
Abstract
Background
Vitamin D deficiency may contribute to osteoporosis in nephrotic syndrome (NS).
Methods
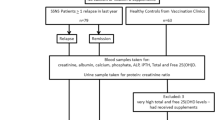
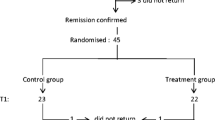
A cross-sectional case–control study was performed to investigate 25 hydroxycholecalciferol [25(OH)D] status in 40 patients with NS in remission and 40 healthy controls. Serum levels of 25(OH)D, calcium, phosphate, alkaline phosphatase (ALP), and intact parathyroid hormone (PTH) were assayed. NS patients were segregated by age at onset, current age, type and duration of NS, months since relapse and current drug therapy.
Results
Levels of 25(OH)D showed a positive correlation with months elapsed since last NS relapse (r s = +0.4, p = 0.012) and were lower in NS patients within 3 months of relapse but similar to that of controls in patients in remission for >3 months [median 14.23 (interquartile range 12.19–17.63) vs. 19.75 (14.04–28.38) ng/ml, respectively; p = 0.039]. There was no correlation of 25(OH)D levels with other disease characteristics or drug therapy. ALP levels were also lowest after relapse (r s = +0.34, p = 0.036). Overall, 25(OH)D levels of <20 ng/ml occurred in 62.5 % of NS patients + controls, and correlated negatively with age (r s = −0.24, p = 0.037) but showed no significant correlation with calcium, phosphate, or PTH levels.
Conclusions
In our patients with NS, vitamin D stores remained low for 3 months after NS relapse but showed an increase with longer remission time to control levels. Vitamin D stores were not influenced by disease characteristics or therapy. Longitudinal studies are required to confirm these findings and evaluate the effect of vitamin D on bones, particularly in frequent relapsers.



Similar content being viewed by others

References
Rathi N, Rathi A (2011) Vitamin D and child health in the 21st century. Indian Pediatr 48:619–625
Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T, Dawson-Hughes B (2006) Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am J Clin Nutr 84:18–28
Kulie T, Groff A, Redmer J, Hounshell J, Schrager S (2009) Vitamin D: an evidence-based review. J Am Board Fam Med 22:698–706
Feber J, Gaboury I, Ni A, Alos N, Arora S, Bell L, Blydt-Hansen T, Clarson C, Filler G, Hay J, Hebert D, Lentle B, Matzinger M, Midgley J, Moher D, Pinsk M, Rauch F, Rodd C, Shenouda N, Siminoski K, Ward LM, Canadian STOPP Consortium (2012) Skeletal findings in children recently initiating glucocorticoids for the treatment of nephrotic syndrome. Osteoporos Int 23:751–760
Koşan C, Ayar G, Orbak Z (2012) Effects of steroid treatment on bone mineral metabolism in children with glucocorticoid-sensitive nephrotic syndrome. West Indian Med J 61:627–630
Bak M, Serdaroglu E, Guclu R (2006) Prophylactic calcium and vitamin D treatments in steroid-treated children with nephrotic syndrome. Pediatr Nephrol 21:350–354
Lombel RM, Gipson DS, Hodson EM (2012) Treatment of steroid-sensitive nephrotic syndrome: new guidelines from KDIGO. Pediatr Nephrol 28:415–426
Indian Pediatric Nephrology Group, Indian Academy of Pediatrics, Bagga A, Ali U, Banerjee S, Kanitkar M, Phadke KD, Senguttuvan P, Sethi S, Shah M (2008) Management of steroid sensitive nephrotic syndrome: revised guidelines. Indian Pediatr 45:203–214
Gulati S, Godbole M, Singh U, Gulati K, Srivastava A (2003) Are children with idiopathic nephrotic syndrome at risk for metabolic bone disease? Am J Kidney Dis 41:1163–1169
Canalis E (2003) Mechanisms of glucocorticoid-induced osteoporosis. Curr Opin Rheumatol 15:454–457
O’Brien CA, Jia D, Plotkin LI, Bellido T, Powers CC, Stewart SA, Manolagas SC, Weinstein RS (2004) Glucocorticoids act directly on osteoblasts and osteocytes to induce their apoptosis and reduce bone formation and strength. Endocrinology 145:1835–1841
Freundlich M, Jofe M, Goodman WG, Salusky IB (2004) Bone histology in steroid-treated children with non-azotemic nephrotic syndrome. Pediatr Nephrol 19:400–407
Freundlich M, Bourgoignie JJ, Zilleruelo G, Abitbol C, Canterbury JM, Strauss J (1986) Calcium and vitamin D metabolism in children with nephrotic syndrome. J Pediatr 108:383–387
Huang JP, Bai KM, Wang BL (1992) Vitamin D and calcium metabolism in children with nephrotic syndrome of normal renal function. Chin Med J (Engl) 105:828–832
Grymonprez A, Proesmans W, Van Dyck M, Jans I, Goos G, Bouillon R (1995) Vitamin D metabolites in childhood nephrotic syndrome. Pediatr Nephrol 9:278–281
Chan YL, Mason RS, Parmentier M, Savdie E, Lissner D, Posen S (1983) Vitamin D metabolism in nephrotic rats. Kidney Int 24:336–341
Barragry JM, France MW, Carter ND, Auton JA, Beer M, Boucher BJ, Cohen RD (1977) Vitamin D metabolism in nephrotic syndrome. Lancet 2:629–632
Greenbaum LA, Benndorf R, Smoyer WE (2012) Childhood nephrotic syndrome—current and future therapies. Nat Rev Nephrol 8:445–458
Sinha A, Bagga A (2012) Nephrotic syndrome. Indian J Pediatr 79:1045–1055
Weng FL, Shults J, Herskovitz RM, Zemel BS, Leonard MB (2005) Vitamin D insufficiency in steroid-sensitive nephrotic syndrome in remission. Pediatr Nephrol 20:56–63
Biyikli NK, Emre S, Sirin A, Bilge I (2004) Biochemical bone markers in nephrotic children. Pediatr Nephrol 19:869–873
Papandreou D, Malindretos P, Karabouta Z (2010) Possible health implications and low vitamin D status during childhood and adolescence: an updated mini review. Int J Endocrinol 2010:472173
Belostotsky V, Mughal MZ, Berry JL, Webb NJ (2008) Vitamin D deficiency in children with renal disease. Arch Dis Child 93:959–962
Hegarty J, Mughal MZ, Adams J, Webb NJ (2005) Reduced bone mineral density in adults treated with high-dose corticosteroids for childhood nephrotic syndrome. Kidney Int 68:2304–2309
Wetzsteon RJ, Shults J, Zemel BS, Gupta PU (2009) Divergent effects of glucocorticoids on cortical and trabecular compartment BMD in childhood nephrotic syndrome. J Bone Miner Res 24:503–513
Mithal A, Wahl DA, Bonjour JP, Burckhardt P, Dawson-Hughes B, Eisman JA, El-Hajj Fuleihan G, Josse RG, Lips P, Morales-Torres J, IOF Committee of Scientific Advisors (CSA) Nutrition Working Group (2009) Global vitamin D status and determinants of hypovitaminosis D. Osteoporos Int 20:1807–1820
Harinarayan CV, Joshi SR (2009) Vitamin D status in India–its implications and remedial measures. J Assoc Phys India 57:40–48
Lips P (2006) Vitamin D physiology. Prog Biophys Mol Biol 92:4–8
Funding
None.
Competing Interests
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Banerjee, S., Basu, S. & Sengupta, J. Vitamin D in nephrotic syndrome remission: a case–control study. Pediatr Nephrol 28, 1983–1989 (2013). https://doi.org/10.1007/s00467-013-2511-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-013-2511-y