
Abstract
Background
Single-site-access (SSA) laparoscopy is more challenging to perform than multiport (MP) laparoscopy. This study examined the effect of MP versus SSA skills training on laparoscopic performance using surgically naive medical students.
Methods
For the study, 40 medical students at the end of their first year were randomized into two groups. Both groups were trained in four basic laparoscopic drills (peg, rope, bean drop, pattern cutting) using a standard MP setup (group 1) and an SSA approach (group 2). The time and number of repetitions required to attain proficiency were recorded. Each group then crossed over to the alternate approach and repeated the sequence. Data are presented as mean ± standard deviation, and statistical analysis was performed using the two-tailed, unpaired t test.
Results
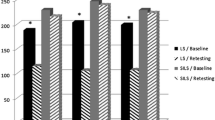
The total times required to attain proficiency for the SSA and MP approaches were not significantly different between the MP-trained group (234.0 ± 114.9 min) and the SSA-trained group (216.4 ± 106.5 min) (p = 0.67). The MP-trained group required less time to reach proficiency on the standard MP setup than the group using the SSA approach (119.1 ± 69.7 vs. 178.0 ± 93.4 min; p = 0.058) and significantly fewer repetitions (77.6 ± 42.6 vs. 118.8 ± 54.3; p = 0.027). The SSA-trained group required significantly less time to reach proficiency on the MP setup than the standard MP-trained group (38.4 ± 29.4 vs. 119.1 ± 69.7 min; p = 0.0013) and needed only a mean of 26.9 repetitions. When the standard MP trainees crossed over to the SSA setup, they required significantly less time to reach proficiency with the SSA approach than the SSA-trained group (114.8 ± 50.5 vs. 178.0 ± 93.4 min; p = 0.026) but required more repetitions than with the MP approach (86.2 ± 35.2 vs. 77.6 ± 42.6; nonsignificant difference).
Conclusions
Laparoscopic SSA skills training results in longer times and more repetitions to achieve proficiency than MP training, but the skills acquired transfer well to the MP approach.





Similar content being viewed by others


References
Navarra G, Pozza E, Occhionorelli S, Carcoforo P, Donini I (1997) One-wound laparoscopic cholecystectomy. Br J Surg 84:695
Vidal O, Valentini M, Ginestà C, Martí J, Espert JJ, Benarroch G, García-Valdecasas JC (2009) Laparoendoscopic single-site surgery appendectomy. Surg Endosc [Epub ahead of print 19 August]
Jeong BC, Park YH, Han DH, Kim HH (2009) Laparoendoscopic single-site and conventional laparoscopic adrenalectomy: a matched case–control study. J Endourol 23:1957–1960
Nguyen NT, Slone J, Reavis K (2009) Comparison study of conventional laparoscopic gastric banding versus laparoendoscopic single site gastric banding. Surg Obes Relat Dis [Epub ahead of print 10 November]
Canes D, Berger A, Aron M, Brandina R, Goldfarb DA, Shoskes D, Desai MM, Gill IS (2009) Laparo endoscopic single site (LESS) versus standard laparoscopic left donor nephrectomy: matched-pair comparison. Eur Urol [Epub ahead of print 28 July]
Scott DJ (2006) Patient safety, competency, and the future of surgical stimulation. Simul Healthcare 1:164–170
Society of American Gastrointestinal and Endoscopic Surgeons (2010) Fundamentals of laparoscopic surgery (FLS) program. Retrieved 7 March 2010, http://flsprogram.org
Rosser JC, Rosser LE, Savalgi RS (1997) Skill acquisition and assessment for laparoscopic surgery. Arch Surg 132:200–204
ACS/APDS Surgical Skills Curriculum for Residents, Phase 1: Module 17 Basic Laparoscopic Skills. Retrieved xxxx at http://elearning.facs.org/login/index.php
Mac Donald E, Pringle K, Ahmed I (2009) Single port laparoscopic repair of incarcerated ventral hernia. Hernia [Epub ahead of print]
Jacob BP, Tong W, Reiner M, Vine A, Katz LB (2009) Single-incision total extraperitoneal (one-site) laparoscopic inguinal hernia. Hernia 13:571–572
Barbaros U, Dinccag A (2009) Single-incision laparoscopic splenectomy: the first two cases. J Gastrointest Surg 13:1520–1523
Rawlings A, Hodgett SE, Matthews BD, Strasberg SM, Quasebarth M, Brunt LM (2010) Single-incision laparoscopic cholecystectomy: initial experience with critical view of safety dissection and routine intraoperative cholangiography. JACS
Fried GM, Feldman LS, Vassiliou MC, Fraser SA, Stanbridge D, Ghitulescu G, Andrew CG (2004) Proving the value of simulation in laparoscopic surgery. Ann Surg 240:518–528
Scott DJ, Dunnington GL (2008) The new ACS/APDS skills curriculum: moving the learning curve out of the operating room. J Gastrointest Surg 12:213–221
Sroka G, Feldman LS, Vassiliou MC, Kavena PA, Fayez R, Fried G (2010) Fundamentals of laparoscopic surgery simulator training to proficiency improves laparoscopic performance in the operating room: a randomized controlled trial. Am J Surg 199:115–120
Acknowledgments
The authors acknowledge the Washington University Institute for Minimally Invasive Surgery for support of this study. Daniel Cox was supported by T35 DK074375.
Disclosures
Michael Brunt had educational grant support from Ethicon Endosurgery, Inc., educational grant support and equipment support from Karl Storz Endoscopy and Stryker Endoscopy, grant and research support from Lifecell Corp., and honoraria for speaking and teaching from Ethicon Endosurgery, Covidien, and Cook Medical. None of these disclosures are related to the content of this study, which was conducted in a completely independent manner and free of industry funding.
Conflict of interest
Daniel R. Cox, Wenjing Zeng, and Margaret M. Frisella have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cox, D.R., Zeng, W., Frisella, M.M. et al. Analysis of standard multiport versus single-site access for laparoscopic skills training. Surg Endosc 25, 1238–1244 (2011). https://doi.org/10.1007/s00464-010-1349-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-010-1349-7