Abstract
Purpose
Curative lobectomy and systematic lymph node dissection for lung cancer in elderly patients are often associated with increased risk of postoperative morbidity and decreased quality of life. Conversely, avoiding surgery may mean not curing the cancer. We retrospectively examined data on surgery for octogenarians with clinical stage I non-small-cell lung cancer (NSCLC) to assess the safety and prognosis for patients who underwent radical or limited surgery.
Methods
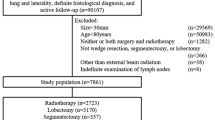
Subjects comprised 44 octogenarians who underwent surgery for clinical stage I NSCLC from 1996 to 2008. Preoperative co-morbidities, surgical procedures, postoperative morbidity, and prognoses were compared between radical and limited surgery.
Results
A total of 14 patients (32%) underwent complete lobectomy and systematic lymph node dissection (radical surgery), and 30 patients (68%) underwent segmentectomy or wedge resection or limited lymph node dissection (limited surgery). No significant differences in preoperative clinicopathological features were seen between groups except that significantly more clinical stage IA patients were in the limited surgery group than in the radical group. Surgical time was significantly shorter with limited surgery. Frequencies of postoperative morbidity and recurrence were similar for each type of surgery. Overall and disease-specific 5-year survival rates did not differ significantly between groups.
Conclusion
Limited surgery is less invasive and is associated with the same prognosis as radical surgery for octogenarians with NSCLC. Limited surgery for this cohort thus appears reasonable to prevent postoperative morbidity, particularly for patients with poor pulmonary reserve.
Similar content being viewed by others


References
Matsuoka H, Okada M, Sakamoto T, Tsubota N. Complications and outcomes after pulmonary resection for cancer in patients 80 to 89 years of age. Eur J Cardiothorac Surg 2005;28:380–383.
Aoki T, Yamato Y, Tsuchida M, Watanabe T, Hayashi J, Hirono T. Pulmonary complications after surgical treatment of lung cancer in octogenarians. Eur J Cardiothorac Surg 2000;18:662–665.
Pagni S, Federico JA, Ponn RB. Pulmonary resection for lung cancer in octogenarians. Ann Thorac Surg 1997;63:785–789.
Ginsberg R, Rubinstein LV, Lung Cancer Study Group. Randomized trial of lobectomy versus limited resection for T1N0 non-small cell lung carcinoma. Ann Thorac Surg 1995;60:615–623.
Mery CM, Pappas AN, Bueno R, Colson YL, Linden P, Sugarbaker DJ, et al. Similar long-term survival of elderly patients with non-small cell lung cancer treated with lobectomy or wedge resection within the surveillance, epidemiology and end results database. Chest 2005;128:237–245.
Mountain CF. Revisions in the international system for staging lung cancer. Chest 1997;111:1710–1717.
Ikeda N, Hayashi A, Iwasaki K, Kajiwara N, Uchida O, Kato H. Surgical strategy for non-small cell lung cancer in octogenarians. Respirology 2007;12:712–718.
Jaklitsch MT, Mery CM, Audisio RA. The use of surgery to treat lung cancer in elderly patients. Lancet Oncol 2003;4:463–471.
Aoki T, Tsuchida T, Watanabe T, Hashimoto T, Koike T, Hirono T, et al. Surgical strategy for clinical stage I non-small cell lung cancer in octogenarians. Eur J Cardiothorac Surg 2003;23:446–450.
Jensik RJ, Faber LP, Milloy FJ, Monson DO. Segmental resection for lung cancer: a fifteen-year experience. J Thorac Cardiovasc Surg 1973;66:563–572.
Bennett WF, Smith RA. Segmental resection for bronchogenic carcinoma: a surgical alternative for the compromised patient. Ann Thorac Surg 1979;27:169–172.
Hoffman TH, Ransdell HT. Comparison of lobectomy and wedge resection for carcinoma of the lung. J Thorac Cardiovasc Surg 1980;79:211–217.
Jacobson MJ, Zand L, Fox RT, Less W. A comparison of wedge and segmental resection of the lung. Thorax 1976;31:365–368.
Koike T, Yamato Y, Yoshiya K, Shimoyama T, Suzuki R. Intentional limited pulmonary resection for peripheral T1 N0 M0 small-sized lung cancer. J Thorac Cardiovasc Surg 2003;125:924–928.
Okada M, Koike T, Higashiyama M, Yamato Y, Kodama K, Tsubota N. Radical sublobar resection for small-sized nonsmall cell lung cancer: a multicenter study. J Thorac Cardiovasc Surg 2006;132:769–775.
Sugi K, Kobayashi S, Sudou M, Sakano H, Matsuda E, Okabe K. Long-term prognosis of video-assisted limited surgery for early lung cancer. Eur J Cardiothorac Surg 2010;37:456–460.
Wright G, Manser RL, Byrnes G, Hart D, Campbell DA. Surgery for non-small cell lung cancer: systematic review and meta-analysis of randomized controlled trials. Thorax 2006;61:597–603.
Wu Y, Huang ZF, Wang SY, Yang XN, Ou W. A randomized trial of systematic nodal dissection in resectable non-small cell lung cancer. Lung Cancer 2002;36:1–6.
Iwasaki A, Hamatake D, Hamanaka W, Hamada T, Shirakusa S, Yamamoto S, et al. Is systemic node dissection for accuracy staging in clinical stage I non-small cell lung cancer worthwhile in the elderly? Thorac Cardiov Surg 2008;56:37–41.
Yasufuku K, Nakajima T, Motoori K, Sekine Y, Shibuya K, Hiroshima K, et al. Comparison of endobronchial ultrasound, positron emission tomography, and CT for lymph node staging of lung cancer. Chest 2006;130:710–718.
Yasufuku K, Chiyo M, Koh E, Moriya Y, Iyoda A, Sekine Y, et al. Endobronchial ultrasound guided transbronchial needle aspiration for staging of lung cancer. Lung Cancer 2005;50:347–354.
Rodin MB, Mohile SG. A practical approach to geriatric assessment in oncology. J Clin Oncol 2007;25:1936–1944.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Okada, A., Hirono, T. & Watanabe, T. Safety and prognosis of limited surgery for octogenarians with non-small-cell lung cancer. Gen Thorac Cardiovasc Surg 60, 97–103 (2012). https://doi.org/10.1007/s11748-011-0880-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-011-0880-3