
Abstract
Purpose
Increasing evidence suggests that alterations in mitochondrial DNA (mtDNA) copy number (mtDNAcn) and relative telomere length (RTL) may be implicated in the tumorigenesis of several malignancies. Alterations of both RTL and mtDNAcn are generally accepted as independent biomarkers for predicting risk and prognosis in various cancers. The aim of this study was to evaluate the prognostic value of combining leukocyte RTL with mtDNAcn (RTL–mtDNAcn) in hepatocellular carcinoma (HCC).
Methods
RTL and mtDNAcn in peripheral blood leukocytes (PBLs) were measured using a real-time PCR-based method in a total of 250 HCC patients treated with transcatheter arterial chemoembolization (TACE). We evaluated the associations between RTL and/or mtDNAcn and HCC overall survival using Kaplan–Meier curve analysis and Cox proportional hazards regression model.
Results
We found that patients with longer leukocyte RTL or lower mtDNAcn had shorter overall survival time. The univariate analysis (HR 1.63, 95 % CI 1.23–2.17, P = 7.7 × 10−4) and multivariate analysis (HR 1.78, 95 % CI 1.31–2.42, P = 2.4 × 10−4) indicated that longer leukocyte RTL was significantly associated with poorer OS in HCC patients. Kaplan–Meier curve analysis showed that patients with longer RTL had shorter overall survival time than those with shorter RTL (log-rank P = 0.001). Patients with lower mtDNA copy number was significantly associated with poorer OS by Cox proportional hazards model using both univariate (HR 1.60, 95 % CI 1.21–2.13, P = 0.001) and multivariate analyses (HR 1.77, 95 % CI 1.30–2.41, P = 2.8 × 10−4). Kaplan–Meier curve analysis showed that patients with lower mtDNA content had significantly shorter overall survival time than those with higher mtDNA content (log-rank P = 0.001). Furthermore, combination of leukocyte RTL and mtDNAcn significantly improved the efficacy of predicting HCC prognosis. Patients with longer RTL and lower mtDNAcn exhibited a significantly poorer overall survival in both the univariate analysis (HR 2.21, 95 % CI 1.52–3.22, P = 3.5 × 10−5) and multivariate analysis (HR 2.60, 95 % CI 1.73–3.90, P = 4.3 × 10−6). The effect on patient prognosis was more evident in patients with longer RTL and lower mtDNAcn than in those with shorter RTL and lower mtDNA (HR 2.11, 95 % CI 1.34–3.32, P = 0.001) or in those with longer RTL and higher mtDNA (HR 2.10, 95 % CI 1.34–3.27, P = 0.001).
Conclusions
Our data suggest that combination of leukocyte RTL-mtDNAcn may be a potential efficient prognostic marker for HCC patients receiving the TACE treatment.
Similar content being viewed by others

Introduction
Human hepatocellular carcinoma (HCC) is one of the most frequent malignancies of liver and a major cause of cancer-related deaths worldwide [1], especially in China [2]. Surgery is one of the most appropriate treatments for HCC. However, only 10–20 % of HCC patients are eligible to receive surgery due to late diagnosis [3]. Local–regional therapy with transcatheter arterial chemoembolization (TACE) is commonly recommended as the first-line treatment for unresectable HCC patients [4]. The effectiveness of TACE is affected by multiple baseline clinical factors such as liver function, performance status, and tumor stage, and it varies significantly among HCC patients. The prognosis of HCC patients treated with TACE is greatly diverse according to disease status. Therefore, to improve the survival of TACE-treated HCC patients, it is urgently needed to identify novel prognostic biomarkers for the prediction of clinical outcomes and to tailor the treatment strategy based on the individual profile of patient.
Telomeres are dynamic nucleoprotein complexes located at ends of eukaryotic chromosomes, which are composed of small tandem “TTAGGG” repeat and telomere binding-associated proteins. Telomeres cap the ends of linear chromosomes, protecting them from degradation and other insults resulting from DNA damage response as well as end-to-end fusion [5]. Previous studies have reported that abnormal telomere length shortening leads to chromosome instability and abnormal lengthening of telomeric DNA rends the cell proliferation unrestricted, thus suggesting that telomere pathway is implicated in pathogenesis of many malignancies [5]. For example, previous studies have shown that telomere shortening might contribute to the development of HCC. In addition, many observational studies have suggested that relative telomere length (RTL) is significantly associated with cancer risk and patient prognosis, although results are not always consistent [6–12]. These aforementioned results suggest that telomere length may be a potential biomarker in the prediction of cancer risk and prognosis.
Mitochondria are primary organelles in eukaryotic cells and principally responsible for multiple cellular functions including cellular energy production, metabolism, apoptosis, and calcium homeostasis [13]. Physiologically, each cell contains multiple mitochondria and each mitochondrion contains 2–10 copies of mitochondrial DNA (mtDNA). The copy number of mtDNA is precisely modulated under physiological condition and is changed extensively under pathological condition [14]. Alterations of mtDNA content (increased or decreased) have been observed to be significantly associated with various malignancies [15, 16]. Recently, the mtDNA content in peripheral blood lymphocytes (PBLs) was reported as a potential biomarker to predict the risk and patients’ prognosis of various cancers [17–22]. Taken together, these data suggest that mtDNA content in blood samples have an immense potential to be a molecular predictor to screen individuals with higher cancer susceptibility and to evaluate malignant progression during the carcinogenic process.
Although alterations of individual telomere length or mtDNA content are generally accepted as independent biomarker in the prediction of cancer risk and prognosis, there has been no study to use telomere length and mtDNA content as combined biomarker in the prediction risk and prognosis of cancer. In the present study, we sought to assess whether leukocyte telomere length/mtDNA content alone or combined can be used to predict the overall survival in a hospital-based HCC patient population who received the TACE treatment.
Materials and methods
Study population
Originally, 269 Han Chinese patients with unresectable HCC were recruited into an ongoing epidemiological study at the Departments of Pain Treatment in the Tangdu Hospital (Hospital 1, n = 66) affiliated to the Fourth Military Medical University (FMMU) in Xi’an and the Eastern Hepatobiliary Surgery Hospital (Hospital 2, n = 203) affiliated to the Secondary Military Medical University (SMMU) in Shanghai between November 2008 and November 2010. All patients had no previous history of other cancers or cancer-related treatments and were newly diagnosed as HCC by imaging technologies. TACE was used as the first-line treatment for all patients as previously described [23]. Among them, 19 cases with incomplete clinical information or follow-up data or poor DNA quality were excluded. Finally, 250 patients were included, and RTL and mtDNAcn were successfully measured for further analysis. This study was approved by the related institutional review boards from FMMU and SMMU, and the signed informed consent was obtained from each participant.
Epidemiologic and clinical data collection
Demographic and personal data were collected through an in-person interview using a standardized questionnaire. Before the first TACE treatment, 5 ml of venous blood from each patient was drawn into coded sodium citrate anticoagulant tubes and delivered to the laboratory for analysis. Detailed clinical information was collected through medical record review by treating physicians. And standard follow-up was performed by a trained clinical specialist through on-site interview, direct calling, or medical record review. The latest follow-up data in this analysis were obtained in October 2015. Overall survival time was defined as the interval from the first TACE treatment to the date of death or last follow-up.
Measurement of relative telomere length and mtDNA copy number
Genomic DNA was extracted from peripheral blood lymphocytes(PBL) using the EZNA Blood DNA Midi Kit (Omega Bio-Tek, Norcross, Ga) according to the manufacturer’s protocol. The relative telomere length (RTL) and mtDNA copy number (mtDNAcn) were measured by quantitative real-time polymerase chain reaction (qRT-PCR) as previously described [19, 24, 25]. The primer sequences for the telomere gene were as follows: forward primer (tel-c), 5′-ACACTAAGGTTTGGGTTTGGGTTTGGGTTTGGGTTAGTGT-3′; reverse primer (tel-g), 5′-TGTTAGGTATCCCTATCCCTATCCCTATCCCTATCCCTAACA-3′. The primer sequences of MT-ND1 gene was used for mtDNA amplification, and the primer sequences were as follows: forward primer (ND1-F), 5′-CCCTAAAACCCGCCACATCT-3′; reverse primer (ND1-R), 5′-GAGCGATGGTGAGAGCTAAGGT-3′. The single-copy nuclear gene human globulin (HGB) was used as a housekeeping gene control in all reaction, and the primer pair was as follows: forward primer (HGB-1), 5′-GTGCACCTGACTCCTGAGGAGA-3′; reverse primer (HGB-2), 5′-CCTTGATACCAACCT GCCCAG-3′. First, the ratio of the telomere repeat copy number or mtDNA copy number (T) to the single gene (HGB) copy number (S) was determined for each sample using standard curves. The derived T/S ratio was proportional to the RTL or mtDNAcn. Second, the ratio for each sample was then normalized according to that in a calibrator DNA sample to standardize different runs. The calibrated T/S ratio was then used as the measurement of RTL or mtDNAcn in this study.
The PCR (20 μL) for gene-specific amplification consisted of mix containing 1 × SYBR green master mix (TaKaRa), 10 nM forward primer, 10 nM reverse primer, and 4 ng of genomic DNA. The thermal cycling conditions were at 95 °C for 30 s, followed by 35 cycles of 94 °C for 30 s, 56 °C (for telomere amplification) or 58 °C (for ND1 and HGB amplification) for 30 s, and 72 °C for 50 s with signal acquisition. The same negative and positive controls, a calibrator DNA, and a sample for constructing a standard curve were included in each run. Data were collected using the CFX Manager 2.1 (Bio-Rad). The R 2 for each standard curve was ≥0.99, with acceptable standard deviations set under 0.25 (for the Ct values). If the data were outside the acceptable range, the test was repeated. Laboratory persons conducting this experimental procedure were blinded to the endpoint of our study.
Statistical analyses
The SPSS version 19.0 software package (IBM, Armonk, NY, USA) was used for the analyses. Cumulative survival time was calculated using the Kaplan–Meier curve analysis. The difference on cumulative survival between different groups was analyzed using a log-rank test. The Cox proportional hazards regression model was used to evaluate the association between variables and HCC overall survival using univariate and multivariate analyses. All P values in this study were two sided, and P < 0.05 was considered to be significant.
Results
Characteristics of the study population
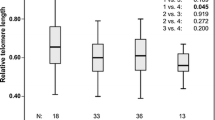
Demographic and clinical characteristics of 250 HCC patients are summarized in Table 1. Among a total of 250 HCC patients with first-line TACE treatment, the median age at the time of HCC diagnosis was 54 years. Majority of the patients were males (89.2 %) and with positive serum HBsAg (81.6 %). Almost all patients (92.8 %) had a Child–Pugh score A. There were more patients with multiple tumor nodules (55.2 %) and with higher level of serum AFP (56.4 %). There were 28.4 % (71) of patients with portal vein thrombus (PVT). According to the sixth edition of TNM Classification of International Union Against Cancer, the percentage (number) of patients with TNM stage I, II, III, and IV were 26.7 (69), 13.2 (33), 45.6 (114), and 13.6 (34), respectively. During the whole follow-up time, there were 193 deaths, among which 190 (98.4 %) died due to hepatic decompensation and/or tumor progression and 3 (1.6 %) were due to other causes. The median value of RTL and mtDNA copy number of all patients was 0.48 and 0.80, respectively.
Prognostic significance of clinical characteristics on HCC
The result of univariate analysis by Cox proportional hazards regression model showed that there was a significant poor overall survival in patients with late TNM stage disease (HR 2.40, 95 % CI 1.77–3.24, P = 1.3 × 10−8), in patients with positive PVT (HR 2.08, 95 % CI 1.52–2.85, P = 5.4 × 10−6), in patients with multiple tumor nodules (HR 1.43, 95 % CI 1.07–1.91,P = 0.015), and in patients with high level of serum AFP (HR 1.48, 95 % CI 1.11–1.97, P = 0.008) (Table 2). Furthermore, multivariate analysis revealed that advanced TNM stage (HR 1.94, 95 % CI 1.33–2.83, P = 5.9 × 10−4) and positive PVT (HR 1.58, 95 % CI 1.12–2.24, P = 0.010) were independent prognostic predictors for OS in all patients (Table 2).
Prognostic analysis of leukocyte RTL and mtDNA content in HCC patients
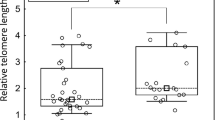
To investigate the prognostic significance of leukocyte RTL, we divided the patients into two subgroups by the median value (0.48) of RTL and estimated the association between RTL and the overall survival of HCC by logistic regression model using univariate and multivariate analyses. The median value of shorter and longer RTL was 0.35 and 0.62, respectively (Table 3). As shown in Table 3, univariate analysis indicated that longer leukocyte RTL was significantly associated with poorer OS in HCC patients (HR 1.63, 95 % CI 1.23–2.17, P = 7.7 × 10−4). Multivariate analysis revealed that longer RTL remained to be significantly associated with poorer OS in HCC patients (HR 1.78, 95 % CI 1.31–2.42,P = 2.4 × 10−4). Kaplan–Meier curve analysis showed that patients with longer RTL had shorter overall survival time than those with shorter RTL (log-rank P = 0.001, Fig. 1a).

KM curves of the overall survival analyses in HCC patients. a RTL; b mtDNAcn; c RTL and mtDNAcn
We then assessed the prognostic effect of mtDNA content on HCC patients receiving TACE treatment. First, we dichotomized the patients into high- or low-mtDNAcn group by the median value (0.80) of mtDNAcn. The median value of high and low mtDNA content was 1.04 and 0.65, respectively (Table 3). As shown in Table 3, patients with lower mtDNA copy number was significantly associated with poorer OS by Cox proportional hazards model using both univariate (HR 1.60, 95 % CI 1.21–2.13, P = 0.001) and multivariate analyses (HR 1.77, 95 % CI 1.30–2.41, P = 2.8 × 10−4). Moreover, Kaplan–Meier curves analysis showed that patients with lower mtDNA content had significantly shorter overall survival time than those with higher mtDNA content (log-rank P = 0.001, Fig. 1b).
Prognostic analysis of mtDNA content and RLT in HCC patients stratified by host characteristics
To exclude the confounding factors that might affect the prognostic value of mtDNA content and/or RTL on HCC overall survival, we further evaluated the effects of mtDNA content or RTL on the OS of HCC patients stratified by host characteristics using multivariate analysis. As shown in Table 4, we found that lower mtDNAcn was significantly associated with poorer prognosis in older patients with an adjusted HR of 2.06 (95 % CI 1.34–3.16, P = 9.6 × 10−4) and in patients with multiple number of tumors (HR 2.04, 95 % CI 1.35–3.12, P = 7.0 × 10−4). Interestingly, longer RTL was significantly associated with poorer HCC OS in younger patients (HR 2.3, 95 % CI 1.41–3.47, P = 8.1 × 10−4, Table 4). Similarly, there is a significant association between longer RTL and poorer OS in patients with multiple tumors (HR 2.03, 95 % CI 1.32–3.12, P = 0.001, Table 4).
Combined prognostic value of mtDNA content and RLT in HCC patients
To assess whether combination of leukocyte RTL and mtDNAcn can improve prognostic prediction efficacy in HCC patients, we further analyzed the effect of combining RTL and mtDNAcn on HCC overall survival. Using patients with shorter RTL and higher mtDNAcn as reference group, patients with longer RTL and lower mtDNAcn exhibited a significantly poorer overall survival in both the univariate analysis (HR 2.21, 95 % CI 1.52–3.22, P = 3.5 × 10−5) and multivariate analysis (HR 2.60, 95 % CI 1.73–3.90, P = 4.3 × 10−6). The effect on patient prognosis was more evident in patients with longer RTL and lower mtDNAcn than in those with shorter RTL and lower mtDNA (HR 2.11, 95 % CI 1.34–3.32, P = 0.001) or those with longer RTL and higher mtDNA (HR 2.10, 95 % CI 1.34–3.27, P = 0.001), (Table 5). Additionally, Kaplan–Meier analysis indicated that patients with shorter RTL and higher mtDNAcn exhibited the longest overall survival time, whereas those with longer RTL and lower mtDNA copy number exhibited the shortest overall survival time (log-rank P = 3.3 × 10−4, Fig. 1c). Furthermore, Pearson’s correlation coefficient was used to evaluate the correlation between mtDNA content and telomere length in HCC patients. As shown in Supplementary Figure. 1A, there was a positive correlation between telomere length and mtDNA copy number (r = 0.165, P = 0.029). All these data suggested that the combination of mtDNA content and RTL had a better efficacy in predicting prognosis of HCC patients with TACE treatment.
Discussion
In present study, we evaluated the prognostic value of leukocyte RTL and mtDNA content in a hospital-based cohort of 250 HCC patients receiving TACE treatment. We found that patients with longer leukocyte RTL or with lower leukocyte mtDNAcn showed poorer prognosis, suggesting that leukocyte RTL and mtDNAcn may serve as independent prognostic factors for HCC patients with TACE treatment. Moreover, combination of leukocyte mtDNAcn and RTL significantly improved the prognosis prediction efficacy for HCC patients. To the best of our knowledge, this is the first study to investigate the combined prognostic effect of mtDNA content and RLT in leukocytes on HCC survival.
A growing number of epidemiological studies have demonstrated that extensive alteration of telomere length is associated with genomic abnormalities which contribute to cancer development and progression [5, 26]. In addition, previous data have shown that leukocyte telomere length is associated with clinical outcome or prognosis of various tumors [7, 9, 10, 12, 27]. These data collectively suggest the telomere length may be a putative biomarker for risk assessment and prognostication of malignancies. In the present study, we also assessed the associations of leukocyte RTL with the OS of the HCC patients treated with TACE. Consistent with previous findings [7, 9, 10], our result confirmed the significant association between longer leukocyte RTL and poorer prognosis in HCC patients. In contrast, several other studies have reported that patients with shorter leukocyte RTL have worse survival in gastric cancer and colorectal cancer [11, 28]. These discrepant results have suggested that the relationship between leukocyte RTL and cancer prognosis may be cancer organ specific.
Previous studies have indicated a potential involvement of the alterations of mtDNA content (increased or decreased) in the tumorigenesis and development of many malignancies [15, 16]. For instance, several studies have demonstrated that leukocyte mtDNA content is associated with the risks or prognosis of some tumor [16–22]. In line with these findings, the present study found that low leukocyte mtDNA content was associated with poor prognosis of HCC patients treated with TACE, suggesting that leukocyte mtDNA content may be used as an independent prognostic factor in HCC. However, several other studies have also reported that patients with high mtDNA content have worse survival in head and neck cancer and esophageal and laryngeal squamous cell carcinoma [29–31]. The discrepancy in these results can be attributed to the difference in follow-up periods, baseline clinicopathological characteristics, TNM stage, and therapeutic schedule. Taken together, these data suggest a critical role of mtDNA content as biomarker to predict cancer prognosis. Either increased or decreased mtDNA content might damage mitochondrial functions and thus promote tumor development and progression [27]. Further investigations are needed to elucidate the biological mechanisms underlying the association between mtDNA content and tumorigenesis.
As an indicator of biological age of cells, telomere length has been reported to be associated with the longevity of human. Previous studies have confirmed that telomere length is negatively associated with age in normal population, indicating that the telomere erosion happens during cell division [32–34]. We have performed further correlation analysis between age and RTL in the present study. As shown in Supplementary Figure. 1B, age was not significantly correlated with RTL. However, a negative correlation trend was noted between them. Previous studies have provided strong evidence to support the notion that the negative correlation exists between age and RTL in general population [32, 33]. Our inconsistent result may be explained by the relative sample size or different regulation mechanisms of telomere length under physiological and pathological conditions. Previous studies have shown that telomere shortening might contribute to HCC progress, and several studies have suggested that RTL is significantly associated with cancer risk and patient prognosis, although results are not always consistent [6–12]. In the present study, our stratified analysis showed that the effect of RTL on HCC prognosis was more prominent in younger patients than older ones, indicating the interaction of age and RTL in prognosis of HCC patients. However, due to the small sample size, we could not exclude the false discovery. Therefore, further validation is warranted in large populations.
In the stratified analyses, we found that high mtDNA content was significantly associated with poor prognosis in patients with older age or multiple tumors, but not in those with younger age or single tumor, indicating the modulating effects of host characteristics through unknown mechanisms. Mitochondrial decay has been shown to occur with age, and age-related decline in mtDNAcn has been previously found both in skeletal muscle and in pancreatic islets from healthy individuals [35, 36], and several previous studies have reported that there are both positive and negative correlations between age and mtDNAcn in tumor cells, but not in peripheral blood cells [19, 20, 37–39]. In the present study, we failed to find the significant correlation between age and mtDNAcn in peripheral blood cells from HCC patients (Supplementary Figure. 1C). The discrepancy among these studies may be explained by the diversity in characteristics of study population, limited sample sizes, and different types of biological material that are investigated. Our results suggest an effect of age on mtDNAcn in PBLs in HCC patients. The impact of alterations in mtDNAcn on cancer prognosis in older individuals may be indicative of the critical role of mtDNAcn in old HCC patients. However, the detailed mechanisms should be investigated in future.
The most salient feature of the present study was the assessment of the mtDNA content plus RLT as a novel index, RLT–mtDNAcn, in HCC prognosis. We identified a significant association between RLT–mtDNAcn and prognosis of HCC patients with TACE treatment. Alterations of both telomere length and mtDNA content are generally accepted as independent biomarker in the prediction of cancer risk and prognosis, and several studies have showed that mtDNA content is positively correlated with RTL in some disease [40, 41]. Consistently, our data have also shown that there is a weak positive correlation (P = 0.024) between telomere length and mtDNA copy number in HCC patients. A recent study has reported that the telomere-p53-peroxisome proliferator-activated receptor gamma co-activator (PGC) axis has a direct connection with telomere dysfunction and mitochondrial compromise [42], suggesting that telomere dysfunction may be associated with impaired mitochondrial biogenesis and function and the combined effect of both telomere dysfunction and mitochondrial compromise may be involved in tumorigenesis, which warrants further investigation in future studies. Previous high-throughput screening-based biomarkers studies have showed that combination of a few molecular biomarkers may significantly improve the efficacy of prognostic prediction [28, 43]. In the present study, our results have suggested that combination of leukocyte mtDNA content and RTL significantly improved the prognosis prediction efficacy for HCC receiving the TACE treatment.
There are several limitations in our study. First, the alteration of mtDNA content and RTL in PBLs after TACE treatment and during disease progression remains unclear. Second, our study is restricted to Han Chinese; the generalizability to other ethnic cohort needs further evaluation. Finally, we only carried out the association analyses between mtDNA content or RTL and prognosis of HCC patients. The underlying mechanisms that account for prognostic effects of leukocyte mtDNA content and RTL in HCC need further investigation.
In summary, our findings confirm that both leukocyte mtDNA content and telomere length may serve as useful biomarker for prognosis prediction of HCC patients receiving TACE treatment. In addition, the present study demonstrates that the combination of leukocyte RTL-mtDNAcn significantly improves the prognosis prediction efficacy for HCC patients; therefore, RTL-mtDNAcn may serve as a potential biomarker to predict HCC prognosis.
References
Siegel RL, Miller KD, Jemal A (2016) Cancer statistics, 2016. CA Cancer J Clin 66(1):7–30. doi:10.3322/caac.21332
Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, Yu XQ, He J (2016) Cancer statistics in China, 2015. CA cancer J clin. doi:10.3322/caac.21338
Yeh JH, Hung CH, Wang JH, Chen CH, Kee KM, Kuo CM, Yen YH, Cheng YF, Chen YY, Hsu HC, Lu SN (2015) Modifiable prognostic factors of hepatocellular carcinoma in patients with non-surgical treatment. PLoS One 10(12):e0144893. doi:10.1371/journal.pone.0144893
Yu X, Ge N, Guo X, Shen S, Liang J, Huang X, Wan S, Xing J, Huang Q, Yang Y (2014) Genetic variants in the EPCAM gene is associated with the prognosis of transarterial chemoembolization treated hepatocellular carcinoma with portal vein tumor thrombus. PLoS One 9(4):e93416. doi:10.1371/journal.pone.0093416
Bisoffi M, Heaphy CM, Griffith JK (2006) Telomeres: prognostic markers for solid tumors. Int J Cancer 119(10):2255–2260. doi:10.1002/ijc.22120
Sun B, Wang Y, Kota K, Shi Y, Motlak S, Makambi K, Loffredo CA, Shields PG, Yang Q, Harris CC, Zheng YL (2015) Telomere length variation: a potential new telomere biomarker for lung cancer risk. Lung Cancer 88(3):297–303. doi:10.1016/j.lungcan.2015.03.011
Svenson U, Nordfjall K, Stegmayr B, Manjer J, Nilsson P, Tavelin B, Henriksson R, Lenner P, Roos G (2008) Breast cancer survival is associated with telomere length in peripheral blood cells. Cancer Res 68(10):3618–3623. doi:10.1158/0008-5472.CAN-07-6497
Fu X, Wan S, Hann HW, Myers RE, Hann RS, Au J, Chen B, Xing J, Yang H (2012) Relative telomere length: a novel non-invasive biomarker for the risk of non-cirrhotic hepatocellular carcinoma in patients with chronic hepatitis B infection. Eur J Cancer 48(7):1014–1022. doi:10.1016/j.ejca.2012.02.066
Svenson U, Ljungberg B, Roos G (2009) Telomere length in peripheral blood predicts survival in clear cell renal cell carcinoma. Cancer Res 69(7):2896–2901. doi:10.1158/0008-5472.CAN-08-3513
Liu HQ, An JZ, Liu J, Yang YF, Zhang HX, Zhao BY, Li JB, Yang HS, Chen ZN, Xing JL (2012) Leukocyte telomere length predicts overall survival in hepatocellular carcinoma treated with transarterial chemoembolization. Carcinogenesis 33(5):1040–1045. doi:10.1093/carcin/bgs098
Chen Y, Qu F, He X, Bao G, Liu X, Wan S, Xing J (2014) Short leukocyte telomere length predicts poor prognosis and indicates altered immune functions in colorectal cancer patients. Ann Oncol : official J Eur Soc Med Oncology/ESMO 25(4):869–876. doi:10.1093/annonc/mdu016
Oh BK, Kim H, Park YN, Yoo JE, Choi J, Kim KS, Lee JJ, Park C (2008) High telomerase activity and long telomeres in advanced hepatocellular carcinomas with poor prognosis. Lab Invest 88(2):144–152. doi:10.1038/labinvest.3700710
Chan DC (2006) Mitochondria: dynamic organelles in disease, aging, and development. Cell 125(7):1241–1252. doi:10.1016/j.cell.2006.06.010
Shadel GS (2008) Expression and maintenance of mitochondrial DNA: new insights into human disease pathology. Am J Pathol 172(6):1445–1456. doi:10.2353/ajpath.2008.071163
Wang Y, Liu VW, Xue WC, Tsang PC, Cheung AN, Ngan HY (2005) The increase of mitochondrial DNA content in endometrial adenocarcinoma cells: a quantitative study using laser-captured microdissected tissues. Gynecol Oncol 98(1):104–110. doi:10.1016/j.ygyno.2005.04.015
Wang Y, Liu VW, Xue WC, Cheung AN, Ngan HY (2006) Association of decreased mitochondrial DNA content with ovarian cancer progression. Br J Cancer 95(8):1087–1091. doi:10.1038/sj.bjc.6603377
Qu F, Liu X, Zhou F, Yang H, Bao G, He X, Xing J (2011) Association between mitochondrial DNA content in leukocytes and colorectal cancer risk: a case-control analysis. Cancer 117(14):3148–3155. doi:10.1002/cncr.25906
Lemnrau A, Brook MN, Fletcher O, Coulson P, Tomczyk K, Jones M, Ashworth A, Swerdlow A, Orr N, Garcia-Closas M (2015) Mitochondrial DNA copy number in peripheral blood cells and risk of developing breast cancer. Cancer Res 75(14):2844–2850. doi:10.1158/0008-5472.CAN-14-1692
Xing J, Chen M, Wood CG, Lin J, Spitz MR, Ma J, Amos CI, Shields PG, Benowitz NL, Gu J, de Andrade M, Swan GE, Wu X (2008) Mitochondrial DNA content: its genetic heritability and association with renal cell carcinoma. J Natl Cancer Inst 100(15):1104–1112. doi:10.1093/jnci/djn213
Hosgood HD 3rd, Liu CS, Rothman N, Weinstein SJ, Bonner MR, Shen M, Lim U, Virtamo J, Cheng WL, Albanes D, Lan Q (2010) Mitochondrial DNA copy number and lung cancer risk in a prospective cohort study. Carcinogenesis 31(5):847–849. doi:10.1093/carcin/bgq045
Zhang J, Li D, Qu F, Chen Y, Li G, Jiang H, Huang X, Yang H, Xing J (2014) Association of leukocyte mitochondrial DNA content with glioma risk: evidence from a Chinese case-control study. BMC Cancer 14:680. doi:10.1186/1471-2407-14-680
Lan Q, Lim U, Liu CS, Weinstein SJ, Chanock S, Bonner MR, Virtamo J, Albanes D, Rothman N (2008) A prospective study of mitochondrial DNA copy number and risk of non-Hodgkin lymphoma. Blood 112(10):4247–4249. doi:10.1182/blood-2008-05-157974
Yuan P, Wang S, Zhou F, Wan S, Yang Y, Huang X, Zhang Z, Zhu Y, Zhang H, Xing J (2014) Functional polymorphisms in the NPAS2 gene are associated with overall survival in transcatheter arterial chemoembolization-treated hepatocellular carcinoma patients. Cancer Sci 105(7):825–832. doi:10.1111/cas.12428
Cawthon RM (2002) Telomere measurement by quantitative PCR. Nucleic Acids Res 30(10):e47
Liu J, Yang Y, Zhang H, Zhao S, Liu H, Ge N, Yang H, Xing JL, Chen Z (2011) Longer leukocyte telomere length predicts increased risk of hepatitis B virus-related hepatocellular carcinoma: a case-control analysis. Cancer 117(18):4247–4256. doi:10.1002/cncr.26015
Zhang C, Chen X, Li L, Zhou Y, Wang C, Hou S (2015) The association between telomere length and cancer prognosis: evidence from a meta-analysis. PLoS One 10(7):e0133174. doi:10.1371/journal.pone.0133174
Svenson U, Roos G (2009) Telomere length as a biological marker in malignancy. Biochim Biophys Acta 1792(4):317–323. doi:10.1016/j.bbadis.2009.01.017
Qu F, Li R, He X, Li Q, Xie S, Gong L, Ji G, Lu J, Bao G (2015) Short telomere length in peripheral blood leukocyte predicts poor prognosis and indicates an immunosuppressive phenotype in gastric cancer patients. Mol Oncol 9(3):727–739. doi:10.1016/j.molonc.2014.11.008
Lin CS, Chang SC, Wang LS, Chou TY, Hsu WH, Wu YC, Wei YH (2010) The role of mitochondrial DNA alterations in esophageal squamous cell carcinomas. J thorac cardiovasc surg 139(1):189–197. doi:10.1016/j.jtcvs.2009.04.007
Guo W, Yang D, Xu H, Zhang Y, Huang J, Yang Z, Chen X, Huang Z (2013) Mutations in the D-loop region and increased copy number of mitochondrial DNA in human laryngeal squamous cell carcinoma. Mol Biol Rep 40(1):13–20. doi:10.1007/s11033-012-1939-7
Cheau-Feng Lin F, Jeng YC, Huang TY, Chi CS, Chou MC, Chin-Shaw Tsai S (2014) Mitochondrial DNA copy number is associated with diagnosis and prognosis of head and neck cancer. Biomarkers 19(4):269–274. doi:10.3109/1354750X.2014.902101
Bekaert S, De Meyer T, Van Oostveldt P (2005) Telomere attrition as ageing biomarker. Anticancer Res 25(4):3011–3021
Tyrka AR, Parade SH, Price LH, Kao HT, Porton B, Philip NS, Welch ES, Carpenter LL (2016) Alterations of mitochondrial DNA copy number and telomere length with early adversity and psychopathology. Biol Psychiatry 79(2):78–86. doi:10.1016/j.biopsych.2014.12.025
Codd V, Mangino M, van der Harst P, Braund PS, Kaiser M, Beveridge AJ, Rafelt S, Moore J, Nelson C, Soranzo N, Zhai G, Valdes AM, Blackburn H, Mateo Leach I, de Boer RA, Kimura M, Aviv A, Wellcome Trust Case Control C, Goodall AH, Ouwehand W, van Veldhuisen DJ, van Gilst WH, Navis G, Burton PR, Tobin MD, Hall AS, Thompson JR, Spector T, Samani NJ (2010) Common variants near TERC are associated with mean telomere length. Nat Genet 42(3):197–199. doi:10.1038/ng.532
Cree LM, Patel SK, Pyle A, Lynn S, Turnbull DM, Chinnery PF, Walker M (2008) Age-related decline in mitochondrial DNA copy number in isolated human pancreatic islets. Diabetologia 51(8):1440–1443. doi:10.1007/s00125-008-1054-4
Short KR, Bigelow ML, Kahl J, Singh R, Coenen-Schimke J, Raghavakaimal S, Nair KS (2005) Decline in skeletal muscle mitochondrial function with aging in humans. Proc Natl Acad Sci USA 102(15):5618–5623. doi:10.1073/pnas.0501559102
Bonner MR, Shen M, Liu CS, DiVita M, He XZ, Lan Q (2009) Mitochondrial DNA content and lung cancer risk in Xuan Wei. China. Lung Cancer 63(3):331–334. doi:10.1016/j.lungcan.2008.06.012
Mengel-From J, Thinggaard M, Dalgard C, Kyvik KO, Christensen K, Christiansen L (2014) Mitochondrial DNA copy number in peripheral blood cells declines with age and is associated with general health among elderly. Hum Genet 133(9):1149–1159. doi:10.1007/s00439-014-1458-9
Miller FJ, Rosenfeldt FL, Zhang C, Linnane AW, Nagley P (2003) Precise determination of mitochondrial DNA copy number in human skeletal and cardiac muscle by a PCR-based assay: lack of change of copy number with age. Nucleic Acids Res 31(11):e61
Kim JH, Kim HK, Ko JH, Bang H, Lee DC (2013) The relationship between leukocyte mitochondrial DNA copy number and telomere length in community-dwelling elderly women. PLoS One 8(6):e67227. doi:10.1371/journal.pone.0067227
Tyrka AR, Carpenter LL, Kao HT, Porton B, Philip NS, Ridout SJ, Ridout KK, Price LH (2015) Association of telomere length and mitochondrial DNA copy number in a community sample of healthy adults. Exp Gerontol 66:17–20. doi:10.1016/j.exger.2015.04.002
Sahin E, Colla S, Liesa M, Moslehi J, Muller FL, Guo M, Cooper M, Kotton D, Fabian AJ, Walkey C, Maser RS, Tonon G, Foerster F, Xiong R, Wang YA, Shukla SA, Jaskelioff M, Martin ES, Heffernan TP, Protopopov A, Ivanova E, Mahoney JE, Kost-Alimova M, Perry SR, Bronson R, Liao R, Mulligan R, Shirihai OS, Chin L, DePinho RA (2011) Telomere dysfunction induces metabolic and mitochondrial compromise. Nature 470(7334):359–365. doi:10.1038/nature09787
Arigami T, Uenosono Y, Matsushita D, Yanagita S, Uchikado Y, Kita Y, Mori S, Kijima Y, Okumura H, Maemura K, Ishigami S, Natsugoe S (2016) Combined fibrinogen concentration and neutrophil-lymphocyte ratio as a prognostic marker of gastric cancer. Oncol Lett 11(2):1537–1544. doi:10.3892/ol.2015.4049
Acknowledgments
This work was supported by the National Natural Science Foundation of China (Grants 81320108021) and the National Basic Research Program of China (Grant 2015CB553703).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
Dengke Bao and Yanna Ba have contributed equally to this work.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Figure 1
Correlation between leukocyte mtDNA copy number and RTL (A), age, and relative telomere length (B) or mtDNA copy number (C). Values of mtDNA copy number were analyzed after log transformation. P values were calculated by Pearson’s correlation (TIFF 3023 kb)
Rights and permissions
About this article

Cite this article
Bao, D., Ba, Y., Zhou, F. et al. Alterations of telomere length and mtDNA copy number are associated with overall survival in hepatocellular carcinoma patients treated with transarterial chemoembolization. Cancer Chemother Pharmacol 78, 791–799 (2016). https://doi.org/10.1007/s00280-016-3128-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-016-3128-1