
Abstract
Purpose
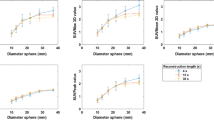
Quantitative measurement of tracer uptake in a tumour can be influenced by a number of factors, including the method of defining regions of interest (ROIs) and the reconstruction parameters used. The main purpose of this study was to determine the effects of different ROI methods on quantitative outcome, using two reconstruction methods and the standard uptake value (SUV) as a simple quantitative measure of FDG uptake.
Methods
Four commonly used methods of ROI definition (manual placement, fixed dimensions, threshold based and maximum pixel value) were used to calculate SUV (SUV[MAN], SUV15 mm, SUV50, SUV75 and SUVmax, respectively) and to generate “metabolic” tumour volumes. Test–retest reproducibility of SUVs and of “metabolic” tumour volumes and the applicability of ROI methods during chemotherapy were assessed. In addition, SUVs calculated on ordered subsets expectation maximisation (OSEM) and filtered back-projection (FBP) images were compared.
Results
ROI definition had a direct effect on quantitative outcome. On average, SUV[MAN], SUV15 mm, SUV50 and SUV75, were respectively 48%, 27%, 34% and 15% lower than SUVmax when calculated on OSEM images. No statistically significant differences were found between SUVs calculated on OSEM and FBP reconstructed images. Highest reproducibility was found for SUV15 mm and SUV[MAN] (ICC 0.95 and 0.94, respectively) and for “metabolic” volumes measured with the manual and 50% threshold ROIs (ICC 0.99 for both). Manual, 75% threshold and maximum pixel ROIs could be used throughout therapy, regardless of changes in tumour uptake or geometry. SUVs showed the same trend in relative change in FDG uptake after chemotherapy, irrespective of the ROI method used.
Conclusion
The method of ROI definition has a direct influence on quantitative outcome. In terms of simplicity, user-independence, reproducibility and general applicability the threshold-based and fixed dimension methods are the best ROI methods. Threshold methods are in addition relatively independent of changes in size and geometry, however, and may therefore be more suitable for response monitoring purposes.



Similar content being viewed by others


References
Dimitrakopoulou-Strauss A, Strauss LG, Heichel T, et al. The role of quantitative 18F-FDG PET studies for the differentiation of malignant and benign bone lesions. J Nucl Med 2002;43:510–8
Avril N, Bense S, Ziegler SI, et al. Breast imaging with fluorine-18-FDG PET: quantitative image analysis. J Nucl Med 1997;38:1186–91
Smith IC, Welch AE, Hutcheon AW, et al. Positron emission tomography using [18F]-fluorodeoxy-d-glucose to predict the pathologic response of breast cancer to primary chemotherapy. J Clin Oncol 2000;18:1676–88
Sugawara Y, Zasadny KR, Neuhoff AW, Wahl RL. Reevaluation of the standardized uptake value for FDG: variations with body weight and methods for correction. Radiology1999;213:521–5
Schelling M, Avril N, Nahrig J, et al. Positron emission tomography using [18F]fluorodeoxyglucose for monitoring primary chemotherapy in breast cancer. J Clin Oncol 2000;18:1689–95
Romer W, Hanauske AR, Ziegler S, et al. Positron emission tomography in non-Hodgkin’s lymphoma: assessment of chemotherapy with fluorodeoxyglucose. Blood 1998;91:4464–71
Choi NC, Fischman AJ, Niemierko A, et al. Dose-response relationship between probability of pathologic tumour control and glucose metabolic rate measured with FDG PET after preoperative chemoradiotherapy in locally advanced non-small-cell lung cancer. Int J Radiat Oncol Biol Phys 2002;54:1024–35
Brun E, Kjellen E, Tennvall J, et al. FDG PET studies during treatment: prediction of therapy outcome in head and neck squamous cell carcinoma. Head Neck 2002;24:127–35
Weber WA, Ziegler SI, Thodtmann R, et al. Reproducibility of metabolic measurements in malignant tumours using FDG PET. J Nucl Med 1999;40:1771–7
Lee JR, Madsen MT, Bushnel D, et al. A threshold method to improve standardized uptake value reproducibility. Nucl Med Commun 2000; 21:685–90
Graham MM, Peterson LM, Hayward RM. Comparison of simplified quantitative analyses of FDG uptake. Nucl Med Biol 2000;7:647–55
Hunter GJ, Hamberg LM, Alpert NM, et al. Simplified measurement of deoxyglucose utilization rate. J Nucl Med 1996;37:950–5
Kole AC, Nieweg OE, Pruim J, et al. Standardized uptake value and quantification of metabolism for breast cancer imaging with FDG and l-[1-11C]tyrosine PET. J Nucl Med 1997;38:692–6
Avril N, Dose J, Janicke F, et al. Metabolic characterization of breast tumours with positron emission tomography using F-18 fluorodeoxyglucose. J Clin Oncol 1996;14:1848–57
Nakamoto Y, Zasadny KR, Minn H, et al. Reproducibility of common semi-quantitative parameters for evaluating lung cancer glucose metabolism with positron emission tomography using 2-deoxy-2-[18F]fluoro-d-glucose. Mol Imaging Biol 2002;4:171–8
Chin BB, Lyengar S, Sabundayo BP, et al. Standardized uptake values in 2-deoxy-2-[18F]fluoro-d-glucose with positron emission tomography: clinical significance of iterative reconstruction and segmented attenuation compared with conventional filtered back projection and measured attenuation correction. Mol Imaging Biol 2002;4:294–300
Visvikis D, Cheze-LeRest C, Costa DC, et al. Influence of OSEM and segmented attenuation correction in the calculation of standardised uptake values for [18F]FDG PET. Eur J Nucl Med 2001;28:1326–35
Boellaard R, Krak NC, Hoekstra OS, et al. Effects of noise, image resolution and ROI definition on the accuracy of standard uptake values: a simulation study. J Nucl Med 2004;45:1519–27
Hoekstra CJ, Hoekstra OS, Stroobants SG, et al. Methods to monitor response to chemotherapy in non-small cell lung cancer with 18F-FDG PET. J Nucl Med 2002;43:1304–09
Boellaard R, van Lingen A, Lammertsma AA. Experimental and clinical evaluation of iterative reconstruction (OSEM) in dynamic PET: quantitative characteristics and effects on kinetic modeling. J Nucl Med 2001;42:808–17
Hoekstra CJ, Paglianiti I, Hoekstra OS, et al. Monitoring response to therapy in cancer using [18F]-2-fluoro-2-deoxy-d-glucose and positron emission tomography: an overview of different analytical methods. Eur J Nucl Med 2000;27:731–43
Yang SN, Liang JA, Lin FJ, et al. Differentiating benign and malignant pulmonary lesions with FDG-PET. Anticancer Res 2001;21:4153–57
Hubner KF, Buonocore E, Gould HR, et al. Differentiating benign from malignant lung lesions using “quantitative” parameters of FDG PET images. Clin Nucl Med 1996;21:941–9
Minn H, Zasadny KR, Quint LE, et al. Lung cancer: reproducibility of quantitative measurements for evaluating 2-[F-18]-fluoro-2-deoxy-d-glucose uptake at PET. Radiology 1995;196:167–73
Weber WA, Ziegler SI, Thodtmann R, Hanauske AR, Schwaiger M. Reproducibility of metabolic measurements in malignant tumours using FDG PET. J Nucl Med 1999;40:1771–7
Wahl RL, Zasadny K, Helvie M, et al. Metabolic monitoring of breast cancer chemohormonotherapy using positron emission tomography: initial evaluation. J Clin Oncol 1993;11:2101–11
Mankoff DA, Dunwald LK, Gralow JR, et al. Changes in blood flow and metabolism in locally advanced breast cancer treated with neoadjuvant chemotherapy. J Nucl Med 2003;44:1806–14
Jansson T, Westlin JE, Ahlstrom H, et al. Positron emission tomography studies in patients with locally advanced and/or metastatic breast cancer: a method for early therapy evaluation? J Clin Oncol 1995;13:1470–7
Zasadny KR, Kison PV, Fransis IR, et al. FDG-PET determination of metabolically active tumour volume and comparison with CT. Clin Pos Imaging 1998;1:123–9
Erdi YE, Mawlawi O, Larson SM, et al. Segmentation of lung lesion volume by adaptive positron emission tomography image thresholding. Cancer1997;15:2505–9
Young H, Baum R, Cremerius U, et al. Measurement of clinical and subclinical tumour response using [18F]-fluorodeoxyglucose and positron emission tomography: review and 1999 EORTC recommendations. European Organization for Research and Treatment of Cancer (EORTC) PET Study Group. Eur J Cancer 1999;35:1773–82
Keyes JW Jr. SUV: standard uptake or silly useless value? J Nucl Med 1995;36:1836–9
Ramos CD, Erdi YE, Gonen M, et al. FDG-PET standardized uptake values in normal anatomical structures using iterative reconstruction segmented attenuation correction and filtered back-projection. Eur J Nucl Med 2001;28:155–64
Etchebehere EC, Macapinlac HA, Gonen M, et al. Qualitative and quantitative comparison between images obtained with filtered back projection and iterative reconstruction in prostate cancer lesions of 18«F-FDG PET. Q J Nucl Med 2002;46:122–30
Lonneux M, Borbath I, Bol A, et al. Attenuation correction in whole-body FDG oncological studies: the role of statistical reconstruction. Eur J Nucl Med 1999;26:591–8
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s00259-005-1926-5
Rights and permissions
About this article
Cite this article
Krak, N.C., Boellaard, R., Hoekstra, O.S. et al. Effects of ROI definition and reconstruction method on quantitative outcome and applicability in a response monitoring trial. Eur J Nucl Med Mol Imaging 32, 294–301 (2005). https://doi.org/10.1007/s00259-004-1566-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-004-1566-1