
Abstract
Summary
After the implementation of the multidisciplinary geriatric hip fracture clinical pathway in 2007, the hospital length of stay and the clinical outcomes improves. Moreover, the cost of manpower for each hip fracture decreases. It proves that this care model is cost-effective.
Introduction
The objective of this study is to compare the clinical outcomes and the cost of manpower before and after the implementation of the multidisciplinary geriatric hip fracture clinical pathway (GHFCP).
Methods
The hip fracture data from 2006 was compared with the data of four consecutive years since 2008. The efficiency of the program is assessed using the hospital length of stay. The clinical outcomes include mortality rates and complication rates are compared. Cost of manpower was also analysed.
Results
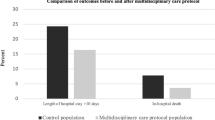
After the implementation of the GHFCP, the preoperative length of stay shortened significantly from 5.8 days in 2006 to 1.3 days in 2011. The total length of stay in both acute and rehabilitation hospitals were also shortened by 6.1 days and 14.2 days, respectively. The postoperative pneumonia rate also decreased from 1.25 to 0.25%. The short- and long-term mortalities also showed a general improvement. Despite allied health manpower was increased to meet the increased workload, the shortened length of stay accounted for a mark decrease in cost of manpower per hip fracture case.
Conclusion
This study proves that the GHFCP shortened the geriatric hip fracture patients’ length of stay and improves the clinical outcomes. It is also cost-effective which proves better care is less costly.



Similar content being viewed by others

References
Parker M, Johansen A (2006) Hip fracture. BMJ 333(7557):27–30
Royal College of Physicians (1999) Osteoporosis. Clinical guidelines for prevention and treatment. Royal College of Physicians of London, London
Clague JE et al (2002) Predictors of outcome following hip fracture. Admission time predicts length of stay and in-hospital mortality. Injury 33(1):1–6
Kates SL, Kates OS, Mendelson DA (2007) Advances in the medical management of osteoporosis. Injury 38(Suppl 3):S17–S23
Brown CA, Starr AZ, Nunley JA (2012) Analysis of past secular trends of hip fractures and predicted number in the future 2010–2050. J Orthop Trauma 26(2):117–122
Gauthier A, Kanis JA, Jiang Y et al (2012) Burden of postmenopausal osteoporosis in Germany: estimations from a disease model. Arch Osteoporos 7(1–2):209–218
Cooper C, Cole ZA, Holroyd CR, Earl SC, Harvey NC, Dennison EM, Melton LJ, Cummings SR, Kanis JA, IOF CSA Working Group on Fracture Epidemiology (2011) Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos Int 22:1277–1288
Kenzora JE et al (1984) Hip fracture mortality: relation to age, treatment, preoperative illness, time of surgery, and complications. Clin Orthop Relat Res 186:45–56
Roche JJ et al (2005) Effect of comorbidities and postoperative complications on mortality after hip fracture in elderly people: prospective observational cohort study. BMJ 331(7529):1374
Forni S, Pieralli F, Sergi A, Lorini C, Bonaccorsi G, Vannucci A (2016) Mortality after hip fracture in the elderly: the role of a multidisciplinary approach and time to surgery in a retrospective observational study on 23,973 patients. Arch Gerontol Geriatr 66:13–17
Kristensen PK, Thillemann TM, Søballe K, Johnsen SP (2016) Can improved quality of care explain the success of orthogeriatric units? A population-based cohort study. Age Ageing 45(1):66–71
Brainsky A et al (1997) The economic cost of hip fractures in community-dwelling older adults: a prospective study. J Am Geriatr Soc 45(3):281–287
Johnell O, Kanis J (2005) Epidemiology of osteoporotic fractures. Osteoporos Int 16(Suppl 2):S3–S7
Gholve PA et al (2005) Multidisciplinary integrated care pathway for fractured neck of femur. a prospective trial with improved outcome. Injury 36(1):93–98 discussion 99
Friedman SM et al (2008) Geriatric co-management of proximal femur fractures: total quality management and protocol-driven care result in better outcomes for a frail patient population. J Am Geriatr Soc 56(7):1349–1356
Choong PF et al (2000) Clinical pathway for fractured neck of femur: a prospective, controlled study. Med J Aust 172(9):423–426
Lau TW, Leung F, Siu D, Wong G, Luk KD (2010) Geriatric hip fracture clinical pathway: the Hong Kong experience. Osteoporos Int 21(Suppl 4):S627–S636
Beaupre LA et al (2006) Reduced morbidity for elderly patients with a hip fracture after implementation of a perioperative evidence-based clinical pathway. Qual Saf Health Care 15(5):375–379
Roberts HC et al (2004) The effectiveness of implementing a care pathway for femoral neck fracture in older people: a prospective controlled before and after study. Age Ageing 33(2):178–184
British Orthopaedic Association (2007) The Care of Fragility Fracture Patients. British Orthopaedic Association, London
Fergus L, Cutfield G, Harris R (2011) Auckland City Hospital’s ortho-geriatric service: an audit of patients aged over 65 with fractured neck of femur. N Z Med J 124(1337):40–54
Bottle A, Aylin P (2006) Mortality associated with delay in operation after hip fracture: observational study. BMJ 332(7547):947–951
Moran CG et al (2005) Early mortality after hip fracture: is delay before surgery important? J Bone Joint Surg Am 87(3):483–489
Leung AH et al (2011) An orthogeriatric collaborative intervention program for fragility fractures: a retrospective cohort study. J Trauma 71(5):1390–1394
Neuman MD et al (2009) The relationship between short-term mortality and quality of care for hip fracture: a meta-analysis of clinical pathways for hip fracture. J Am Geriatr Soc 57(11):2046–2054
Lawrence TM, White CT, Wenn R, Moran CG (2005) The current hospital costs of treating hip fractures. Injury 36(1):88–91
Kates SL, Mendelson DA, Friedman SM (2011) The value of an organized fracture program for the elderly: early results. J Orthop Trauma 25(4):233–237
Switzer JA, Jaglal S, Bogoch ER (2009) Overcoming barriers to osteoporosis care in vulnerable elderly patients with hip fractures. J Orthop Trauma 23(6):454–459
Marsland D, Colvin PL, Mears SC, Kates SL (2010) How to optimize patients for geriatric fracture surgery. Osteoporos Int 21(Suppl 4):S535–S546
Acknowledgments
I would like to thank Ms. Win Lui, Ms. Karen Yip, Ms. Wong Ka Wah, Ms. Christo Chew from the Performance office and Finance division of Queen Mary Hospital who contributed and made tremendous effort on data capturing and processing. I would also like to thank Ms. Teresa Kwan, the case manager of the Geriatric Hip Fracture Clinical Pathway, who has also spent a lot of effort in keeping the clinical pathway running smoothly and providing accurate data auditing.
This research was supported by the Health and Medical Research Fund (project no. 111122031) to the Department of Orthopaedics and Traumatology, the University of Hong Kong.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Rights and permissions
About this article

Cite this article
Lau, T.W., Fang, C. & Leung, F. The effectiveness of a multidisciplinary hip fracture care model in improving the clinical outcome and the average cost of manpower. Osteoporos Int 28, 791–798 (2017). https://doi.org/10.1007/s00198-016-3845-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-016-3845-7