
Abstract
Summary
Children who sustain a forearm fracture when injured have lower bone density throughout their skeleton, and have a smaller cortical area and a lower strength index in their radius. Odds ratios per SD decrease in bone characteristics measured by peripheral quantitative computed tomography (pQCT) and dual-energy X-ray absorptiometry (DXA) were similar (1.28 to 1.41).
Introduction
Forearm fractures are common in children. Bone strength is affected by bone mineral density (BMD) and bone geometry, including cross-sectional dimensions and distribution of mineral. Our objective was to identify bone characteristics that differed between children who sustained a forearm fracture compared to those who did not fracture when injured.
Methods
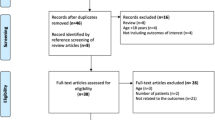
Children (5–16 years) with a forearm fracture (cases, n = 224) and injured controls without fracture (n = 200) were enrolled 28 ± 8 days following injury. Peripheral QCT scans of the radius (4% and 20% sites) were obtained to measure volumetric BMD (vBMD) of total, trabecular and cortical bone compartments, and bone geometry (area, cortical thickness, and strength strain index [SSI]). DXA scans (forearm, spine, and hip) were obtained to measure areal BMD (aBMD) and bone area. Receiver operating characteristic (ROC) analyses were used to assess screening performance of bone measurements.
Results
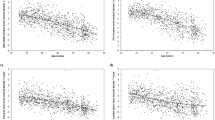
At the 4% pQCT site, total vBMD, but not trabecular vBMD or bone area, was lower (−3.4%; p = 0.02) in cases than controls. At the 20% site, cases had lower cortical vBMD (−0.9%), cortical area (−2.8%), and SSI (−4.6%) (p < 0.05). aBMD, but not bone area, at the 1/3 radius, spine, and hip were 2.7–3.3% lower for cases (p < 0.01). Odds ratios per 1 SD decrease in bone measures (1.28–1.41) and areas under the ROC curves (0.56–0.59) were similar for all bone measures.
Conclusions
Low vBMD, aBMD, cortical area, and SSI of the distal radius were associated with an increased fracture risk. Interventions to increase these characteristics are needed to help reduce forearm fracture occurrence.

Similar content being viewed by others

References
Jones IE, Williams SM, Dow N, Goulding A (2002) How many children remain fracture-free during growth? A longitudinal study of children and adolescents participating in the Dunedin Multidisciplinary Health and Development Study. Osteoporos Int 13:990–995
Cooper C, Dennison EM, Leufkens HG, Bishop N, van Staa TP (2004) Epidemiology of childhood fractures in Britain: a study using the general practice research database. J Bone Miner Res 19:1976–1981
Jones IE, Cannan R, Goulding A (2000) Distal forearm fractures in New Zealand children: annual rates in a geographically defined area. N Z Med J 113:443–445
Khosla S, Melton LJ 3rd, Dekutoski MB, Achenbach SJ, Oberg AL, Riggs BL (2003) Incidence of childhood distal forearm fractures over 30 years: a population-based study. JAMA 290:1479–1485
Goulding A, Cannan R, Williams SM, Gold EJ, Taylor RW, Lewis-Barned NJ (1998) Bone mineral density in girls with forearm fractures. J Bone Miner Res 13:143–148
Goulding A, Jones IE, Taylor RW, Williams SM, Manning PJ (2001) Bone mineral density and body composition in boys with distal forearm fractures: a dual-energy X-ray absorptiometry study. J Pediatr 139:509–515
Manias K, McCabe D, Bishop N (2006) Fractures and recurrent fractures in children; varying effects of environmental factors as well as bone size and mass. Bone 39:652–657
Clark EM, Ness AR, Tobias JH (2008) Vigorous physical activity increases fracture risk in children irrespective of bone mass: a prospective study of the independent risk factors for fractures in healthy children. J Bone Miner Res 23:1012–1022
Bouxsein ML, Karasik D (2006) Bone geometry and skeletal fragility. Curr Osteoporos Rep 4:49–56
Jones G, Boon P (2008) Which bone mass measures discriminate adolescents who have fractured from those who have not? Osteoporos Int 19:251–255
Ferrari SL, Chevalley T, Bonjour JP, Rizzoli R (2006) Childhood fractures are associated with decreased bone mass gain during puberty: an early marker of persistent bone fragility? J Bone Miner Res 21:501–507
Goulding A, Grant AM, Williams SM (2005) Bone and body composition of children and adolescents with repeated forearm fractures. J Bone Miner Res 20:2090–2096
Skaggs DL, Loro ML, Pitukcheewanont P, Tolo V, Gilsanz V (2001) Increased body weight and decreased radial cross-sectional dimensions in girls with forearm fractures. J Bone Miner Res 16:1337–1342
Cheng S, Xu L, Nicholson PHF, Tylavsky FA, Lyytikainen A, Wang Q, Suominen H, Kujala UM, Kroger H, Alen M (2009) Low volumetric BMD is linked to upper-limb fracture in pubertal girls and persists into adulthood: a seven-year cohort study. Bone 45:480–486
Darelid A, Ohlsson C, Rudang R, Kindblom JM, Mellstrom D, Lorentzon M (2009) Trabecular volumetric bone mineral density is associated with previous fracture during childhood and adolescence in males—the GOOD study. J Bone Miner Res 25:537–544
Neu CM, Manz F, Rauch R, Merkel A, Schoenau E (2001) Bone densities and bone size at the distal radius in healthy children and adolescents: a study using peripheral quantitative computed tomography. Bone 28:227–232
Kontulainen S, Liu D, Manske S, Jamieson M, Sievanen H, McKay H (2007) Analyzing cortical bone cross-sectional geometry by peripheral QCT: comparison with bone histomorphometry. J Clin Densitom 10:86–92
Ward KA, Adams JE, Hangartner TN (2005) Recommendations for thresholds for cortical bone geometry and density measurement by peripheral quantitative computed tomography. Calcif Tissue Int 77:275–280
Taylor A, Konrad PT, Norman ME, Karcke HT (1997) Total body bone mineral density in young children: influence of head bone mineral density. J Bone Miner Res 12:652–655
Landin LA (1983) Fracture patterns in children. Acta Orthop Scand Suppl 54:1–109
Clark EM, Ness AR, Tobias JH (2008) Bone fragility contributes to the risk of fracture in children, even after moderate and severe trauma. J Bone Miner Res 23:173–179
Ogden CL, Kuczmarski RJ, Flegal KM, Mei Z, Guo S, Wei R, Grummer-Strawn LM, Curtin LR, Roche AF, Johnson CL (2002) Centers for Disease Control and Prevention 2000 growth charts for the United States: improvements to the 1977 National Center for Health Statistics version. Pediatrics 109:45–60
Tanner JM (1962) Growth at adolescence. Blackwell Scientific, Oxford
Schoenau E, Neu CM, Rauch R, Manz F (2002) Gender-specific pubertal changes in volumetric cortical bone mineral density at the proximal radius. Bone 31:110–113
Cole TJ (2000) Sympercents: symmetric percentage differences on the 100 log(e) scale simplify the presentation of log transformed data. Stat Med 19:3109–3125
Spadaro JA, Werner FW, Brenner RA, Fortino MD, Fay LA, Edwards WT (1994) Cortical and trabecular bone contribute strength to the osteopenic distal radius. J Orthop Res 12:211–218
Sornay-Rendu E, Boutroy S, Munoz F, Delmas PD (2007) Alterations of cortical and trabecular architecture are associated with fractures in postmenopausal women, partially independent of decreased BMD measured by DXA: the OFELY study. J Bone Miner Res 22:425–433
Pritchett J (1991) Growth plate activity in the upper extremity. Clin Orthop 268:235–242
Rauch F, Neu C, Manz F, Schoenau E (2001) The development of metaphyseal cortex—implications for distal radius fractures during growth. J Bone Miner Res 16:1547–1555
Kirmani S, Christen D, vanLenthe GH, Fischer PR, Bouxsein ML, McCready LK, Melton LJ 3rd, Riggs BL, Amin S, Muller R, Khosla S (2009) Bone structure at the distal radius during adolescent growth. J Bone Miner Res 24:1033–1042
Parfitt AM (1994) The two faces of growth: benefits and risks to bone integrity. Osteoporos Int 4:382–398
Ducher G, Courteix D, Meme S, Magni C, Viala JF, Benhamou SL (2005) Bone geometry in response to long-term tennis playing and its relationship with muscle volume: a quantitative magnetic resonance imaging study in tennis players. Bone 37:457–466
Muller ME, Webber CE, Bouxsein ML (2003) Predicting the failure load of the distal radius. Osteoporos Int 14:345–352
Jones G, Ma D, Cameron F (2006) Bone density interpretation and relevance in Caucasian children aged 9–17 years of age: insights from a population-based fracture study. J Clin Densitom 9:202–209
Johnell O, Kanis JA, Oden A, Johansson H, De Laet C, Delmas P, Eisman JA, Fujiwara S, Kroger H, Mellstrom D, Meunier PJ, Melton LJ 3rd, O’Neill T, Pols H, Reeve J, Silman A, Tenenhouse A (2005) Predictive value of BMD for hip and other fractures. J Bone Miner Res 20:1185–1194
Goulding A, Jones IE, Taylor RW, Manning PJ, Williams SM (2000) More broken bones: a 4-year double cohort study of young girls with and without distal forearm fractures. J Bone Miner Res 15:2011–2018
Goulding A, Jones IE, Taylor RW, Piggot JM, Taylor D (2003) Dynamic and static tests of balance and postural sway in boys: effects of previous wrist bone fractures and high adiposity. Gait Posture 17:136–141
Goulding A, Rockell JE, Black RE, Grant AM, Jones IE, Williams SM (2004) Children who avoid drinking cow’s milk are at increased risk for prepubertal bone fractures. J Am Diet Assoc 104:250–253
Mackey DC, Lui LY, Cawthon PM, Bauer DC, Nevitt MC, Cauley JA, Hillier TA, Lewis CE, Barrett-Connor E, Cummings SR (2007) High-trauma fractures and low bone mineral density in older women and men. JAMA 298:2381–2388
Acknowledgments
We would like to thank the subjects and their families who generously donated their time to participate in this study. We also would like to thank the staff responsible for data collection Donna Bianchi, Ashwini-Roy Chaudhury, Gemma Uetrecht and Caroline Wood.
Conflicts of interest
None.
Funding
This project was supported by NIH grants AR47242 and RR08084, from the General Clinical Research Centers Program
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kalkwarf, H.J., Laor, T. & Bean, J.A. Fracture risk in children with a forearm injury is associated with volumetric bone density and cortical area (by peripheral QCT) and areal bone density (by DXA). Osteoporos Int 22, 607–616 (2011). https://doi.org/10.1007/s00198-010-1333-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-010-1333-z