
Abstract
Introduction
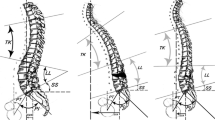
Sagittal imbalance is a spine deformity with multifactorial etiology, associated with severe low back pain and gait disturbance that worsen deeply patients’ quality of life. The amount of correction achievable through PSO is limited by the height of the resection of the posterior wall, causing a ceiling of segmental correction of 30–35°. The aim of this study is to describe and preliminarily evaluate the results of an alternative technique, corner osteotomy (CO), that can increase the amount of correction.
Materials and methods
From March 2012, every patient examined in our Division, diagnosed with sagittal imbalance to be treated with PSO, underwent CO and fusion. This technique consists in removing the posterior vertebral arch, the pedicle and the posterior–superior corner of the vertebral body; the inferior endplate of the vertebra above is prepared and the superior adjacent disc removed to obtain, when closing the osteotomy, a direct interbody fusion. Ten patients undergoing CO were compared with 20 patients undergoing PSO regarding spinopelvic parameters, operative variables, complications and degree of correction.
Results
Patients undergoing CO obtained higher lordotic angle at the osteotomy than patients undergoing PSO (36.6° ± 8.2° vs 16.5° ± 9.5°, p < 0.001) and had lower postoperative PT and SVA and higher average increase in lordosis. Complications were similar between groups. A trend toward longer surgical time, greater bleeding and higher transfusion rate was observed in the CO group, though this finding could be related to higher complexity of cases or incidence of associated anterior approach.
Discussion and conclusions
Corner osteotomy technique was more effective than the PSO in increasing segmental and lumbar lordosis with modest increase in blood loss and similar complication rate. The CO technique, in addition, proved a good reproducibility. Further studies with larger populations should confirm these preliminary results.










Similar content being viewed by others


References
Lafage V, Schwab F, Patel A et al (2009) Pelvic tilt and truncal inclination: two key radiographic parameters in the setting of adults with spinal deformity. Spine 34:E599–E606
Smith JS, Shaffrey CI, Berven S, Glassman S, Hamill C, Horton W, Ondra S, Schwab F, Shainline M, Fu KM, Bridwell K (2009) Improvement of back pain with operative and non operative in adults with scoliosis. Neurosurgery 65:86–93
Smith JS, Shaffrey CI, Glassman SD, Berven SH, Schwab FJ, Hamill CL, Horton WC, Ondra SL, Sansur CA, Bridwell KH (2011) Risk-benefit assessment of surgery for adult scoliosis: an analysis based on patient age. Spine 36:817–824
Rose PS, Bridwell KH, Lenke LG, Cronen GA, Mulconrey DS, Buchowski JM, Kim YJ (2009) Role of pelvic incidence, thoracic kyphosis, and patient factors on sagittal plane correction following pedicle subtraction osteotomy. Spine 34:785–791
Mi Kyung K, Sun-Ho L, Eun-Sang K, Whan E, Sung-Soo C, Chong-Suh L (2011) The impact of sagittal balance on clinical results after posterior interbody fusion for patients with degenerative spondylolisthesis: a pilot study. BMC Musculoskelet Disord 12:69. doi:10.1186/1471-2474-12-69
Lamartina C, Berjano P, Petruzzi M, Sinigaglia A, Casero G, Cecchinato R, Damilano M, Bassani R (2012) Criteria to restore sagittal balance in deformity and degenerative spondylolisthesis. Eur Spine J 21:27–31
Jackson RP, McManus AC (1994) Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size. A prospective controlled clinical study. Spine 19:1611–1618
Lazennec JY, Ramaré S, Arafati N, Laudet CG, Gorin M, Roger B, Hansen S, Saillant G, Maurs L, Trabelsi R (2000) Sagittal alignment in lumbosacral fusion: relations between radiological parameters and pain. Eur Spine J 9:47–55
Mehta VA, Amin A, Omeis I, Gokaslan ZL, Gottfried ON (2012) Implications of spinopelvic alignment for the spine surgeon. Neurosurgery 70:707–721
Boulay C, Tardieu C, Hecquet J, Benaim C, Mouilleseaux B, Marty C, Prat-Pradal D, Legaye J, Duval-Beaupère G, Pélissier J (2006) Sagittal alignment of spine and pelvis regulated by pelvic incidence: standard values and prediction of lordosis. Eur Spine J 15:415–422
Mac-Thiong JM, Roussouly P, Berthonnaud E, Guigui P (2010) Sagittal parameters of global spinal balance: normative values from a prospective cohort of seven hundred nine Caucasian asymptomatic adults. Spine 35:1193–1198
Schwab F, Lafage V, Patel A, Farcy JP (2009) Sagittal plane considerations and the pelvis in the adult patient. Spine 34:1828–1833
Roussouly P, Nnadi C (2010) Sagittal plane deformity: an overview of interpretation and management. Eur Spine J 19:1824–1836
Berjano P, Bassani R, Casero G, Sinigaglia A, Cecchinato R, Lamartina C (2013) Failures and revisions in surgery for sagittal imbalance: analysis of factors influencing failure. Eur Spine J. doi:10.1007/s00586-013-3024-x
Enercan M, Ozturk C, Kahraman S, Sarıer M, Hamzaoglu A, Alanay A (2012) Osteotomies/spinal column resections in adult deformity. Eur Spine J 22(Suppl 2):S254–S264
Chang K, Cheng C, Chen H, Chang K, Chen T (2008) Closing-opening wedge osteotomy for the treatment of sagittal imbalance. Spine 33(13):1470–1477
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Berjano, P., Pejrona, M., Damilano, M. et al. Corner osteotomy: a modified pedicle subtraction osteotomy for increased sagittal correction in the lumbar spine. Eur Spine J 24 (Suppl 1), 58–65 (2015). https://doi.org/10.1007/s00586-014-3618-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-014-3618-y