. The role of single-photon emission computed tomography/computed tomography in localizing parathyroid adenoma. Nucl Med Commun. 2013;34:621–6.
Lavely WC, Goetze S, Friedman KP, Leal JP, Zhang Z, Garret-Mayer E, et al. Comparison of SPECT/CT, SPECT, and planar imaging with single- and dual-phase (99m)Tc-sestamibi parathyroid scintigraphy. J Nucl Med. 2007;48:1084–9.
Shafiei B, Hoseinzadeh S, Fotouhi F, Malek H, Azizi F, Jahed A, et al. Preoperative 99mTc-sestamibi scintigraphy in patients with primary hyperparathyroidism and concomitant nodular goiter: comparison of SPECT-CT, SPECT, and planar imaging. Nucl Med Commun. 2012;33:1070–6.
Phillips CD, Shatzkes DR. Imaging of the parathyroid glands. Semin Ultrasound CT MR. 2012;33:123–9.
Parikshak M, Castillo ED, Conrad MF, Talpos GB. Impact of hypercalcemia and parathyroid hormone level on the sensitivity of preoperative sestamibi scanning for primary hyperparathyroidism. Am Surg. 2003;69:393–8
Biertho LD, Kim C, Wu HS, Unger P, Inabnet WB. Relationship between sestamibi uptake, parathyroid hormone assay, and nuclear morphology in primary hyperparathyroidism. J Am Coll Surg. 2004;199:229–33.
Goldstein RE, Billheimer D, Martin WH, Richards K. Sestamibi scanning and minimally invasive radioguided parathyroidectomy without intraoperative parathyroid hormone measurement. Ann Surg. 2003;237:722–30.
Parel RJ, Bolton JS, Fuhrman GM. An analysis of sestamibi-positive versus -negative patients with primary hyperparathyroidism. Am Surg. 2001;67:1101–4.
Ciappuccini R, Morera J, Pascal P, Rame JP, Heutte N, Aide N, et al. Dual-phase 99mTc sestamibi scintigraphy with neck and thorax SPECT/CT in primary hyperparathyroidism: a single-institution experience. Clin Nucl Med. 2012;37:223–38.
Gotthardt M, Lohmann B, Behr TM, Bauhofer A, Franzius C, Schipper ML, et al. Clinical value of parathyroid scintigraphy with technetium-99 m methoxyisobutylisonitrile: discrepancies in clinical data and a systematic meta-analysis of the literature. World J Surg. 2004;28:100–7.
Author information
Authors and Affiliations
Corresponding author
Additional information
Zhong-Ling Qiu and Bo Wu contributed equally to this work.
Rights and permissions
About this article

Cite this article
Qiu, ZL., Wu, B., Shen, CT. et al. Dual-phase 99mTc-MIBI scintigraphy with delayed neck and thorax SPECT/CT and bone scintigraphy in patients with primary hyperparathyroidism: correlation with clinical or pathological variables. Ann Nucl Med 28, 725–735 (2014). https://doi.org/10.1007/s12149-014-0876-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-014-0876-z