
Abstract
Summary
Among 62,275 women and 6455 men, FRAX stratified risk for incident major osteoporotic fracture (MOF) and incident hip fracture (HF) without sex interaction. Performance was good in those with osteoporosis regardless of how this was defined.
Introduction
Some studies have reported that FRAX performance differs according to sex and/or osteoporosis definitions. We evaluated whether the performance of FRAX to predict incident MOF and HF in women and men was affected by the presence or absence of osteoporosis defined by World Health Organization (WHO) or National Osteoporosis Foundation (NOF) criteria.
Methods
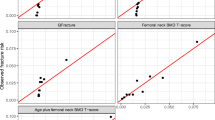
We studied women and men age ≥ 40 years with baseline hip and spine DXA scans (1996–2013). Individuals were classified into four non-overlapping subgroups: osteoporosis by WHO criteria, osteoporosis exclusively by NOF criteria, high fracture risk by FRAX (MOF ≥ 20% or HF ≥ 3%, without osteoporosis), and low fracture risk (MOF < 20% and HF < 3% without osteoporosis). In each subgroup, we evaluated stratification (hazard ratios [HR]) and calibration (observed vs predicted 10-year fracture probability) for incident fracture.
Results
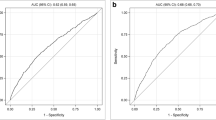
The population included 62,275 women (5345 MOF and 1471 HF) and 6455 men (405 MOF and 108 HF). FRAX scores were strongly predictive of MOF (HR per SD: women 2.12, 95% CI 2.06–2.18; men 1.89, 95% CI 1.73–2.08; sex interaction p value = 0.97) and HF (women 4.78, 95% CI 4.44–5.14; men 4.20, 95% CI 3.22–5.49; sex interaction p value = 0.71). FRAX scores gave similar HRs for MOF among the four subgroups (subgroup interaction p value 0.34 for women, 0.22 for men). Observed versus predicted 10-year MOF and HF probability for the defined subgroups demonstrated a high level of concordance for women and men (all r2 ≥ 0.9).
Conclusions
FRAX was a strong and consistent predictor of MOF and HF in both women and men and performed well in those with osteoporosis whether defined by WHO or NOF criteria.


Similar content being viewed by others

References
Consensus Development Panel NIH (2001) Osteoporosis prevention, diagnosis, and therapy. JAMA 285:785–795
Kanis JA, Cooper C, Rizzoli R et al (2017) Identification and management of patients at increased risk of osteoporotic fracture: outcomes of an ESCEO expert consensus meeting. Osteoporos Int 28:2023–2034
Williamson S, Landeiro F, McConnell T et al (2017) Costs of fragility hip fractures globally: a systematic review and meta-regression analysis. Osteoporos Int 28:2791–2800
MacLean C, Newberry S, Maglione M et al (2008) Systematic review: comparative effectiveness of treatments to prevent fractures in men and women with low bone density or osteoporosis. Ann Intern Med 148:197–213
Hopkins RB, Goeree R, Pullenayegum E et al (2011) The relative efficacy of nine osteoporosis medications for reducing the rate of fractures in post-menopausal women. BMC Musculoskelet Disord 12:209
Leslie WD, Lix LM (2014) Comparison between various fracture risk assessment tools. Osteoporos Int 25(1):1–21. https://doi.org/10.1007/s00198-013-2409-3
Kanis JA, on behalf of the World Health Organization Scientific Group. Assessment of osteoporosis at the primary health-care level. Technical Report. Accessible at http://www.shef.ac.uk/FRAX/pdfs/WHO_Technical_Report.pdf. 2007. Published by the University of Sheffield
Kanis JA, Johnell O, Oden A et al (2000) Long-term risk of osteoporotic fracture in Malmo. Osteoporos Int 11:669–674
Satagopan JM, Ben-Porat L, Berwick M et al (2004) A note on competing risks in survival data analysis. Br J Cancer 91:1229–1235
Kanis JA, Harvey NC, Cooper C et al (2016) A systematic review of intervention thresholds based on FRAX: a report prepared for the National Osteoporosis Guideline Group and the International Osteoporosis Foundation. Arch Osteoporos 11(1):25–0278. https://doi.org/10.1007/s11657-016-0278-z
Sandhu SK, Nguyen ND, Center JR, Pocock NA, Eisman JA, Nguyen TV (2010) Prognosis of fracture: evaluation of predictive accuracy of the FRAX algorithm and Garvan nomogram. Osteoporos Int 21(5):863–871. https://doi.org/10.1007/s00198-009-1026-7
Ensrud KE, Taylor BC, Peters KW, Gourlay ML, Donaldson MG, Leslie WD, Blackwell TL, Fink HA, Orwoll ES, Schousboe J, for the Osteoporotic Fractures in Men (MrOS) Study Group (2014) Implications of expanding indications for drug treatment to prevent fracture in older men in United States: cross sectional and longitudinal analysis of prospective cohort study. BMJ 349(jul03 5):g4120. https://doi.org/10.1136/bmj.g4120
Leslie WD, MacWilliam L, Lix L et al (2005) A population-based study of osteoporosis testing and treatment following introduction of a new bone densitometry service. Osteoporos Int 16:773–782
Leslie WD, Caetano PA, MacWilliam LR, Finlayson GS (2005) Construction and validation of a population-based bone densitometry database. J Clin Densitom 8(1):25–30. https://doi.org/10.1385/JCD:8:1:025
Looker AC, Wahner HW, Dunn WL, Calvo MS, Harris TB, Heyse SP, Johnston CC Jr, Lindsay R (1998) Updated data on proximal femur bone mineral levels of US adults. Osteoporos Int 8(5):468–489. https://doi.org/10.1007/s001980050093
Kanis JA, McCloskey EV, Johansson H, Oden A, Melton LJ III, Khaltaev N (2008) A reference standard for the description of osteoporosis. Bone 42(3):467–475. https://doi.org/10.1016/j.bone.2007.11.001
Cosman F, de Beur SJ, Leboff MS et al (2014) Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int 25(10):2359–2381. https://doi.org/10.1007/s00198-014-2794-2
Leslie WD, Lix LM, Langsetmo L, Berger C, Goltzman D, Hanley DA, Adachi JD, Johansson H, Oden A, McCloskey E, Kanis JA (2011) Construction of a FRAX((R)) model for the assessment of fracture probability in Canada and implications for treatment. Osteoporos Int 22(3):817–827. https://doi.org/10.1007/s00198-010-1464-2
Leslie WD, Lix LM, Johansson H, Oden A, McCloskey E, Kanis JA, Manitoba Bone Density Program (2010) Independent clinical validation of a Canadian FRAX tool: fracture prediction and model calibration. J Bone Miner Res 25(11):2350–2358. https://doi.org/10.1002/jbmr.123
Fraser LA, Langsetmo L, Berger C et al (2011) Fracture prediction and calibration of a Canadian FRAX(R) tool: a population-based report from CaMos. Osteoporos Int 22:829–837
Dagan N, Cohen-Stavi C, Leventer-Roberts M et al (2017) External validation and comparison of three prediction tools for risk of osteoporotic fractures using data from population based electronic health records: retrospective cohort study. BMJ 356:i6755. https://doi.org/10.1136/bmj.i6755.:i6755
WHO Collaborating Centre for Drug Statistics Methodology. (eds) (2005) Guidelines for ATC classification and DDD assignment. Oslo
Leslie WD, Lix LM, Johansson H, Oden A, McCloskey E, Kanis JA, for the Manitoba Bone Density Program (2012) Does osteoporosis therapy invalidate FRAX for fracture prediction? J Bone Miner Res 27(6):1243–1251. https://doi.org/10.1002/jbmr.1582
Leslie WD, Tsang JF, Caetano PA, Lix LM, Manitoba Bone Density Program (2007) Effectiveness of bone density measurement for predicting osteoporotic fractures in clinical practice. J Clin Endocrinol Metab 92(1):77–81. https://doi.org/10.1210/jc.2006-1415
Roos NP, Shapiro E (1999) Revisiting the Manitoba Centre for Health Policy and Evaluation and its population-based health information system. Med Care 37(6 Suppl):JS10–JS14
Leslie WD, Lix LM, Wu X (2013) Competing mortality and fracture risk assessment. Osteoporos Int 24(2):681–688. https://doi.org/10.1007/s00198-012-2051-5
Marshall D, Johnell O, Wedel H (1996) Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ 312:1254–1259
Stone KL, Seeley DG, Lui LY, Cauley JA, Ensrud K, Browner WS, Nevitt MC, Cummings SR, Osteoporotic Fractures Research Group (2003) BMD at multiple sites and risk of fracture of multiple types: long-term results from the Study of Osteoporotic Fractures. J Bone Miner Res 18(11):1947–1954. https://doi.org/10.1359/jbmr.2003.18.11.1947
Schuit SC, van der Klift M, Weel AE et al (2004) Fracture incidence and association with bone mineral density in elderly men and women: the Rotterdam study. Bone 34(1):195–202. https://doi.org/10.1016/j.bone.2003.10.001
Siris ES, Chen YT, Abbott TA, Barrett-Connor E, Miller PD, Wehren LE, Berger ML (2004) Bone mineral density thresholds for pharmacological intervention to prevent fractures. Arch Intern Med 164(10):1108–1112. https://doi.org/10.1001/archinte.164.10.1108
Leslie WD, Rubin MR, Schwartz AV, Kanis JA (2012) Type 2 diabetes and bone. J Bone Miner Res 27(11):2231–2237. https://doi.org/10.1002/jbmr.1759
Shepherd JA, Schousboe JT, Broy SB, Engelke K, Leslie WD (2015) Executive summary of the 2015 ISCD position development conference on advanced measures from DXA and QCT: fracture prediction beyond BMD. J Clin Densitom 18(3):274–286. https://doi.org/10.1016/j.jocd.2015.06.013
Lix LM, Azimaee M, Osman BA et al (2012) Osteoporosis-related fracture case definitions for population-based administrative data. BMC Public Health 12:301
O'Donnell S (2013) Use of administrative data for national surveillance of osteoporosis and related fractures in Canada: results from a feasibility study. Arch Osteoporos 8(143)
Acknowledgments
The authors acknowledge the Manitoba Centre for Health Policy for use of data contained in the Population Health Research Data Repository (HIPC 2011/2012-31). The results and conclusions are those of the authors, and no official endorsement by the Manitoba Centre for Health Policy, Manitoba Health, Seniors and Active Living, or other data providers is intended or should be inferred. This article has been reviewed and approved by the members of the Manitoba Bone Density Program Committee.
Funding
No funding support was received for this research project. SNM is chercheur-clinicienne boursier des Fonds de Recherche du Québec en Santé. LML is supported by a Manitoba Health Research Chair. SRM holds the Endowed Chair in Patient Health Management supported by the Faculties of Medicine and Dentistry and Pharmacy and Pharmaceutical Sciences at the University of Alberta.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by the Health Research Ethics Board for the University of Manitoba.
Conflicts of interest
Suzanne Morin: Research Grants: Amgen, Merck.
Eugene McCloskey: Nothing to declare for FRAX and the context of this paper, but numerous ad hoc consultancies/speaking honoraria and/or research funding from Amgen, Bayer, General Electric, GSK, Hologic, Lilly, Merck Research Labs, Novartis, Novo Nordisk, Nycomed, Ono, Pfizer, ProStrakan, Roche, Sanofi-Aventis, Servier, Tethys, UBS, and Warner-Chilcott.
John A. Kanis: Grants from Amgen, grants from Lilly, non-financial support from Medimaps, grants from Unigene, non-financial support from Asahi, and grants from Radius Health, outside the submitted work. Dr. Kanis is the architect of FRAX but has no financial interest. Governmental and NGOs: National Institute for health and clinical Excellence (NICE), UK; International Osteoporosis Foundation; INSERM, France; Ministry of Public Health, China; Ministry of Health, Australia; Ministry of Health, Abu Dhabi; National Osteoporosis Guideline Group, UK; WHO.
William Leslie, Sumit Majumdar, Lisa Lix, H. Johansson, John T. Schousboe, Kristine E. Ensrud: None.
Electronic supplementary material
ESM 1
(DOCX 39 kb)
Rights and permissions
About this article

Cite this article
Leslie, W.D., Majumdar, S.R., Morin, S.N. et al. Performance of FRAX in clinical practice according to sex and osteoporosis definitions: the Manitoba BMD registry. Osteoporos Int 29, 759–767 (2018). https://doi.org/10.1007/s00198-018-4415-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-018-4415-y