
Abstract
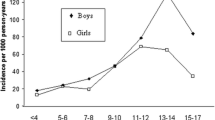
Rate of fracture was examined according to age at first fracture in 313 New Zealand children (145 girls, 168 boys) under l3 years of age (95.4% of a consecutive series of children treated at one hospital for a recent confirmed fracture at any site). In their lifetimes they had experienced 468 separate fracture events, over half (54.7%) occurring in the 32.3% of children breaking bones on more than one occasion. Children experiencing a first fracture before 4 years of age had 36.7 (95%CI 30.7–44.1) fractures per l00 years of exposure: this was a significantly higher rate than that of children experiencing their first fracture later in life. Thus, using the <4.0 year age group as a reference, we found that rate ratios (adjusted for gender) for groups that had suffered the first fracture at later ages were: first fracture between 4.0 and 6.99 years, 0.77 (95%CI 0.58–1.03); first fracture between 7.0 and 9.99 years, 0.63 (95%CI 0.42–0.94); first fracture between 10.0 and 12.99 years, 0.48 (95% CI 0.32–0.72). Asthma was over-represented (31% seen, 25% expected), and a high proportion of the sample (32.9%) used corticosteroid medications; however, neither characteristic affected age at first fracture. In contrast, the large number (n= 42) of youngsters (13.4% of the sample) reporting adverse reactions to milk were younger at first fracture than children without reactions to milk (P<0.05). We conclude that children experiencing their first fracture at a young age have high rates of fracture and should be targeted for advice to improve their bone strength.

Similar content being viewed by others

References
Jones IE, Williams SM, Dow N, Goulding A (2002) How many children remain fracture-free during growth? A longitudinal study of children and adolescents participating in the Dunedin Multidisciplinary Health and Development Study. Osteoporos Int 13:990–995
Goulding A, Jones IE, Williams SM, Grant AM, Taylor RW, Manning PJ, Langley J (2005) First fracture is associated with increased risk of new fractures during growth. J Pediatr 146:286–288
Cadogan J, Eastell R, Jones N, Barker ME (1997) Milk intake and bone mineral acquisition in adolescent girls: randomised, controlled intervention trial. BMJ 315:1255–1260
Bonjour J-P, Chevalley T, Ammann P, Slosman D, Rizzoli R (2001) Gain in bone mineral mass in prepubertal girls 3.5 years after discontinuation of calcium supplementation: a follow-up study. Lancet 358:1208–1212
Fuchs RK, Snow CM (2002) Gains in hip bone mass from high impact training are maintained: a randomized controlled trial in children. J Pediatr 141:357–362
Kontulainen S, Kannus P, Haapasalo H, Sievanen H, Pasanen M, Heinonen A, Oja P, Vuori I (2001) Good maintenance of exercise-induced bone gain with decreased training of female tennis and squash players: a prospective 5-year follow-up study of young and old starters and controls. J Bone Miner Res 16:195–201
MacKelvie KJ, Petit MA, Khan KM, Beck TJ, McKay H (2004) Bone mass and structure are enhanced following a 2-year randomized controlled trial of exercise in prepubertal boys. Bone 34:755–764
Hagino H, Yamamoto K, Ohshiro H, Nose T (2000) Increasing incidence of distal radius fractures in Japanese children and adolescents. J Orthop Sci 5:356–360
Lyons RA, Delahunty AM, Kraus D, Heaven M, McCabe M, Allen H, Nash P (1999) Children’s fractures: a population based study. Inj Prev 5:129–132
Khosla S, Melton LJ, Dekutoski MB, Achenbach SJ, Oberg AL, Riggs BL (2003) Incidence of childhood distal forearm fractures over 30 years. A population-based study. JAMA 290:1479–1485
Sherker S, Ozanne-Smith J (2004) Are current playground safety standards adequate for preventing arm fractures? Med J Aust 180:562–565
Van Staa TP, Bishop NJ, Leufkens HGM (2004) Are inhaled corticosteroids associated with an increased risk of fracture in children? Osteoporos Int 15:785–791
Goulding A, Rockell JE, Black RE, Grant AM, Jones IE, Williams SM (2004) Children who avoid drinking cow’s milk are at increased risk for prepubertal bone fractures. J Am Diet Assoc 104:250–253
Wyshak G (2000) Teenaged girls, carbonated beverage consumption, and bone fractures. Arch Paediatr Adolesc Med 154:610–613
Ma DQ, Jones G (2004) Soft drink and milk consumption, physical activity, bone mass, and upper limb fractures in children: a population-based case-control study. Calcif Tissue Int 75:286–291
Jones G, Ponsonby A-L, Smith BJ, Carmichael A (2000) Asthma, inhaled corticosteroid use, and bone mass in prepubertal children. J Asthma 37:603–611
Ma DQ, Jones G (2002) Clinical risk factors but not bone density are associated with prevalent fractures in prepubertal children. J Paediatr Child Health 38:497–500
Van Staa TP, Cooper C, Leufkens HGM, Bishop NJ (2003) Children and the risk of fractures caused by oral corticosteroids. J Bone Miner Res 18:913–918
Landin LA (1983) Fracture patterns in children. Acta Orthop Scand Suppl 54:1–109
Asher MI, Barry D, Clayton TO, Crane J, D’Souza W, Ellwood P, Ford RPK, Mackay R, Mitchell EA, Moyes C, Pattemore P, Pearce N, Stewart AW (2001) The burden of symptoms of asthma, allergic rhinoconjunctivitis and atopic eczema in children and adolescents in six New Zealand centres: ISAAC Phase One. NZ Med J 114:114–120
Hall J, Martin I (2002) Paediatric prescribing in New Zealand. NZ Fam Physician 29:14–18
Host A, Halken S, Jacobsen HP, Christensen AE, Herskind AM, Plesner K (2002) Clinical course of cow’s milk protein allergy/intolerance and atopic diseases in childhood. Pediatr Allergy Immunol 13:23–28
Lyons RA, Sellstrom E, Delahunty AM, Loeb M, Varilo S (2000) Incidence and cause of fractures in European districts. Arch Dis Child 82:452–455
Jones G, Cooley HM (2002) Symptomatic fracture incidence in those under 50 years of age in southern Tasmania. J Paediatr Child Health 38:278–283
Brudvik C, Hove LM (2003) Childhood fractures in Bergen, Norway: identifying high-risk groups and activities. J Pediatr Orthop 23:629–634
Cooper C, Dennison EM, Leufkens HGM, Bishop N, Van Staa TP (2004) Epidemiology of childhood fractures in Britain: a study using the General Practice Research Database. J Bone Miner Res 19:1976–1981
Stanley D, Bell MJ (1989) Forearm fractures in schoolchildren. BMJ 298:1159–1160
Schlienger RG, Jick SS, Meier CR (2004) Inhaled corticosteroids and the risk of fractures in children and adolescents. Pediatrics 114:469–473
Black RE, Williams SM, Jones IE, Goulding A (2002) Children who avoid drinking cow milk have low dietary calcium intakes and poor bone health. Am J Clin Nutr 76:675–680
Goulding A (2003) Milk components and bone health. Aust J Dairy Technol 58:73–78
Rockell JEP, Williams SM, Taylor RW, Grant AM, Jones IE, Goulding A (2005) Two-year changes in bone and body composition in young children with a history of prolonged milk avoidance. Osteoporos Int 16:1016–1023
Kalkwarf HJ, Khoury JC, Lanphear BP (2003) Milk intake during childhood and adolescence, adult bone density, and osteoporotic fractures in US women. Am J Clin Nutr 77:257–265
Goulding A, Cannan R, Williams SM, Gold EJ, Taylor RW, Lewis-Barned NJ (1998) Bone mineral density in girls with forearm fractures. J Bone Miner Res 13:143–148
Goulding A, Jones IE, Taylor RW, Manning PJ, Williams SM (2001) Bone mineral density and body composition in boys with distal forearm fractures: a dual-energy X-ray absorptiometry study. J Pediatr 139:509–515
Landoll JD, Mobley SL, Ha E, Badenhop-Stevens E, Hangartner TN, Matkovic V (2004) Children with bone fragility fractures have reduced volumetric bone mineral density of the radius. J Bone Miner Res 19:F343 (abstract)
Skaggs DL, Loro ML, Pitukcheewanont P, Tolo V, Gilsanz V (2001) Increased body weight and decreased radial cross-sectional dimensions in girls with forearm fractures. J Bone Miner Res 16:1337–1342
Goulding A, Jones IE, Taylor RW, Manning PJ, Williams SM (2000) More broken bones: a 4-year double cohort study of young girls with and without distal forearm fractures. J Bone Miner Res 15:2011–2018
Davidson PL, Goulding A, Chalmers DJ (2003) Biomechanical analysis of arm fracture in obese boys. J Paediatr Child Health 39:657–664
Javaid MK, Cooper C (2002) Prenatal and childhood influences on osteoporosis. Best Pract Res Clin Endocrinol Metab 16:349–367
Jones IE, Williams SM, Goulding A (2004) Associations of birth weight and length, childhood size and smoking with bone fractures during growth: evidence from a birth cohort study. Am J Epidemiol 159:343–350
Lyons R, Delahunty A, Heaven M, McCabe M, Allen H, Nash P (2000) Incidence of childhood fractures in affluent and deprived areas: population based study. BMJ 320:149
Ma D, Jones G (2003) Television, computer, and video viewing; physical activity; and upper limb fracture risk in children: a population-based case control study. J Bone Miner Res 18:1970–1977
Ma D, Morley R, Jones G (2004) Risk-taking, coordination and upper limb fractures in children: a population based case-control study. Osteoporos Int 15:633–638
Acknowledgments
We thank all the children and parents who participated and are especially grateful to the staff of the Departments of Orthopaedics, Radiology, Pediatrics and Emergency Care for their willing co-operation in this study. We acknowledge grant support from the Bone Research Unit, University of Otago and ACC. F-J.Y. was the recipient of an Otago BMed Sci (Hons) Scholarship. This study was funded and supported by the Accident Compensation Corporation (ACC), Wellington, New Zealand. Views and/or conclusions in this article are those of the authors and may not reflect the position of ACC.
Author information
Authors and Affiliations
Corresponding author
Additional information
None of the authors has any conflicts of interest
Rights and permissions
About this article
Cite this article
Yeh, FJ., Grant, A.M., Williams, S.M. et al. Children who experience their first fracture at a young age have high rates of fracture. Osteoporos Int 17, 267–272 (2006). https://doi.org/10.1007/s00198-005-2009-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-005-2009-y