
Opinion statement
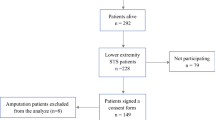
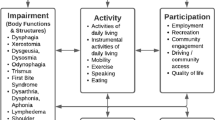
The current standard of care for soft tissue sarcoma (STS) is limb salvage surgery and adjuvant radiotherapy, with long-term survival rates of approximately 70%. However, the extensive surgical resection and subsequent reconstruction result in 50% of survivors living with chronic disability. Rehabilitation aims to optimize functional independence and quality of life, and is routinely offered to patients undergoing surgical treatment for STS. Unfortunately, there is a dearth of research related to rehabilitation in this area. We propose a model for assessing disability, for designing treatment interventions and for evaluating rehabilitative outcomes in STS. The World Health Organization’s (WHO) international classification of functioning, disability, and health (ICF) is divided into three domains: 1) impairments (related to body structure and function), 2) activity limitations (related to usual self-care activities/activities of daily living), and 3) participation restrictions (related to social roles). A literature review of STS rehabilitation reveals that most studies have focused on disability assessment, with few papers describing or evaluating rehabilitation interventions commonly employed in STS. Clinicians are forced to extrapolate findings from other patient populations in order to evaluate the effectiveness of specific rehabilitation strategies (ie, those used for particular sequelae of STS, such as lymphedema or impaired exercise tolerance). There is strongest support for complex decongestive physiotherapy (targeting lymphedema) and aerobic exercise interventions (aimed at alleviating cancerrelated fatigue and psychosocial sequelae). The most poorly researched topic is rehabilitation for genitourinary disability (both incontinence and sexual dysfunction). Most studies related to oncologic rehabilitation are restricted to the impairment level (eg, affecting range of motion, muscle strength) of the ICF, with only a small minority addressing activity limitations (eg, affecting activities of daily living) experienced by patients. A consideration of participation restrictions (eg, fulfillment of vocational roles) is almost wholly absent from the literature. Yet social role reintegration is of fundamental importance to patients. Further research is required in these two domains. The ICF provides a comprehensive framework for future research into rehabilitation interventions for STS.
Similar content being viewed by others

References and Recommended Reading
O’Sullivan B, Bell RS, Bramwell VHC: Sarcomas of the soft tissues. In Oxford Textbook of Oncology. Edited by Souhami R, Tannock I, Hohenberger P, Horiot J-C. Oxford: Oxford University Press, 2001:2495–2524.
Davis AM, O’Sullivan B, Bell RS, et al.: Function and health status outcomes in a randomized trial comparing preoperative and postoperative radiotherapy in extremity soft tissue sarcoma. J Clin Oncol 2002, 20:4472–4477.
Davis AM: Functional outcome in extremity soft tissue sarcoma. Seminars in Radiation Oncology 1999, 9:360–368.
World Health Organization: International Classification of Functioning, Disability, and Health. Geneva, Switzerland, 2001. This new WHO biopsychosocial classification system provides a comprehensive framework for evaluating rehabilitative outcomes. It integrates function from the level of the organ system all the way up to the individual’s social environment. It is applicable across the continuum of care.
World Health Organization: International Classification of Impairments, Disabilities and Handicaps. Geneva, Switzerland, 1980.
Davis AM, Sennik S, Griffin AM, et al.: Predictors of functional outcomes following limb salvage surgery for lower-extremity soft tissue sarcoma. J Surg Oncol 2000, 73:206–211.
Beck LA: Cancer rehabilitation: does it make a difference? Rehabilitation Nursing 2003, 28:42–47.
Gerber L, Hicks J, Klaiman M, et al.: Rehabilitation of the cancer patient. In Cancer: Principles and Practice of Oncology. Editors De Vita VT, Hellman S, Rosenberg SA. Philadelphia: Lippincott-Raven Publishers, 1997:2925–2955.
Gudas SA: Shoulder rehabilitation in cancer patients. Rehabil Oncol 2000, 18:23–28.
American Cancer Society: Returning to work after cancer treatment: American Cancer Society, http:// www.cancer.org/docroot/NWS/content/NWS_1_1x_ Returning_to_Work_after_Cancer_Treatment.asp, 2000.
Brown A, Parsons JA, Martino C, et al.: Work status following distal femoral Kotz reconstruction for malignant tumors of bone. Arch Phys Med Rehabil 2003, 84:62–68.
Verbeek J, Spelten E, Kammeijer M, Sprangers M: Return to work of cancer survivors: a prospective cohort study into the quality of rehabilitation by occupational physicians. Occup Environ Med 2003, 60:352–361.
Enneking WF: Modification of the system for functional evaluation in the surgical management of musculoskeletal tumors. In Limb Salvage in Musculoskeletal Oncology. Edited by Enneking WF. New York: Churchill Livingstone, 1987:626–639.
Enneking WF, Dunham W, Gebhardt MC, et al.: A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin Orthop 1993, 286
Lane JM, Christ GH, Khan SN, Backus SI: Rehabilitation for limb salvage patients. Cancer 2001, 92:1013–1019.
Lampert MH, Gerber LH, Glatstein E, et al.: Soft tissue sarcoma: functional outcome after wide local excision and radiation therapy. Arch Phys Med Rehabil 1984, 65:477–480.
Cheng P-T, Lin Y-H, Hao S-P, Yeh AR: Objective comparison of shoulder dysfunction after three neck dissection techniques. Ann Otol Rhinol Laryngol 2000, 109:761–766.
Mock V: Fatigue management: evidence and guidelines for practice. Cancer 2001, 92:1699–1707.
Dimeo FC, Stieglitz R-D, Novelli-Fischer U, et al.: Effects of physical activity on the fatigue and psychologic status of cancer patients during chemotherapy. Cancer 1999, 85:2273–2277.
Holley S: Cancer-related fatigue: suffering a different fatigue. Cancer Pract 2000, 8:87–95.
Holley S, Borger D: Energy for living with cancer: preliminary findings of a cancer rehabilitation group intervention study. Oncol Nurs Forum 2001, 28:1393–1396.
Miaskowski C, Lee KA: Pain, fatigue, and sleep disturbances in oncology outpatients receiving radiation therapy for bone metastasis: a pilot study. J Pain Symptom Manage 1999, 17:320–332.
Cheville AL, McGarvey CL, Petrek JA, et al.: Lymphedema management. Semin Radiat Oncol 2003, 13:290–301. This excellent review analyzes the results of numerous studies of lymphedema management and provides strong evidence supporting CDP as the preferred treatment option.
Leduc O, Leduc A, Bourgeois P, Belgrado J-P: The physical treatment of upper limb edema. Cancer 1998, 83:2835–2839.
Piso DU, Eckardt A, Liebermann A, et al.: Early rehabilitation of head-neck edema after curative surgery for orofacial tumors. Am J Phys Med Rehabil 2001, 80:261–269.
Ko DSC, Lerner R, Klose G, Cosimi AB: Effective treatment of lymphedema of the extremities. Arch Surg 1998, 133:452–457.
Drouin J, Pfalzer LA: Aerobic exercise guidelines for the person with cancer. Acute Care Perspect 2001, 10:18–24.
Pinto BM, Maruyama NC: Exercise in the rehabilitation of breast cancer survivors. Psychooncology 1999, 8:191–206.
Dimeo F, Stieglitz R-D, Novelli-Fischer U, et al.: Correlation between physical performance and fatigue in cancer patients. Ann Oncol 1997, 8:1251–1255.
Segal R, Evans W, Johnson D, et al.: Structured exercise improves physical functioning in women with stages I and II breast cancer: result of a randomized controlled trial. J Clin Oncol 2001, 19:657–665.
MacVicar MG, Winningham ML, Nickel JL: Effects of aerobic interval training on cancer patients’ functional capacity. Nurs Res 1989, 38:348–351.
Courneya KS, Friedenreich CM: Determinants of exercise during colorectal cancer treatment: an application of the theory of planned behavior. Oncol Nurs Forum 1997, 24:1715–1723.
Guyatt GH, et al.: The 6-minute walk test: a new measure of exercise capacity in patients with chronic heart failure. Can Med Assoc J 1985, 132:919–923.
CourneyaKS, Friedenreich CM: Relationship between exercise pattern across the cancer experience and current quality of life in colorectal cancer survivors. J Altern Complement Med 1997, 3:215–226. The collected works of Courneya, Friedenreich, and colleagues have been some of the most comprehensive in evaluating oncology rehabilitation interventions and provides an excellent model for research in other areas; address issues of participation and importance of premorbid social roles.
van Kampen M, de Weerdt W, van Poppel H, et al.: Effect of pelvic-floor re-education on duration and degree of incontinence after radical prostatectomy: a randomized controlled trial. Lancet 2000, 355:91–98.
Gallo-Silver L: The sexual rehabilitation of persons with cancer. Cancer 2000, 8:10–15.
Fialka-Moser V, Crevenna R, Korpan M, Quittan M: Cancer rehabilitation: Particularly with aspects on physical impairments. J Rehab Med 2003, 35:153–162.
Sheard T, Maguire P: The effect of psychological interventions on anxiety and depression in cancer patients: results of two meta-analyses. Br J Cancer 1999, 80:1770–1780. Important summary of two meta-analyses into the important area of psychosocial sequelae of cancer; reports effect sizes and facilitates clinician judgment regarding the most appropriate treatment interventions.
Courneya KS, Keats MR, Turner AR: Physical exercise and quality of life in cancer patients following high dose chemotherapy and autologous bone marrow transplantation. Psychooncology 2000, 9:127–136.
Aaronson NK, Ahmedzai S, Bergman B, et al.: The European Organization for the Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993, 85:365–376.
Ware JE, Kosinski M, Keller SD: SF-36 Physical and Mental Health Summary Scales: A User’s Manual. Boston: Health Assessment Lab, New England Medical Centre, 1994.
Davis AM, Bell RS, Badley EM, et al.: Evaluating functional outcome in patients with lower extremity sarcoma. Clin Orthop 1999, 358:90–100.
Passik SD, McDonald MV: Psychosocial aspects of upper extremity lymphedema in women treated for breast carcinoma. Cancer 1998, 83:2817–2820.
Rinehart-Ayres ME: Conservative approaches to lymphedema treatment. Cancer 1998, 83:2828–2832.
Harris SR, Hugi MR, Olivotto IA, et al.: Upper extremity rehabilitation in women with breast cancer after axillary dissection: clinical practice guidelines. Can Med Assoc J 2001, 13:91–103.
Young-McCaughan S, Mays MZ, Arzola SM, et al.: Change in exercise tolerance, activity and sleep patterns, and quality of life in patients with cancer participating in a structured exercise program. Oncol Nurs Forum 2003, 30:441–452.
Engstrom CA, Strohl RA, Rose L, et al.: Sleep alterations in cancer patients. Cancer Nurs 1999, 22:143–148.
Schwartz AL: Patterns of exercise and fatigue in physically active cancer survivors. Oncol Nurs Forum 1998, 25:485–491.
Brennan MJ, Miller LT: Overview of treatment options and review of the current role and use of compression garments, intermittent pumps, and exercise in the management of lymphedema. Cancer 1998, 83:2821–2827.
Petersson L-M, Berglund G, Brodin O, et al.: Group rehabilitation for cancer patients: satisfaction and perceived benefits. Patient Educ Couns 2000, 40:219–229.
Keus RB, Rutgers EJT, Ho GH, et al.: Limb-sparing therapy of extremity soft tissue sarcomas: treatment outcomes and long-term functional results. Euro J Cancer 1994, 30:1459–1463.
Colterjohn NR, Davis AM, O’Sullivan B, et al.: Functional outcome in limb-salvage surgery for soft tissue tumors of the foot and ankle. Sarcoma 1997, 1:67–74.
Serletti JM, Carras AJ, O’keefe RJ, Rosier RN: Functional outcome after soft tissue reconstruction for limb salvage after sarcoma surgery. Plast Reconstr Surg 1998, 102:1576–1583.
Monga U, Jaweed M, Kerrigan AJ, et al.: Neuromuscular fatigue in prostate cancer patients undergoing radiotherapy. Arch Phys Med Rehabil 1997, 78:961–966.
Andrykowski MA, Carpenter JS, Greiner CB, et al.: Energy level and sleep quality following bone marrow transplantation. Bone Marrow Transplant 1997, 20:669–679.
Ardies CM: Exercise, cachexia, and cancer therapy: a molecular rationale. Nutr Cancer 2002, 42:143–157.
Ganz PA, Rowland JH, Desmond K, et al.: Life after breast cancer: understanding women’s health-related quality of life and sexual functioning. J Clin Oncol 1998, 16:501–514.
Schover LR: Sexual rehabilitation after treatment for prostate cancer. Cancer 1993, 71:1024–1030.
Passik SD, Newman M, Brennan M, Tunkel R: Predictors of psychological distress, sexual dysfunction, and physical functioning among women with upper extremity lymphedema related to breast cancer. Psychooncology 1995, 4:255–263.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Parsons, J.A., Davis, A.M. Rehabilitation and quality-of-life issues in patients with extremity soft tissue sarcoma. Curr. Treat. Options in Oncol. 5, 477–488 (2004). https://doi.org/10.1007/s11864-004-0036-0
Issue Date:
DOI: https://doi.org/10.1007/s11864-004-0036-0