
Abstract
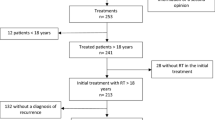
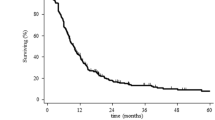
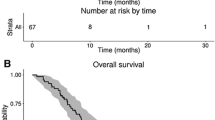
The optimal treatment for patients with recurrent high grade glioma (HGG) remains controversial. Available therapies include surgery, re-irradiation, alternating electric fields or systemic therapy. Here we investigate whether re-resection will improve survival in patients receiving repeat radiotherapy for tumor recurrence. 231 consecutive patients with recurrent HGG treated with re-irradiation between 1994 and 2012 were analyzed. 105 patients underwent re-resection. Re-irradiation was delivered using daily fractions of 3.5 Gy to a median total dose of 35 Gy. Survival was then analyzed comparing patients with and without re-resection. Overall survival (OS) and survival from the first recurrence are reported. Univariate and cox-proportional hazard modeling was performed in a step-wise multivariate analysis using known prognostic factors. The median follow-up time from initial diagnosis was 25.7 months. The median OS from initial diagnosis of the entire group was 22.5 months. There was no significant difference in median overall survival between patients who received re-resection versus no re-resection, 23 versus 21.9 months respectively (p = 0.6). Additionally, there was no difference in median survival from the time of first recurrence 10.5 months without re-resection versus 11.1 months with re-resection (p = 0.09). After adjusting for known prognostic variables, only age remained significant. Re-irradiation is an effective salvage therapy for patients with localized, progressive high grade glioma, achieving a median survival of 10–11 months from re-irradiation. Our data reveals no significant improvement in survival with the addition of re-resection to re-irradiated patients with HGG.


Similar content being viewed by others
References
Ostrom QT, Gittleman H, Farah P, Ondracek A, Chen Y, Wolinsky Y, Stroup NE, Kruchko C, Barnholtz-Sloan JS (2013) CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2006-2010. Neuro-Onco. doi:10.1093/neuonc/not151
Salcman M (1980) Survival in glioblastoma: historical perspective. Neurosurgery 7:435–439
Gilbert MR, Dignam JJ, Armstrong TS et al (2014) A randomized trial of bevacizumab for newly diagnosed glioblastoma. N Engl J Med 370:699–708
Barbagallo GMV, Jenkinson MD, Brodbelt AR (2008) “Recurrent” glioblastoma multiforme, when should we reoperate? Br J Neurosurg 22:452–455
Stupp R, Brada M, van den Bent MJ, Tonn J-C, Pentheroudakis G, on behalf of the ESMO Guidelines Working Group (2014) High-grade glioma: eSMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol Off J Eur Soc Med Oncol ESMO. doi:10.1093/annonc/mdu050
Gorlia T, Stupp R, Brandes AA et al (2012) New prognostic factors and calculators for outcome prediction in patients with recurrent glioblastoma: a pooled analysis of EORTC brain tumour group phase I and II clinical trials. Eur J Cancer Oxf Engl 48:1176–1184
Clarke JL, Ennis MM, Yung WKA et al (2011) Is surgery at progression a prognostic marker for improved 6-month progression-free survival or overall survival for patients with recurrent glioblastoma? Neuro-Oncol 13:1118–1124
Mann BS (2014) Overall survival benefit from surgical resection in treatment of recurrent glioblastoma. Ann Oncol Off J Eur Soc Med Oncol ESMO. doi:10.1093/annonc/mdu243
Bloch O, Han SJ, Cha S, Sun MZ, Aghi MK, McDermott MW, Berger MS, Parsa AT (2012) Impact of extent of resection for recurrent glioblastoma on overall survival: clinical article. J Neurosurg 117:1032–1038
Oppenlander ME, Wolf AB, Snyder LA et al (2014) An extent of resection threshold for recurrent glioblastoma and its risk for neurological morbidity. J Neurosurg 120:846–853
Quick J, Gessler F, Dützmann S, Hattingen E, Harter PN, Weise LM, Franz K, Seifert V, Senft C (2014) Benefit of tumor resection for recurrent glioblastoma. J Neurooncol 117:365–372
Park JK, Hodges T, Arko L et al (2010) Scale to predict survival after surgery for recurrent glioblastoma multiforme. J Clin Oncol Off J Am Soc Clin Oncol 28:3838–3843
Fogh SE, Andrews DW, Glass J et al (2010) Hypofractionated stereotactic radiation therapy: an effective therapy for recurrent high-grade gliomas. J Clin Oncol Off J Am Soc Clin Oncol 28:3048–3053
Macdonald DR, Cascino TL, Schold SC, Cairncross JG (1990) Response criteria for phase II studies of supratentorial malignant glioma. J Clin Oncol Off J Am Soc Clin Oncol 8:1277–1280
Wen PY, Macdonald DR, Reardon DA et al (2010) Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J Clin Oncol Off J Am Soc Clin Oncol 28:1963–1972
Stupp R, Hegi ME, Mason WP et al (2009) Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol 10:459–466
Daneyemez M, Gezen F, Canakçi Z, Kahraman S (1998) Radical surgery and reoperation in supratentorial malignant glial tumors. Minim Invasive Neurosurg MIN 41:209–213
Helseth R, Helseth E, Johannesen TB, Langberg CW, Lote K, Rønning P, Scheie D, Vik A, Meling TR (2010) Overall survival, prognostic factors, and repeated surgery in a consecutive series of 516 patients with glioblastoma multiforme. Acta Neurol Scand 122:159–167
Guyotat J, Signorelli F, Frappaz D, Madarassy G, Ricci AC, Bret P (2000) Is reoperation for recurrence of glioblastoma justified? Oncol Rep 7:899–904
Ryken TC, Kalkanis SN, Buatti JM, Olson JJ (2014) The role of cytoreductive surgery in the management of progressive glioblastoma : a systematic review and evidence-based clinical practice guideline. J Neurooncol 118:479–488
Weller M, van den Bent M, Hopkins K et al (2014) EANO guideline for the diagnosis and treatment of anaplastic gliomas and glioblastoma. Lancet Oncol 15:e395–e403
Skeie BS, Enger PØ, Brøgger J, Ganz JC, Thorsen F, Heggdal JI, Pedersen P-H (2012) γ knife surgery versus reoperation for recurrent glioblastoma multiforme. World Neurosurg 78:658–669
Lederman G, Wronski M, Arbit E, Odaimi M, Wertheim S, Lombardi E, Wrzolek M (2000) Treatment of recurrent glioblastoma multiforme using fractionated stereotactic radiosurgery and concurrent paclitaxel. Am J Clin Oncol 23:155–159
Combs SE, Thilmann C, Edler L, Debus J, Schulz-Ertner D (2005) Efficacy of fractionated stereotactic reirradiation in recurrent gliomas: long-term results in 172 patients treated in a single institution. J Clin Oncol Off J Am Soc Clin Oncol 23:8863–8869
Fokas E, Wacker U, Gross MW, Henzel M, Encheva E, Engenhart-Cabillic R (2009) Hypofractionated stereotactic reirradiation of recurrent glioblastomas : a beneficial treatment option after high-dose radiotherapy? Strahlenther Onkol Organ Dtsch Röntgenges Al 185:235–240
Minniti G, Armosini V, Salvati M, Lanzetta G, Caporello P, Mei M, Osti MF, Maurizi RE (2011) Fractionated stereotactic reirradiation and concurrent temozolomide in patients with recurrent glioblastoma. J Neurooncol 103:683–691
Hudes RS, Corn BW, Werner-Wasik M, Andrews D, Rosenstock J, Thoron L, Downes B, Curran WJ (1999) A phase I dose escalation study of hypofractionated stereotactic radiotherapy as salvage therapy for persistent or recurrent malignant glioma. Int J Radiat Oncol Biol Phys 43:293–298
Taal W, Oosterkamp HM, Walenkamp AME et al (2014) Single-agent bevacizumab or lomustine versus a combination of bevacizumab plus lomustine in patients with recurrent glioblastoma (BELOB trial): a randomised controlled phase 2 trial. Lancet Oncol. doi:10.1016/S1470-2045(14)70314-6
Conflict of interest
None.
Disclosures
This work was presented in part as a digital poster at the 2013 American Society of Therapeutic Radiation Oncologists (ASTRO) annual meeting in Atlanta, Georgia September 22-25, 2013.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Palmer, J.D., Siglin, J., Yamoah, K. et al. Re-resection for recurrent high-grade glioma in the setting of re-irradiation: more is not always better. J Neurooncol 124, 215–221 (2015). https://doi.org/10.1007/s11060-015-1825-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-015-1825-y