
Abstract
Aims/hypothesis
We sought to assess the role of coronary artery calcification (CAC) and its progression in predicting incident coronary artery disease (CAD) in individuals with type 1 diabetes using data from the Pittsburgh Epidemiology of Diabetes Complications (EDC) Study.
Methods
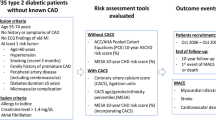
The present study examined 292 participants who had at least one CAC measure and were free from CAD at baseline; 181 (62%) had repeat CAC assessments 4–8 years later and did not develop CAD between the two CAC measures. The HRs of incident CAD events were estimated using Cox models in categorised or in appropriately transformed CAC scores. C statistics and net reclassification improvement (NRI) were used to assess the added predictive value of CAC for incident CAD.
Results
At baseline, the mean age of participants was 39.4 years and the mean diabetes duration was 29.5 years. There were 76 participants who experienced a first incident CAD event over an average follow-up of 10.7 years. At baseline, compared with those without CAC (Agatston score = 0), the adjusted HR (95% CI) in groups of 1–99, 100–399 and ≥400 was 3.1 (1.6, 6.1), 4.4 (2.0, 9.5) and 4.8 (1.9, 12.0), respectively. CAC density was inversely associated with incident CAD in those with CAC volume ≥100 (HR 0.3 [95% CI 0.1, 0.9]) after adjusting for volume score. Among participants with repeated CAC measures, annual CAC progression was positively associated with incident CAD after controlling for baseline CAC. The HR (95% CI) for above vs below the median annual CAC volume progression was 3.2 (1.2, 8.5). When compared with a model that only included established risk factors, the addition of CAC improved the predictive ability for incident CAD events in the whole group.
Conclusions/interpretation
CAC is strongly associated with incident CAD events in individuals with type 1 diabetes; its inclusion in CAD risk models may lead to improvement in prediction over established risk factors.
Similar content being viewed by others


Introduction
Individuals with diabetes have a significantly elevated risk of mortality, largely attributable to cardiovascular diseases [1,2,3]. While cardiovascular disease screening in asymptomatic individuals with diabetes does not result in improved outcomes [4], recent studies have found novel applications for certain biomarkers and imaging approaches that can further help to stratify risk in individuals with diabetes [5, 6]. Malik et al [6] demonstrated that assessment of coronary artery calcification (CAC) has value in determining the long-term prognosis of cardiovascular risk in individuals with diabetes. Though non-invasive investigations have not proved universally beneficial in clinical circumstances, the American College of Cardiology (ACC) gives a class IIa recommendation for measuring CAC under certain circumstances in cardiovascular risk assessment of individuals with diabetes [7].
Given the dynamic nature of atherosclerosis, there has been increasing interest in assessing temporal changes in CAC scores compared with single time point CAC measures. However, existing studies on the prognostic significance of CAC progression and its association with cardiovascular disease provide conflicting results, especially after taking into account single time point CAC measures [8, 9]. Although CAC is well recognised as a surrogate of overall atherosclerotic burden, the magnitude of calcification may also reflect a stabilising process in plaques. This notion is supported by Criqui et al [10] who observed that CAC density protected against cardiovascular disease events when controlling for CAC volume in the general population. In the Coronary Artery Calcification in Type 1 Diabetes (CACTI) study, a faster CAC progression in individuals with type 1 diabetes compared with non-diabetic individuals was reported [11]. Unfortunately, the prognostic significance of temporal change in CAC as well as CAC density has not been well studied in people with diabetes.
Disease onset is earlier in people with type 1 diabetes than in those with type 2 diabetes, meaning that the disease has a significantly larger impact on life expectancy and cardiovascular risk [3, 12]. Consequently, risk prediction models based on the general population or cohorts of individuals with type 2 diabetes are not suitable for predicting cardiovascular risk in type 1 diabetes [13]. The most recent validated risk engine, QRISK3, accounts for type 1 diabetes status [14]. A number of cardiovascular risk prediction models focused on individuals with type 1 diabetes have not shown good calibration and discrimination [12, 15, 16]. These models did not adequately capture the heterogeneity in cardiovascular risk in individual individuals with type 1 diabetes as they invariably failed to capture the impact of certain risk factors [17, 18]. CAC measures therefore may be useful in assessing and managing cardiovascular risk in individuals with type 1 diabetes, although there are limited outcome data demonstrating their utility in risk prediction in type 1 diabetes over and above existing risk models [18]. We thus sought to assess the role of CAC measures and CAC progression in predicting coronary artery disease (CAD) outcomes using data from a prospective cohort of individuals with childhood-onset type 1 diabetes participating in the Pittsburgh Epidemiology of Diabetes Complications (EDC) study based in Western Pennsylvania.
Methods
Study population
As described previously [19], the EDC study was a prospective cohort of individuals with childhood-onset type 1 diabetes. Participants were diagnosed before the age of 17 years and seen within 1 year of the diagnosis at the Children’s Hospital of Pittsburgh between 1950 and 1980. Though clinic based, this cohort has been shown to be epidemiologically representative of the type 1 diabetes population in Allegheny County, Pennsylvania [20]. A total of 658 eligible participants were examined between 1986 and 1988 and then assessed biennially over a 25 year period.
At the EDC 10 year follow-up examination (1996–1998), all participants aged 30 years or over were initially invited to undergo a CAC scan; this invitation was subsequently expanded to participants aged ≥18 years after approval was obtained from the University of Pittsburgh Institutional Review Board. A subset of participants also agreed to have repeat scans approximately 4–8 years later, at the EDC 14 year (2000–2002) or 18 year (2004–2006) follow-up examination. Informed consent was obtained from all participants.
A total of 292 participants who had at least one CAC assessment and were free from CAD at the time of the assessment was evaluated in the current report. Of these, 199 (68%) had repeated scans; 181 individuals did not develop CAD between CAC measures and were included for the evaluation of CAC progression. Compared with individuals who had a second CAC measure, participants who had no repeat CAC scan were older, more likely to use statins and had earlier onset of diabetes, longer diabetes duration, higher BMI, higher systolic blood pressure and higher baseline CAC scores (see electronic supplementary material [ESM] Table 1). The time of first CAC measurement was taken as the baseline for these analyses. Participants were followed up to first event, death or the 25th year of the EDC study (2011–2014).
Assessment of coronary artery calcification
All the CAC scans were evaluated centrally at one site. CAC was measured using electron beam computed tomography (EBCT) scans (Imatron C-150 scanner; GE, South San Francisco, CA, USA). Scans were triggered by electrocardiogram signals at 80% of the R–R interval and obtained in 3 mm contiguous sections of the heart. CAC was quantified using Agatston units (following the method described by Agatston et al [21]) and by a volume-based approach using the isotropic interpolation method [22]. The area and density scores were obtained using the algorithms described in the Multi-Ethnic Study of Atherosclerosis (MESA) [10]. The area score was obtained by dividing the volume score by the scan slice thickness of 3.0 mm. The density score was subsequently calculated by dividing the Agatston score by area score (CAC density = Agatston score / area score). The progression was determined as the annualised difference between the square root of baseline and square root of follow-up CAC score (annual CAC progression = √[follow-up CAC] − √[baseline CAC] / [t2 − t1 in years]), according to the method previously published by Radford et al [9] (t1 and t2 refer to the time at baseline and the follow-up, respectively). CAC volume might be a better measure of progression, as the Agatston score is determined using both CAC density and volume [23]. Our primary analysis of CAC progression was thus based on CAC volume. We also examined progression in CAC Agatston score associated with incident CAD.
Ascertainment of CAD
CAD status was evaluated biennially from the first CAC measure to the end of the follow-up. Incident CAD was defined as new-onset EDC physician-diagnosed angina, myocardial infarction confirmed by Q waves on an ECG (Minnesota codes 1.1 or 1.2) or hospital records, angiographic stenosis ≥50%, revascularisation or ischaemic ECG changes (Minnesota codes 1.3, 4.1–4.3, 5.1–5.3 and 7.1) [24]. Other than fatal and non-fatal myocardial infarction, all CAD events in the present analysis occurred at least 90 days after the CAC tests, suggesting that the CAD diagnoses were unlikely to have been driven by the CAC results.
Measurement of covariates
Demographic and medical history information was obtained through questionnaires at the time of first CAC measure. An ‘ever smoker’ was defined as a person who had smoked at least 100 cigarettes in their lifetime. BMI was calculated as the weight (kg) divided by the square of the height (m2). Blood pressure was measured three times using a random zero sphygmomanometer according to the Hypertension Detection and Follow-up Program protocol and the mean of second and third readings was used [25]. Hypertension was defined as systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg or the use of antihypertensive medications [26].
HbA1c was assessed via automated HPLC (Diamat; BioRad, Hercules, CA, USA) at the time CAC was first assessed. Subsequently, HbA1c was measured with the DCA 2000 analyser (Bayer, Tarrytown, NY, USA). Results from the two methods were highly correlated (r = 0.95) [27]. The values were then converted to DCCT-aligned HbA1c using a regression equation derived from duplicate assays [27]. Total cholesterol was determined enzymatically [28]. HDL-cholesterol was measured by a precipitation technique (heparin and manganese chloride) using a modified version of the Lipid Research Clinics method [29]. Non-HDL-cholesterol was calculated as total cholesterol minus HDL-cholesterol. Urinary albumin was determined by immunonephelometry [30]. Urinary albumin excretion rate (AER) was calculated for each of three timed urinary samples (24 h, overnight and 4 h collections); the median of the three AERs was used in the analyses.
Statistical analysis
Demographics and risk factors were compared among those with baseline CAC = 0, 1–99 and ≥100 and between CAD incident cases and non-cases at the end of follow-up. For comparing three subgroups with different CAC values, the χ2 test for categorical variables and unbalanced analysis of variance (ANOVA) analysis for continuous variables were used, as appropriate. Unadjusted Cox proportional hazard models were applied to report p values for the comparisons between CAD cases and non-cases.
Cox proportional hazard models were constructed with follow-up years used as the time axis to assess the association of baseline CAC Agatston and volume score with the incidence of CAD. Baseline CAC was examined in three ways: four categories (0, 1–99, 100–399 and ≥400), two categories (<100 and ≥100), log-transformed continuous variables (loge [CAC+1]). The loge (CAC+1) transformation has been previously used in the MESA papers for studies both in the general population [31] and in the population with diabetes [6]. HRs and 95% CIs were presented accordingly. For multivariable analyses, the models were adjusted for risk factors that had been previously demonstrated to be important predictors of CAD [12] or that were found to be significantly associated with outcomes in the univariate analyses. Of note, age and diabetes duration were highly correlated (r = 0.84) in this childhood-onset type 1 diabetes cohort. Thus, only diabetes duration was used for the adjustment. Specifically, model 1 adjusted for sex, diabetes duration, ever smoking, BMI, HbA1c and hypertension, and model 2 (fully adjusted model) further controlled for urinary AER, lipid profile (HDL- and non-HDL-cholesterol) and the use of statins.
Only participants with CAC >0 were analysed for CAC density because plaque density could only be quantified in those with prevalent CAC [10]. Cox proportional hazard models were performed to evaluate the association between CAC density and incident CAD after adjusting for CAC volume and the full set of covariates as described above. The adjusted model was then stratified by CAC volume (1–99 vs ≥100). Heterogeneity of effect in the association between density and clinical outcomes by CAC volume was tested by fitting interaction terms between density and categorical CAC volume (1–99 vs ≥100) in the adjusted model. A CAC score of ≥100 was chosen as it is considered to confer a moderate (or more) cardiovascular risk among asymptomatic individuals [32].
The association of CAC progression with incident CAD, adjusting for baseline CAC and the full set of the covariates, was assessed in those with repeated CAC measures also using Cox models. The primary analysis of annual CAC progression was based on a dichotomised variable (below vs above the median) in volume score.
The proportionality assumptions were confirmed using Schoenfeld residuals as well as interaction terms with follow-up time [33].
The incremental values of the CAC measures for prediction of CAD events were evaluated by the increase in the C-statistic [34] and improvement in the continuous net reclassification improvement (NRI) [35] as compared with the basic model only with established risk factors. The fit of the models was assessed using the log-likelihood ratio test.
Urinary AER was log-transformed prior to statistical testing, given the highly skewed distribution of this variable. A two-sided p < 0.05 was considered significant. All analyses were performed with SAS v 9.4 (SAS Institute, Cary, NC, USA) and R version 3.4.3 (R Core Team, Vienna, Austria). The R package ‘survIDINRI’ was applied for NRI analysis with censored survival data and the package ‘survC1’ for C statistics for risk prediction.
Results
Among the 292 participants that were free from clinical CAD at the first CAC measure (baseline of this analysis), the mean age was 39.4 (range 18–60) years and mean diabetes duration was 29.5 (range 17–55) years. A total of 76 participants experienced a first incident CAD event during a mean (SD) follow-up of 10.7 (5.0) years from the first CAC measure. These events were grouped into five categories: fatal myocardial infarction (13, 17.1%), non-fatal myocardial infarction (15, 19.7%), revascularisation (25, 32.9%), physician-diagnosed angina (14, 18.4%) and ECG-confirmed ischaemia (9, 11.8%).
The demographic and clinical characteristics of study participants are presented in Table 1. Individuals who had any amount of CAC detected at baseline were more likely to smoke and had longer diabetes duration and higher urinary AER than those without CAC. Compared with individuals who did not develop CAD during the follow-up, those who had incident CAD were more likely to be older, have longer diabetes duration and have higher systolic blood pressure and urinary AER. Additionally, individuals who had incident CAD on follow-up had a remarkably heavier burden of CAC at baseline.
At baseline, compared with individuals without CAC (i.e. score = 0), the adjusted HR (95% CI) associated with incident CAD events for individuals with an Agatston score of 1–99, 100–399 and ≥400 was 3.1 (1.6, 6.1), 4.4 (2.0, 9.5) and 4.8 (1.9, 12.0), respectively (Table 2). Categorised CAC volume (0, 1–99, 100–399 and ≥400) showed a similar ‘dose-dependent’ response for incident CAD risk prediction even after adjusting for a wide range of risk factors. The CAD risk in participants with CAC over 100 was twice that of those with CAC less than 100 (Table 2). These CAC associations remained significant when only fatal and non-fatal incident myocardial infarction was included as an outcome event (28 events were identified). Compared with CAC = 0, the adjusted HR (95% CI) of Agatston score group 1–99, 100–399 and ≥400 was 3.2 (1.01, 10.2), 3.9 (0.99, 15.4) and 5.6 (1.3, 23.4), respectively.
Table 3 shows the associations of CAC density with incident CAD and the interaction effect of CAC volume and density in participants with baseline CAC >0. Controlling for CAC volume and established risk factors (sex, diabetes duration, ever smoking, BMI, HbA1c, hypertension, HDL- and non-HDL-cholesterol, urinary AER and the use of statins), density was inversely associated with CAD, although the association was statistically non-significant (HR [95% CI] 0.8 [0.5, 1.2], p = 0.269). In the stratified analysis, however, CAC density was significantly inversely associated with incident CAD in the subgroup with CAC volume score ≥100 (HR [95% CI] 0.3 [0.1, 0.9], p = 0.027). The inverse association was attenuated and became non-significant in those with lower CAC volume (1–99) (HR [95% CI] 0.7 [0.3, 1.7], p = 0.419). In the overall adjusted model, the interaction term of CAC volume and density was marginal (p = 0.06).
In participants with repeated CAC measures, CAC annual progression showed a positive association with incident CAD after controlling for baseline CAC and other covariates (Table 4). When compared with participants with an annual rate of volume progression below the median (0.24), the adjusted HR (95% CI) in those with a rate of progression above the median was 3.2 (1.2, 8.5) (p = 0.020). A similar association was observed for annual progression of CAC Agatston scores. The results of CAC annual progression and incident CAD were consistent when including participants who developed CAD between the two CAC scans (ESM Table 2).
When compared with the model that only included established risk factors (i.e. base model, comprised of sex, diabetes duration, smoking status, BMI, HbA1c, HDL- and non-HDL-cholesterol, urine AER, hypertension and the use of statins), the addition of baseline CAC measures significantly improved the fit of the model (ESM Table 3) and the discrimination ability for incident CAD event, as determined by C-statistic (ESM Table 4) and continuous NRI (ESM Table 5) in the study participants overall (N = 292). In the subgroup of participants who had repeated CAC measures and did not develop CAD between two CAC scans (n = 181), the inclusion of measures of either baseline CAC or CAC progression led to an improvement in CAD risk prediction over the baseline model, although the difference was not statistically significant.
Discussion
Using data from a long-term prospective cohort study of individuals with early onset type 1 diabetes we demonstrated that Agatston and volume-based CAC measures are moderately and independently associated with the risk of incident CAD in this population. We also found that CAC density is inversely associated with CAD risk in individuals with moderately to markedly elevated CAC volume (CAC volume ≥100). The inclusion of CAC in CAD risk models led to improvement in prediction over established risk factors in the study participants overall. In a subgroup of participants who had repeated CAC measures, information on either baseline CAC or CAC progression improved risk prediction but the difference was not statistically significant.
Individuals with diabetes have, in the past, been lumped together into a ‘coronary risk equivalent’ category, based on early works by Haffner and colleagues [36, 37]. However, a number of more recent studies have challenged this concept based on findings of significantly lower risk of cardiovascular disease in people with diabetes compared with those with prior history of myocardial infarction [38], and presence of significant heterogeneity in risk based on age and diabetes duration [39, 40]. This is particularly important in individuals with type 1 diabetes in whom early onset and long duration of disease confers a broad range of risk. The use of type 1 diabetes risk scores and novel application of biomarkers (e.g. N-terminal pro-brain natriuretic peptide [NT-pro-BNP]) and imaging techniques (e.g. CAC score) can help identify those at low or high risk of CAD. The current findings complement and supplement extant data on the use of CAC in CAD risk prediction in diabetes. While Malik et al demonstrated the usefulness of CAC measures in type 2 diabetes [41], our study extends those findings to individuals with type 1 diabetes. We demonstrated a strong independent association between CAC and CAD in type 1 diabetes and the incorporation of CAC measures in risk prediction models materially improved discrimination of people at high risk of CAD above and beyond established risk factors. Moreover, as Malik et al observed, we found that individuals with zero CAC had a much lower risk of CAD over a 10 year period [41]. Such ability to identify individuals with type 1 diabetes that are at high or low risk of incident CAD will allow targeting of preventive strategies and enable personalised care of individuals. While the materially higher risk of incident CAD among our participants (10 year risk 11–52%) represents the higher risk category of this group, it may also in part reflect the broader definition of CAD used in this study (which included angina and coronary stenosis >50%, rather than hard events only).
Our finding of an inverse association between CAC density and CAD risk among individuals with CAC volume ≥100 is in keeping with a prior report by Criqui et al, based on the general MESA cohort, that showed a similar inverse relationship [10]. However, we did not find a significant association in individuals with CAC volume <100, unlike the MESA study in which no significant interaction of CAC density with volume was noted [42]. Increasing CAC density is hypothesised to protect against CAD events because a calcified plaque is likely to be more stable than a soft plaque [10]. Consistent with this hypothesis, Hou et al have reported a higher incidence of cardiovascular events in individuals with non-calcified plaque [43]. The current study provides findings in individuals with type 1 diabetes compatible with this hypothesis. The lack of significant association in individuals with CAC volume <100 may represent a true difference in type 1 diabetes, suggesting that having a dense plaque is beneficial only in individuals with significant atherosclerotic burden in this population, or this may represent a type 2 error, given the relatively smaller sample size.
We also found that CAC progression was independently and strongly associated with incident CAD. Although addition of information on CAC progression improves risk prediction to some extent, the difference was not statistically significant when assessed by C-statistic and NRI. This finding is consistent with a report by Radford et al showing that a single measurement of CAC provides similar predictive ability to information on CAC progression [9]. The authors concluded that when serial measurements of CAC are available, information on the latest CAC would be sufficient to capture the risk. However, it is important to note that the small sample size (n = 181) and event numbers (n events = 37) of the subgroup in our study limit the power of the statistical tests. In addition, selection bias is a major concern: when participants who developed CAD between the two CAC measures (18 cases) were excluded from the analysis, participants who developed CAD earlier (between the two CAC scans) vs later (after the second CAC scan) were likely to carry a much higher degree of CAD risk.
The 18 individuals who developed CAD between the first and second set of scans (in the 55 individuals with CAD who had repeated CAC scans) were excluded from the primary analysis since it was uncertain whether these events, which might lead to a change in therapy, could influence the progression of CAC. However, given the pathogenesis of CAC, as well as the chronic and cumulative features of calcification in vessels [44], we believe it is unlikely that the degree of CAC progression would be much influenced by the diagnosis of CAD. Indeed, Schenker et al reported a stepwise association between CAC scores and death or myocardial infarction among those with existing myocardial ischaemia [45]. As such, the average annual rate of CAC progression between two scans is likely to be representative of the progression rate between the first scan and the occurrence of the event. Nevertheless, the Cox model results regarding the positive and significant association between annual CAC progression rate and incident CAD were consistent whether or not data from these 18 participants were retained in the analysis.
The strengths and limitations of the present study merit some consideration. First, to our knowledge, this is the first study to demonstrate the utility of CAD risk prediction using CAC scores in individuals with childhood-onset type 1 diabetes. Second, with repeat data from a subset of participants we demonstrated the potential role of CAC progression in this population. Third, we observed the protective effect of CAC density in participants with high CAC volume. Finally, as the EDC is a cohort with long-term follow-up of individuals with a very young age of type 1 diabetes onset, this report helps to better understand the trajectory and heterogeneity of the disease with regards to CAD events.
Despite its long follow-up period, the power of this study may be limited by the small number of participants (fewer than 300). Similarly, information on CAC progression was available for a smaller subset, limiting the statistical power and our ability to reject the null hypotheses. Nonetheless, given the large number of events observed, we were able to detect differences for several of the hypotheses that were tested. Second, we did not have the ability to look at specific CAD outcomes, such as myocardial infarction, CAD mortality and revascularisation, or softer outcomes such as angina or coronary stenosis >50%. However, we have used a rigorous assessment of CAD events and have previously demonstrated that this is a valid outcome for evaluation of risk prediction models [12].
In conclusion, we found that CAC score is strongly associated with the risk of incident CAD in individuals with type 1 diabetes. Inclusion of CAC measures in CAD risk models may lead to improvement in prediction over established risk factors. Further research assessing the utility of CAC measurements in type 1 diabetes in better targeting interventions and improving CAD events and mortality outcomes is warranted.
Abbreviations
- AER:
-
Albumin excretion rate
- CAC:
-
Coronary artery calcification
- CAD:
-
Coronary artery disease
- EDC:
-
Epidemiology of Diabetes Complications study
- MESA:
-
Multi-Ethnic Study of Atherosclerosis
- NRI:
-
Net reclassification improvement
References
Harris MI (1995) Summary. In: Harris MI, Cowie CC, Stern MP, Boyko EJ, Reiber GE, Bennett PH (eds), Diabetes in America, 2nd ed. U.S. Govt. Printing Office, Washington, DC (National Institute of Health [NIH] publication No.95–1468)
Khunti K, Davies M, Majeed A et al (2015) Hypoglycemia and risk of cardiovascular disease and all-cause mortality in insulin-treated people with type 1 and type 2 diabetes: a cohort study. Diabetes Care 38(2):316–322. https://doi.org/10.2337/dc14-0920
Secrest AM, Becker DJ, Kelsey SF et al (2010) Cause-specific mortality trends in a large population-based cohort with long-standing childhood-onset type 1 diabetes. Diabetes 59(12):3216–3222. https://doi.org/10.2337/db10-0862
Young LH, Wackers FJT, Chyun DA et al (2009) Cardiac outcomes after screening for asymptomatic coronary artery disease in patients with type 2 diabetes: the DIAD study: a randomized controlled trial. JAMA 301(15):1547–1555. https://doi.org/10.1001/jama.2009.476
Silverman MG, Blaha MJ, Budoff MJ et al (2012) Potential implications of coronary artery calcium testing for guiding aspirin use among asymptomatic individuals with diabetes. Diabetes Care 35(3):624–626. https://doi.org/10.2337/dc11-1773
Malik S, Zhao Y, Budoff M et al (2017) Coronary artery calcium score for long-term risk classification in individuals with type 2 diabetes and metabolic syndrome from the Multi-Ethnic Study of Atherosclerosis. JAMA Cardiol 2(12):1332–1340. https://doi.org/10.1001/jamacardio.2017.4191
Budoff MJ, Raggi P, Beller GA et al (2016) Noninvasive cardiovascular risk assessment of the asymptomatic diabetic patient: the imaging Council of the American College of cardiology. JACC Cardiovasc Imaging 9:176–192
McEvoy JW, Blaha MJ, DeFilippis AP et al (2010) Coronary artery calcium progression: an important clinical measurement? J Am Coll Cardiol 56(20):1613–1622. https://doi.org/10.1016/j.jacc.2010.06.038
Radford NB, DeFina LF, Barlow CE et al (2016) Progression of CAC score and risk of incident CVD. JACC Cardiovasc Imaging 9:1420–1429
Criqui MH, Denenberg JO, Ix JH et al (2014) Calcium density of coronary artery plaque and risk of incident cardiovascular events. JAMA 311(3):271. https://doi.org/10.1001/jama.2013.282535
Maahs DM, Jalal D, Chonchol M et al (2013) Impaired renal function further increases odds of 6-year coronary artery calcification progression in adults with type 1 diabetes: the CACTI study. Diabetes Care 36(9):2607–2614. https://doi.org/10.2337/dc12-2538
Zgibor JC, Ruppert K, Orchard TJ et al (2010) Development of a coronary heart disease risk prediction model for type 1 diabetes: The Pittsburgh CHD in Type 1 Diabetes Risk Model. Diabetes Res Clin Pract 88(3):314–321. https://doi.org/10.1016/j.diabres.2010.02.009
Zgibor JC, Piatt GA, Ruppert K et al (2006) Deficiencies of cardiovascular risk prediction models for type 1 diabetes. Diabetes Care 29(8):1860–1865. https://doi.org/10.2337/dc06-0290
Hippisley-Cox J, Coupland C, Brindle P (2017) Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: prospective cohort study. BMJ 357:j2099
Cederholm J, Eeg-Olofsson K, Eliasson B et al (2011) A new model for 5-year risk of cardiovascular disease in type1 diabetes; from the Swedish National Diabetes Register (NDR). Diabet Med 28(10):1213–1220. https://doi.org/10.1111/j.1464-5491.2011.03342.x
Vistisen D, Andersen GS, Hansen CS et al (2016) Prediction of first cardiovascular disease event in type 1 diabetes mellitus the steno type 1 risk engine. Circulation 133(11):1058–1066. https://doi.org/10.1161/CIRCULATIONAHA.115.018844
Wurm R (2016) Cardiovascular risk prediction in patients with diabetes – when one biomarker is not enough. Available from http://www.acc.org/latest-in-cardiology/articles/2016/11/03/08/32/cardiovascular-risk-prediction-in-patients-with-diabetes. Accessed 13 Mar 2018
Burge MR, Eaton RP, Schade DS (2016) The role of a coronary artery calcium scan in type 1 diabetes. Diabetes Technol Ther 18(9):594–603. https://doi.org/10.1089/dia.2016.0110
Orchard TJ, Dorman JS, Maser RE et al (1990) Prevalence of complications in IDDM by sex and duration. Pittsburgh Epidemiology of Diabetes Complications Study II. Diabetes 39(9):1116–1124. https://doi.org/10.2337/diab.39.9.1116
Wagener DK, Sacks JM, LaPorte RE, Macgregor JM (1982) The Pittsburgh study of insulin-dependent diabetes mellitus. Risk for diabetes among relatives of IDDM. Diabetes 31(2):136–144. https://doi.org/10.2337/diab.31.2.136
Agatston AS, Janowitz WR, Hildner FJ et al (1990) Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 15(4):827–832. https://doi.org/10.1016/0735-1097(90)90282-T
Callister TQ, Cooil B, Raya SP et al (1998) Coronary artery disease: improved reproducibility of calcium scoring with an electron-beam CT volumetric method. Radiology 208(3):807–814. https://doi.org/10.1148/radiology.208.3.9722864
Hokanson JE, MacKenzie T, Kinney G et al (2004) Evaluating changes in coronary artery calcium: an analytic method that accounts for interscan variability. Am J Roentgenol 182(5):1327–1332. https://doi.org/10.2214/ajr.182.5.1821327
Orchard TJ, Olson JC, Erbey JR et al (2003) Insulin resistance-related factors, but not glycemia, predict coronary artery disease in type 1 diabetes: 10-year follow-up data from the Pittsburgh Epidemiology of Diabetes Complications Study. Diabetes Care 26(5):1374–1379. https://doi.org/10.2337/diacare.26.5.1374
Borhani N, Kass E, Langford H et al (1976) The hypertension detection and follow-up program: Hypertension detection and follow-up program cooperative group. Prev Med (Baltim) 5:207–215
Costacou T, Orchard TJ (2013) Differential effect of glycemia on the incidence of hypertension by sex: The Epidemiology of Diabetes Complications study. Diabetes Care 36(1):77–83. https://doi.org/10.2337/dc12-0708
Prince CT, Becker DJ, Costacou T et al (2007) Changes in glycaemic control and risk of coronary artery disease in type 1 diabetes mellitus: findings from the Pittsburgh Epidemiology of Diabetes Complications Study (EDC). Diabetologia 50(11):2280–2288. https://doi.org/10.1007/s00125-007-0797-7
Allain CC, Poon LS, Chan CS et al (1974) Enzymatic determination of total serum cholesterol. Clin Chem 20:470–475
Warnick GR, Albers JJ (1978) Heparin--Mn2+ quantitation of high-density-lipoprotein cholesterol: an ultrafiltration procedure for lipemic samples. Clin Chem 24:900–904
Ellis D, Coonrod BA, Dorman JS et al (1989) Choice of urine sample predictive of microalbuminuria in patients with insulin-dependent diabetes mellitus. Am J Kidney Dis 13(4):321–328. https://doi.org/10.1016/S0272-6386(89)80039-3
McClelland RL, Nasir K, Budoff M et al (2009) Arterial age as a function of coronary artery calcium (from the Multi-Ethnic Study of Atherosclerosis [MESA]). Am J Cardiol 103(1):59–63. https://doi.org/10.1016/j.amjcard.2008.08.031
Greenland P, LaBree L, Azen SP et al (2004) Coronary artery calcium score combined with framingham score for risk prediction in asymptomatic individuals. JAMA 291(2):210. https://doi.org/10.1001/jama.291.2.210
Schoenfeld D (1982) Partial residuals for the proportional hazards regression model. Biometrika 69(1):239–241. https://doi.org/10.1093/biomet/69.1.239
Uno H, Cai T, Pencina MJ et al (2011) On the C-statistics for evaluating overall adequacy of risk prediction procedures with censored survival data. Stat Med 30:1105–1117
Pencina MJ, D’Agostino RB, Steyerberg EW (2011) Extensions of net reclassification improvement calculations to measure usefulness of new biomarkers. Stat Med 30(1):11–21. https://doi.org/10.1002/sim.4085
Haffner SM, Lehto S, Rönnemaa T et al (1998) Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 339(4):229–234. https://doi.org/10.1056/NEJM199807233390404
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (2001) Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA 285(19):2486–2497. https://doi.org/10.1001/jama.285.19.2486
Bulugahapitiya U, Siyambalapitiya S, Sithole J, Idris I (2009) Is diabetes a coronary risk equivalent? Systematic review and meta-analysis. Diabet Med 26(2):142–148. https://doi.org/10.1111/j.1464-5491.2008.02640.x
Rana JS (2016) Is diabetes really a CHD risk equivalent? Available from http://www.acc.org/latest-in-cardiology/articles/2016/04/12/13/40/is-diabetes-really-a-chd-risk-equivalent. Accessed 13 Mar 2018
Wannamethee SG, Shaper AG, Whincup PH et al (2011) Impact of diabetes on cardiovascular disease risk and all-cause mortality in older men: influence of age at onset, diabetes duration, and established and novel risk factors. Arch Intern Med 171(5):404–410. https://doi.org/10.1001/archinternmed.2011.2
Malik S, Budoff MJ, Katz R et al (2011) Impact of subclinical atherosclerosis on cardiovascular disease events in individuals with metabolic syndrome and diabetes: the multi-ethnic study of atherosclerosis. Diabetes Care 34(10):2285–2290. https://doi.org/10.2337/dc11-0816
Criqui MH, Knox JB, Denenberg JO et al (2017) Coronary artery calcium volume and density: potential interactions and overall predictive value: The Multi-Ethnic Study of Atherosclerosis. JACC Cardiovasc Imaging 10:845–854
Hou Z, Lu B, Gao Y et al (2012) Prognostic value of coronary CT Angiography and calcium score for major adverse cardiac events in outpatients. JACC Cardiovasc Imaging 5:990–999
Min JK, Lin FY, Gidseg DS et al (2010) Determinants of coronary calcium conversion among patients with a normal coronary calcium scan. J Am Coll Cardiol 55(11):1110–1117. https://doi.org/10.1016/j.jacc.2009.08.088
Schenker MP, Dorbala S, Hong ECT et al (2008) Interrelation of coronary calcification, myocardial ischemia, and outcomes in patients with intermediate likelihood of coronary artery disease: a combined positron emission tomography/computed tomography study. Circulation 117(13):1693–1700. https://doi.org/10.1161/CIRCULATIONAHA.107.717512
Acknowledgements
The authors thank the staff and the participants of the EDC study for their contributions.
Data availability
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Funding
Research reported in this study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases at the National Institutes of Health (grant R01-DK-034818) and the Rossi Memorial Fund.
Author information
Authors and Affiliations
Contributions
JG conceived and designed the study, acquired, analysed and interpreted the data and drafted the manuscript. SAE conceived and designed the study, interpreted the data, drafted the manuscript and edited and critically reviewed the manuscript for important intellectual content. RGM and DE conceived and designed the study, acquired and interpreted the data and edited and critically reviewed the manuscript for important intellectual content. TJO and TC conceived and designed the study, acquired and interpreted the data, edited and critically reviewed the manuscript for important intellectual content and provided administrative and material support. All authors gave final approval of the version of the manuscript to be published. TJO is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding author
Ethics declarations
The authors declare that there is no duality of interest associated with this manuscript.
Electronic supplementary material
ESM
(PDF 200 kb)
Rights and permissions
About this article

Cite this article
Guo, J., Erqou, S.A., Miller, R.G. et al. The role of coronary artery calcification testing in incident coronary artery disease risk prediction in type 1 diabetes. Diabetologia 62, 259–268 (2019). https://doi.org/10.1007/s00125-018-4764-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-018-4764-2