
Abstract
Purpose
We investigated whether the preemptive use of gabapentin, a structural analogue of gamma amino butyric acid could reduce postoperative pain and fentanyl consumption in patients after single-level lumbar discoidectomy.
Methods
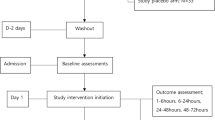
Fifty-six ASA I and II patients were randomly allocated into two equal groups to receive either gabapentin 300 mg or placebo two hours before surgery. After surgery, the pain was assessed on a visual analogue scale (VAS) at intervals of 0–6, 6–12, 12–18, and 18–24 hr at rest. Total fentanyl consumption in the first 24 hr after surgery was also recorded. Fentanyl 2 μg·kg−1 intravenously was used to treat postoperative pain on patients’ demand.
Results
Patients in the gabapentin group had significantly lower VAS scores at all time intervals of 0–6, 6–12, 12–18,and 18–24 hr than those in the placebo group (3.5 ± 2.3, 3.2 ± 2.1, 1.8 ± 1.7, 1.2 ± 1.3 vs 6.1 ± 1.7, 4.4 ± 1.2, 3.3 ± 1.1, 2.1 ± 1.2; P < 0.05). The total fentanyl consumed after surgery in the first 24 hr in the gabapentin group (233.5 ± 141.9, mean + SD) was significantly less than in the placebo group (359.6 ± 104.1 ; P < 0.05).
Conclusion
Preemptive gabapentin 300 mg po significantly decreases the severity of pain postoperatively in patients who undergo single-level lumbar discoidectomy.
Résumé
Objectif
Vérifier si l’usage préventif de gabapentine, analogue structurel de l’acide gamma amino-butyrique, pouvait réduire la douleur postopératoire et la consommation de fentanyl dans les cas de discectomie lombaire à un seul niveau.
Méthode
Cinquante-six patients d’état physique ASA I et II, répartis au hasard en deux groupes égaux, ont reçu soit 300 mg de gabapentine, soit un placebo, deux heures avant l’opération. Après l’opération, la douleur a été évaluée selon une échelle visuelle analogique (EVA) de 0–6, 6–12, 12–18 et 18–24 h au repos. La consommation totale de fentanyl pendant les 24 premières heures postopératoires a aussi été notée. Une dose iv de 2 μg·kg−1 de fentanyl a été utilisée pour traiter la douleur postopératoire sur demande.
Résultats
Les patients sous gabapentine ont eu des scores significativement plus bas à l’EVA, pour toutes les mesures aux intervalles de 0–6, 6–12, 12–18 et 18–24 h, que ceux du groupe placebo (3,5 ± 2,3 ; 3,2 ±2,1 ; 1,8 ± 1,7 ; 1,2 ± 1,3 vs 6,1 ± 1,7 ; 4,4 ± 1,2 ; 3,3 ± 1,1 ; 2,1 ± 1,2 ; P < 0,05). La consommation postopératoire totale de fentanyl pendant les 24 premières heures a été significativement plus faible avec la gabapentine (233,5 ± 141,9, moyenne + écart type) qu’avec le placebo (359,6 ± 104,1 ; P < 0,05).
Conclusion
L’administration préventive de 300 mg po de gabapentine diminue significativement la sévérité de la douleur postopératoire chez les patients qui subissent une discectomie lombaire à un seul niveau.
Similar content being viewed by others


References
Abdi S, Lee DH, Chung JM. The anti-allodynic effects of amitriptyline, gabapentin, and lidocaine in a rat model of neuropathic pain. Anesth Analg 1998; 87: 1360–6.
Goa KL, Sorkin EM. Gabapentin. A review of its pharmacological properties and clinical potential in epilepsy. Drugs 1993; 46: 409–27.
Dirks J, Fredensborg BB, Christensen D, Fomsgaard JS, Flyger H, Dahl JB. A randomized study of the effects of single-dose gabapentin versus placebo on postoperative pain and morphine consumption after mastectomy. Anesthesiology 2002; 97: 560–4.
Mao J, Chen LL. Gabapentin in pain management. Anesth Analg 2000; 91: 680–7.
Field MJ, Holloman FF, McCleary S, Hughes J, Singh L. Evaluation of gabapentin and S-( + )−3-isobutylgaba in a rat model of postoperative pain. J Pharmacol Exp Ther 1997; 282: 1242–6.
Dirks J, Petersen KL, Rowbotham MC, Dahl JB. Gabapentin suppresses cutaneous hyperalgesia following heat/capsaicin sensitization. Anesthesiology 2002; 97: 102–6.
Petersen KL, Jones B, Segredo V, Dahl JB, Rowbotham MC. Effect of ramifentanil on pain and secondary hyperalgesia associated with the heat-capsaicin sensitization model in healthy volunteers. Anesthesiology 2001; 94: 15–20.
Kissin I. Preemptive analgesia. Why its effect is not always obvious (Editorial). Anesthesiology 1996; 84: 1015–9.
Fassoulaki A, Patris K, Sarantopoulos C, Hogan Q. The analgesic effect of gabapentin and mexiletine after breast surgery for cancer. Anesth Analg 2002; 95: 985–91.
Eckhardt K, Ammon S, Hofmann U, Riebe A, Gugeler N, Mikus G. Gabapentin enhances the analgesic effect of morphine in healthy volunteers. Anesth Analg 2000; 91: 185–91.
Woolf CJ, Chong MS. Preemptive analgesia-treating postoperative pain by preventing the establishment of central sensitization. Anesth Analg 1993; 77: 362–79.
Kissin I. Preemptive analgesia. Anesthesiology 2000; 93: 1138–43.
Gilron I. Is gabapentin a “broad-spectrum” analgesic? (Editorial). Anesthesiology 2002; 97: 537–9.
Pandey CK, Bose N, Garg G, et al. Gabapentin for the treatment of pain in Guillain-Barre syndrome: a double-blinded, placebo-controlled, crossover study. Anesth Analg 2002; 95: 1719–23.
Nicholson B. Gabapentin use in neuropathic pain syndromes. Acta Neurol Scand 2000; 101: 359–71.
Feng Y, Cui M, Willis WD. Gabapentin markedly reduces acetic acid-induced visceral nociception. Anesthesiology 2003; 98: 729–33.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Pandey, C.K., Sahay, S., Gupta, D. et al. Preemptive gabapentin decreases postoperative pain after lumbar discoidectomy. Can J Anesth 51, 986–989 (2004). https://doi.org/10.1007/BF03018484
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03018484