
Abstract
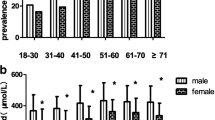
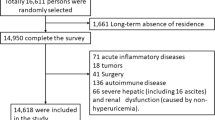
To investigate the prevalence of hyperuricemia in general Thai population and to evaluate its association with metabolic syndrome. A total of 1,945 subjects who sought for routine annual health checkup in our hospital from 1 October 2009 to 31 March 2010 were enrolled into the study. Inclusion criteria were healthy individuals, aged ≥35 years old, and lived in Bangkok for over 10 years. Data of general health status, age, gender, history of alcoholic consumption, body weight, height, and waist circumference were obtained by an interview-structured questionnaire. Fasting blood sample was collected from each subject early in the morning for uric acid, total cholesterol, high density lipoprotein cholesterol, triglycerides, and glucose levels. The prevalence of hyperuricemia in our study population was 24.4%, being significantly more common in men than women (59% vs. 11%, p < 0.001). The condition was also associated with various features of high body mass index or waist circumference, alcohol consumption, dyslipidemia, and high fasting blood glucose. Metabolic syndrome was found in 35% and 23% of men and women with hyperuricemia; direct relationship between level of uric acid and prevalence of metabolic syndrome was observed. Hyperuricemia is common among Bangkok population in our study. This disorder is frequently associated with metabolic syndrome.
Similar content being viewed by others

References
Choi HK, Atkinson K, Karlson EW, Willen WC, Curhan G (2004) Purine-rich foods, dairy and protein intake, and the risk of gout in men. New Eng J Med 350:1003–1007
Krishnan E, Griffith C, Kwoh C (2005) Burden of illness from gout in ambulatory care in the United States. Arhritis Rheum 52:S656
Arromdee E, Michet CJ, Crowson CS, O’Fallon WM, Gabriel SE (2002) Epidemiology of gout: is the incidence rising? J Rheumatol 29:2403–2406
Wallace KL, Riedel AA, Joseph-Ridge N, Wortmann R (2004) Increasing prevalence of gout and hyperuricemia over 10 years among older adults in a managed care population. J Rheumatol 31:1582–1587
Terkeltaub RA (2003) Clinical practice: gout. N Engl J Med 349:1647–1655
Klemp P, Stansfied S, Castle B, Robertson M (1997) Gout is on the increase in New Zealand. Ann Rheum Dis 56:22–27
Darmawan J, Valkenburg HA, Muirden KD, Wigley RD (1992) The epidemiology of gout and hyperuricemia in a rural population in Java. J Rheumatol 19:1595–1599
Lee M-S, Lin S-C, Chang H-Y, Lyu L-C, Tsai K-S, Pan W-H (2005) High prevalence of hyperuricemia in elderly Taiwanese. Asia Pac J Clin Nutr 14:285–292
Mikuls TR, Saag KG (2006) New insights into gout epidemiology. Curr Opin Rheumatol 18:199–203
Campion EW, Glynn RJ, deLabry LO (1987) Asymptomatic hyperruricemia: the risks and consequences. Am J Med 82:421–442
Grundy SM (2007) Metabolic syndrome: a multiplex cardiovascular risk factor. J Clin Endocrinol Metab 92:399–404
Yoo TW, Sung KC, Shin HS, Kim BS, Kang JH et al (2005) Relationship between serum uric acid concentration and insulin resistance and metabolic syndrome. Circ J 69:928–933
Myers A, Epstein FH, Dodge HJ, Mikkelsen WM (1968) The relation of serum uric acid to risk factors in coronary heart disease. Am J Med 45:520–528
Iwashima Y, Horio T, Kamide K, Rakugi H, Ogihara T, Kawano Y (2006) Uric acid, left ventricular mass index, and risk of cardiovascular disease in essential hypertension. Hypertension 47:195–202
Abbbott RD, Brand FN, Kannel WB, Castelli WP (1988) Gout and coronary heart disease: the Framingham study. J Clin Epidemiol 41:237–242
Sundstrom J, Sullivan L, D’Agostino RB, Levy D, Kannel WB, Vasan RS (2005) Relations of serum uric acid to longitudinal blood pressure tracking and hypertension incidence. Hypertension 45:28–33
Krishnan E, Kwoh K, Schumacher HR, Kuller L (2007) Hypertension and incidence of hypertension among men without metabolic syndrome. Hypertension 49:298–303
Lee J, Sparrow D, Vokonas PS, Landsberg L, Weiss ST (1995) Uric acid and coronary heart disease risk: evidence for a role of uric acid in the obesity-insulin resistance syndrome. the normative aging study. Am J Epidemiol 142:288–294
Himmelmann A, Kjeldsen SE, Hedner T (2003) Recent hypertension guidelines: JNC-7 and ESH/ESC. Blood Press 12:196–197
World Health Organization (1998) Report of a WHO consultation on obesity. obesity: preventing and managing the global epidemic. Geneva: World Health Organization
Alberti KGM, Zimmer P, Shaw J (2006) Metabolic syndrome: a new world-wide definition. a consensus statement from the International Diabetes Federation. Diabet Med 23:469–480
Nan H, Qiao Q, Dong Y, Gao W, Tang B, Qian R et al (2006) The prevalence of hyperuricemia in a population o f the coastal city of Qingdao, China. J Rheumato l33:1346–1350
Lohsoonthorn V, Dhanamun B, Williams MA (2006) Prevalence of hyperuricemia and its relationship with metabolic syndrome in Thai adults receiving annual health exams. Arch Med Res 37:883–889
Lin KC, Lin HY, Chou P (2000) Community based epidemiological study on hyperuricemia and gout in Kin-Hu, Kinmen. J Rheumatol 27:1045–1050
Gordon T, Kannel WB (1983) Drinking and its relation to smoking, BP, blood lipids, and uric acid. the Framingham study. Arch Int Med 143:1366–1374
Choi HK, Curhan G (2004) Beer, liquor and wine consumption and serum uric acid level: the third National Health and Nutrition Examination Survey. Arthritis Rheum 51:1023–1029
Choi HK, Liu S, Curhan G (2005) Intake of purine-rich foods, protein and dairy products and relationship to serum levels of uric acid: the third National Health and Nutrition Examination Survey. Arthritis Rheum 52:283–289
Choi JW, Ford ES, Gao X, Choi HK (2008) Sugar-sweetened soft drinks, diet soft drinks, and serum uric acid level: the third National Health and Nutrition Examination Survey. Arthritis Rheum 59:109–116
Yamamoto T, Moriwaki Y, Agbedana OE, Takahashi S, Suda M, Higashino K (1994) Impaired lipoprotein metabolismin patients with primary gout: influence of alcohol intake and body weight. Br J Rheumatol 33:731–734
Vuorinen-Markkola H, Yki-Jarvinen H (1994) Hyperuricemia and insulin resistance. J Clin Endocrinol Metab 78:25–29
Rathmann W, Funkhouser E, Dyer AR, Roseman JM (1998) Relations of hyperuricemia with the various components of the insulin resistance syndrome in young black and white adults: the CARDIA study. coronary artery risk development in young adults. Annuals Epidemiol 8:250–261
Choi HK, Atkinson K, Karlson EW, Curhan G (2005) Obesity, weight change, hypertension, diuretic use, and risk of gout in men. Arch Intern Med 165:742–748
Reaven GM (1997) The kidney: an unwilling accomplice in syndrome X. Am J Kidney Dis 30:928–931
Masuo K, Kawaguchi H, Mikami H, Ogihara T, Tuck ML (2003) Serum uric acid and plasma norepinephrine concentrations predict subsequent weight gain and blood pressure elevation. Hypertension 42:474–480
Jordan KM, Cameron JS, Snaith M, Zhang W, Doherty M, Seckl J et al (2007) British Society for Rheumatology and British Health Professionals in Rheumatology guideline for the management of gout. Rheumatol Oxf 46:1372–1374
Zhang W, Doherty M, Pascual E, Bardin T, Barskova V, Conaghan P et al (2006) EULAR evidenced based recommendations for gout. Part II: management. report of a task force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann Rheum Dis 65:1312–1324
Acknowledgment
The study was supported by a grant from Medical Research Fund, Bangkok Metropolitan Administration Medical College and Vajira Hospital. The authors wish to thank: Dr. Vallop Suwandee and Dr. Siriwan Tangjitgamol for their support in preparing the manuscript; Dr. Sumonmal Manusirivithaya and Miss Busaba Supawattanabodee for their statistical advice.
Disclosures
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Uaratanawong, S., Suraamornkul, S., Angkeaw, S. et al. Prevalence of hyperuricemia in Bangkok population. Clin Rheumatol 30, 887–893 (2011). https://doi.org/10.1007/s10067-011-1699-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-011-1699-0