
Abstract
Background
The endoscopy unit before remediation may be a high-risk area for slip and fall injuries due to a large number of exposed above-the-floor wires in the endoscopy rooms, dimmed lighting during endoscopic procedures, and staff inattention to obstacles due to preoccupation with the endoscopic patient.
Aim
To describe a novel, previously unappreciated workplace hazard to endoscopic personnel: Exposed wires in the endoscopy unit.
Methods
This study is a retrospective review of 110,000 endoscopic procedures performed during the last 5 years at an academic, teaching hospital with a high-volume endoscopy unit. All significant orthopedic injuries to endoscopic personnel from slips, twists, and falls from tripping over exposed cords in the endoscopy unit were reviewed. The severity of injury was documented based on roentgenographic findings, number of days of missed work, number of days with a modified work schedule, and requirement for orthopedic surgery. The number of potentially exposed cords per endoscopy room was determined.
Results
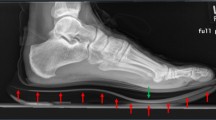
During the 5-year study period, three endoscopic personnel suffered significant orthopedic injuries from slips, twists, and falls from tripping over cords, wires, or tubing lying exposed over the floor in the endoscopy suite: The resulting injuries consisted of fourth and fifth metacarpal hand fractures due to a fall after tripping on oxygen tubing; a rib fracture due to tripping on electrical wires trailing from an endoscopy cart; and a grade II ankle sprain due to the foot becoming entangled in oxygen tubing. All injuries resulted in lost days of work [mean 9.3 ± 11.0 (SD) days] and in additional days of restricted work (mean 41.7 ± 31.8 days). One injury required orthopedic surgery. Hospital review revealed a mean of 35.3 ± 7.5 cords, wires, or tubing per endoscopy procedure room, the majority of which were exposed above the floor before remediation (n = 10 rooms). Remediation of exposed wires included: bundling related wires together in a cable to reduce the number of independent wires, covering exposed wires on the floor with a nonslip heavy mat, and running wires from ceiling outlets to equipment high above ground (e.g. mounted endoscopy video monitors).
Conclusions
Tripping, slipping, and falling over exposed wires can cause significant injury to endoscopic personnel. This previously undescribed hazard should be preventable by simple remediation, and all endoscopic personnel, hospital architects, hospital administrators, and governmental regulators should be alerted to this potential hazard

Similar content being viewed by others


Notes
Cords, wires, and tubing: (1) in all ten rooms included those for the main endoscopic television monitor, endoscopy cart, endoscope water pump, supplemental oxygen, wall vacuum, intravenous line, blood pressure cuff, electrocardiographic leads, and pulse oximetry; (2) in eight rooms for the auxiliary endoscopic television monitor; (3) in one (ERCP) room for the portable X-ray machine, fluoroscopy display monitor, electrically powered ERCP stretcher, and anesthesia gas machine. In all ten rooms, an additional 11.3 + 1.1 wires were easily embedded in the wall and are not included in the above total. These wires were for telephone jacks, computer, computer monitor, keyboard, mouse, and X-ray view box (Fig. 1c).
References
Cappell MS. Colonoscopist’s thumb: DeQuervain’s syndrome (tenosynovitis of the left thumb) associated with overuse during endoscopy. Gastrointest Endosc. 2006;64(5):841–843.
Buschbacher R. Overuse syndromes among endoscopists. Endoscopy. 1994;26(6):539–544.
Hansel SL, Crowell MD, Pardi DS, Bouras EP, Dibaise JK. Prevalence and impact of musculoskeletal injury among endoscopists: a controlled pilot study. J Clin Gastroenterol. 2009;43(5):399–404.
Keate RF, Drden GW, Wang K, Chen YK, et al. Occupational injuries to endoscopists: report from the ASGE web survey. Abstract S1450. Gastrointest Endosc. 2006;63(5):111.
Liberman AS, Shrier I, Gordon PH. Injuries sustained by colorectal surgeons performing colonoscopy. Surg Endosc. 2005;19(12):1606–1609.
Shergill AK, Asundi KR, Barr A, et al. Pinch force and forearm-muscle load during routine colonoscopy: a pilot study. Gastrointest Endosc. 2009;69(1):142–146.
Seeff LC, Richards TB, Shapiro JA, et al. How many endoscopies are performed for colorectal cancer screening? results from CDC’s survey of endoscopic capacity. Gastroenterology. 2004;127(6):1670–1677.
Stevens M, Holman CD, Bennett N. Preventing falls in older people: impact of an intervention to reduce environmental hazards in the home. Am Geriatr Soc. 2001;49(11):1442–1447.
Bentley TA, Haslam RA. Identification of risk factors and countermeasures for slip, trip and fall accidents during the delivery of mail. Appl Ergon. 2001;32(2):127–134.
McMurdo ME, Millar AM, Daly F. A randomized controlled trial of fall prevention strategies in old peoples’ homes. Gerontology. 2000;46(2):83–87.
Morley JE. Falls: where do we stand? Mo Med. 2007;104(1):63–67.
Bellemere P. A national campaign for the prevention of hand accidents. Chir Main. 2003;22(5):233–239.
Pickett W, Brison RJ, Niezgoda H, Chipman ML. Nonfatal farm injuries in Ontario: a population-based survey. Accid Anal Prev. 1995;27(4):425–433.
Kallin K, Jensen J, Olsson LL, Nyberg L, Gustafson Y. Why the elderly fall in residential care facilities, and suggested remedies. Fam Pract. 2004;53(1):41–52.
Schillings AM, Mulder T, Duysens J. Stumbling over obstacles in older adults compared to young adults. Neurophysiol. 2005;94(2):1158–1168.
Tammelleo AD. Legal case briefs for nurses, AL: nurse spills water—patient falls: liability issue. NY Regan Rep Nurs Law. 1991;31(9):3.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cappell, M.S. Injury to Endoscopic Personnel from Tripping over Exposed Cords, Wires, and Tubing in the Endoscopy Suite: A Preventable Cause of Potentially Severe Workplace Injury. Dig Dis Sci 55, 947–951 (2010). https://doi.org/10.1007/s10620-009-0923-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-009-0923-0