
Purpose:
To evaluate the outcome of hyperfractionated-accelerated radiotherapy and subsequent planned primary tumor resection and radical neck dissection in locally advanced tumors of the oral cavity.
Patients and Methods:
This retrospective analysis evaluates 126 subsequent patients who were treated between 1988 and 1997 for locally advanced tumors of the oral cavity (with extension into the oropharynx in 17 patients), 34 (27%) AJCC stage III and 92 (73%) stage IV. Primary tumor and nodal metastases were irradiated with 1.4 Gy bid to a median total dose of 72.8 Gy (range 58.8–75.6 Gy). Then, planned radical surgery of the primary site according to the initial tumor extent and cervical nodes was performed. Median follow-up of living patients was 6 years (range 1–11 years).
Results:
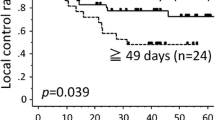
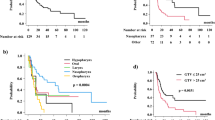
4 weeks after radiotherapy, 14 patients (11%) had complete tumor remission, 92 (73%) partial remission, 15 (12%) no change, and five (4%) progressive disease. Complete resection was achieved in 117 (93%) patients (nine incomplete resections). 5-year locoregional control rate was 62 ± 9%, overall survival 36 ± 9%. Surgery-related morbidity occurred in 42 patients (33%; mainly delayed wound healing and fistulae), overall severe treatment-related morbidity in 46 patients (36%). 24/84 relapse-free patients (29%) required a percutaneous gastrostomy or nasal tube ≥ 1 year after therapy.
Conclusion:
In this study, the outcome of combined curative radiotherapy and planned surgery of the primary tumor and neck nodes was comparable to reported results of hyperfractionated radiotherapy with or without salvage surgery of the neck nodes with respect to locoregional control and overall survival. Planned surgery carries a substantial risk of morbidity and seems to offer no benefit in comparison to salvage surgery of the neck nodes only. Therefore, salvage surgery is preferred.
Ziel:
Das Ergebnis einer hyperfraktioniert-akzelerierten Strahlentherapie, gefolgt von geplanter Resektion des Primärtumors und einer zervikalen Lymphknotendissektion bei fortgeschrittenen Mundhöhlentumoren wurde untersucht.
Patienten und Methodik:
Retrospektiv wurde das Therapieergebnis von 126 Patienten analysiert, die von 1988 bis 1997 wegen lokal fortgeschrittener, potentiell operabler Mundhöhlentumoren (mit Ausdehnung bis in den Oropharynx bei 17 Patienten)—34 Tumoren (27%) im AJCC-Stadium III und 92 (73%) im Stadium IV—behandelt wurden. Primärtumor und Lymphknotenmetastasen wurden mit 1,4 Gy zweimal täglich, Wochendosis 12,6 Gy, Gesamtdosis 72,8 Gy (Spanne 58,8–75,6 Gy), bestrahlt. Anschließend wurden eine radikale Tumor- und Lymphknotenresektion durchgeführt. Die mediane Nachbeobachtungszeit lebender Patienten beträgt 6 Jahre (Spanne 1–11 Jahre).
Ergebnisse:
4 Wochen nach Strahlentherapie hatten 14 Patienten (11%) eine komplette Tumorremission, 92 (73%) eine partielle Tumorremission, 15 (12%) Status idem und fünf (4%) einen progredienten Tumor. Eine komplette Tumorresektion war bei 117/126 Patienten (93%) möglich. Die lokale 5-Jahres-Kontrollrate betrug 62 ± 9%, das Gesamtüberleben 36 ± 9%. Operationsassoziierte Morbidität, vor allem verzögerte Wundheilung und Fisteln, trat bei 42 Patienten (33%) auf. Insgesamt wurden gravierende Therapiefolgen bei 46 Patienten (36%) beobachtet. 24/84 rezidivfreie Patienten (29%) hatten ≥ 1 Jahr nach Therapie eine PEG (perkutane endoskopische Gastrostomie).
Schlussfolgerung:
In diesem Patientenkollektiv waren die lokale Kontrollrate und die Gesamtüberlebenszeit mit den publizierten Ergebnissen von hyperfraktioniert-akzelerierten Studien mit und ohne „salvage surgery“ der Lymphknoten vergleichbar. Die elektive Resektion des Primärtumors und der zervikalen Lymphknoten („in den alten Grenzen“) wies ein deutliches Morbiditätsrisiko auf. Ihr Nutzen im Vergleich zu ausschließlicher hyperfraktioniert-akzelerierter Strahlentherapie ist wahrscheinlich gering, so dass die Resektion auf inkomplett zurückgebildete Lymphknotenmetastasen beschränkt werden sollte.
Similar content being viewed by others

Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hoeller, U., Biertz, I., Flinzberg, S. et al. Hyperfractionated-Accelerated Radiotherapy Followed by Radical Surgery in Locally Advanced Tumors of the Oral Cavity. Strahlenther Onkol 182, 157–163 (2006). https://doi.org/10.1007/s00066-006-1472-5
Received:
Revised:
Issue Date:
DOI: https://doi.org/10.1007/s00066-006-1472-5