
Abstract
Background
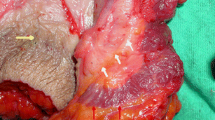
Lateral internal anal sphincterotomy (LIS) is considered the treatment of choice for chronic anal fissure. This study aimed to compare the outcome of standard LIS and posterolateral internal sphincterotomy (PLIS) at 5 o’clock position as regards healing of anal fissure, improvement in symptoms, and complications.
Methods
Patients with chronic anal fissure were randomly allocated to one of two groups; group I underwent PLIS and group II underwent LIS. Patients were compared regarding the duration of healing of anal fissure, improvement in anal pain as recorded by visual analogue scale (VAS), complications, particularly fecal incontinence (FI) and changes in the anal pressures.
Results
Eighty (49 females) patients were included to this trial. The mean age of patients was 35.5 years. The duration of healing was significantly shorter in group I than in group II (4.1 ± 1.7 vs 5.8 ± 1.4 weeks; p < 0.0001). Group I achieved significantly lower pain score at 1 month postoperatively than group II (1.1 ± 0.9 vs 1.7 ± 0.98; p = 0.005). Two (2.5%) of group I patients and six (10%) of group II patients experienced minor FI postoperatively. The postoperative reduction in the mean resting anal pressure in group I was significantly higher than that in group II.
Conclusion
Time to complete healing was significantly shorter and pain score was significantly lower after PLIS than after LIS which can be due to more reduction in the resting anal pressure after PLIS. Continence disturbances occurred after PLIS less frequently than after LIS; however, no significant differences between the two techniques were noted.
Trial registration
www.clinicaltrials.gov NCT03426449




Similar content being viewed by others

References
Dykes SL, Madoff RD (2007) Benign anorectal: anal fissure. In: The ASCRS textbook of colon and rectal surgery. Springer, New York, pp 178–191
Stewart Sr DB, Gaertner W, Glasgow S, Migaly J, Feingold D, Steele SR (2017) Clinical practice guideline for the management of anal fissures. Dis Colon Rectum 60(1):7–14
Shen B (2013) Pouchitis: what every gastroenterologist needs to know. Clin Gastroenterol Hepatol 11(12):1538–1549. https://doi.org/10.1016/j.cgh.2013.03.033
Collins EE, Lund JN (2007) A review of chronic anal fissure management. Tech Coloproctol. 11(3):209–223
Memon AS, Siddiqui FG, Hamad A (2010) Fissurectomy with posterior midline sphincterotomy for management of chronic anal fissure. J Coll Physicians Surg Pak 20(4):229–231
Nelson RL, Manuel D, Gumienny C, Spencer B, Patel K, Schmitt K, Castillo D, Bravo A, Yeboah-Sampong A (2017) A systematic review and meta-analysis of the treatment of anal fissure. Tech Coloproctol. 21(8):605–625
Nelson RL (2016) Efficacy of fissurectomy and botox for chronic anal fissure. Dis Colon Rectum 59(5):e41
Lunniss PJLIFT (2009) Procedure: a simplified technique for fistula-in-ano. Tech Coloproctol. 13(3):237–240
Schouten WR, Briel JW, Auwerda JJ (1994) Relationship between anal pressure and anodermal blood flow. The vascular pathogenesis of anal fissures. Dis Colon Rectum. 37(7):664–669
Jorge JM, Wexner SD (1993) Etiology and management of fecal incontinence. Dis Colon Rectum 36:77e97
Anal fissure, BMJ Best Practice [Database on the internet], http://bestpractice.bmj.com/best-ractice/monograph/563/basics/classification.html. Accessed on February 1, 2018
Emile SH, Youssef M, Elfeki H, Thabet W, Elgendy H, Omar W, Khafagy W, Farid M (2016) Effect of age, patient’s sex, and type of trauma on the correlation between size of sphincter defect and anal pressures in posttraumatic fecal incontinence. Surgery 160(5):1318–1325
Aslam MI, Pervaiz A, Figueiredo R (2014) Internal sphincterotomy versus topical nitroglycerin ointment for chronic anal fissure. Asian J Surg 37(1):15–19. https://doi.org/10.1016/j.asjsur.2013.07.004
Higuero T (2015) Update on the management of anal fissure. J Visc Surg 152(2 Suppl):S37–S43. https://doi.org/10.1016/j.jviscsurg.2014.07.007
Castillo E, Margolin DA (2004) Anal fissures: diagnosis and management. Tech Gastrointest Endosc 6(1):12–16
Barisone P, Ippoliti M, Dezzani C, Abbo L, Aimo I (2004) Operative procedures for anal fissure: open lateral internal sphincterotomy versus posterior midline sphincterotomy with anoplasty. Chirurgia 17(2):43–46
Mcnamara MJ, Percy JP, Fielding IR (1990) A Coloproctol study of anal fissure treated by subcutaneous lateral internal sphincterotomy. Ann Surg 211(2):235–238
Hancock BD (1977) The internal sphincter and anal fissure. Br J Surg 64(2):92–95
Chowcat NL, Araujo JGC, Boulos PB (1986) Internal sphincterotomy for chronic anal fissure: long term effects on anal pressure. Br J Surg 73(11):915–916
Peker K, Yilmaz I, Demiryilmaz I, Inal A, IŞIK A (2014) The effect of lateral internal sphincterotomy on resting anal sphincter pressures. Turk J Med Sci 44(4):691–695
Taylor BM, Beart RW Jr, Phillips SF (1984) Longitudinal and radial variations of pressure in the human anal sphincter. Gastroenterology 86(4):693–697
Rossi H, Rothenberger D (2015) Incontinence after lateral internal sphincterotomy. In: Pawlik TM, Maithel SK, Merchant NB (eds) Gastrointestinal surgery: management of complex perioperative complications. Springer Science+Business Media, New York, p 449
Emile SH (2017) Indications and technical aspects of internal anal sphincterotomy: highlighting the controversies. Dis Colon Rectum. 60(1):128–132
Nyam DC, Pemberton JH (1999) Long-term results of lateral internal sphincterotomy for chronic anal fissure with particular reference to incidence of fecal incontinence. Dis Colon Rectum. 42(10):1306–1310
Hyman N (2004) Incontinence after lateral internal sphincterotomy: a prospective study and quality of life assessment. Dis Colon Rectum 47(1):35–38
Garg P, Garg M, Menon GR (2013) Long-term continence disturbance after lateral internal sphincterotomy for chronic anal fissure: a systematic review and meta-analysis. Color Dis 15(3):e104–e117. https://doi.org/10.1111/codi.12108
Siproudhis L, Bellissant E, Pagenault M, Mendler MH, Allain H, Bretagne JF, Gosselin M (1999) Fecal incontinence with normal anal canal pressures: where is the pitfall? Am J Gastroenterol 94(6):1556–1563
Emile SH (2016) The orchestra of anal continence: how can it affect the management decision? World J Colorectal Surg 6(5):article 3
Arroyo A, Pérez F, Serrano P, Candela F, Lacueva J, Calpena R (2005) Surgical versus chemical (botulinum toxin) sphincterotomy for chronic anal fissure: long-term results of a prospective randomized clinical and manometeric study. Am J Surg 189(4):429–434
Chen HL, Woo XB, Wang HS, Lin YJ, Luo HX, Chen YH, Chen CQ, Peng JS (2014) Botulinum toxin injection versus lateral internal sphincterotomy for chronic anal fissure: a meta-analysis of randomized control trials. Tech Coloproctol 18(8):693–698
Notaras MJ (1969) Lateral subcutaneous sphincterotomy for anal fissure: a new technique. Proc R Soc Med 62:713
Author information
Authors and Affiliations
Contributions
Mohamed Farid introduced the concept of and designed the study. Sameh Emile and Mohammed Alawady collected the required data. Mohammed Alawady, Sameh Emile, Mahmoud Abdelnaby, and Hosam Elbanna conducted the procedures and the analysis of data. Mohamed Farid conducted interpretation of the results. Sameh Emile, Mohammed Alawady, and Hosam Elbanna wrote the manuscript. Mohamed Farid, Mahmoud Abdelnaby, and Hosam Elbanna drafted and critically revised the manuscript.
Corresponding author
Ethics declarations
Ethical approval for the study was obtained from the institutional review board (IRB) of Mansoura Faculty of Medicine.
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Alawady, M., Emile, S.H., Abdelnaby, M. et al. Posterolateral versus lateral internal anal sphincterotomy in the treatment of chronic anal fissure: a randomized controlled trial. Int J Colorectal Dis 33, 1461–1467 (2018). https://doi.org/10.1007/s00384-018-3087-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-018-3087-6