
Abstract
Background: Randomized trials have demonstrated the efficacy of 1- and 2-cm excision margins for thin and intermediate-thickness melanomas, respectively. The optimal margin of excision for thick melanomas is still unknown, however. We evaluated whether the margins used for intermediate-thickness melanomas can be applied safely to thicker lesions.
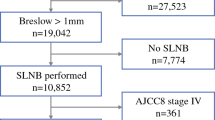
Methods: The charts of 278 patients with thick primary melanomas treated between 1985 and 1996 were retrospectively reviewed. Patients with distant metastases at presentation or with follow-up less than 6 months were excluded. Median follow-up was 27 months. Known melanoma prognostic factors and excision margins were evaluated for their impact on local recurrence (LR), disease-free survival (DFS), and overall survival (OS).
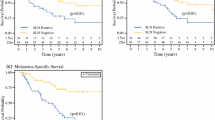
Results: Median tumor thickness was 6.0 mm, and 57% were ulcerated. At presentation, 201 patients (72%) were node negative and 77 (28%) were node positive (palpable or occult). The 5-year OS and DFS rates were 55% and 30%, respectively. The LR rate for all patients was 12%. Although nodal status, thickness, and ulceration were significantly associated with OS by multivariate analysis, neither LR nor excisional margin (<2 cm vs. >2 cm) significantly affected DFS or OS in these patients.
Conclusions: Because margins of excision greater than 2 cm do not improve LR, DFS, or OS compared to a margin of 2 cm or less, a 2-cm margin of excision is adequate for patients with thick melanoma. Because nodal status is a significant prognostic factor in these patients, staging by sentinel node biopsy should be considered in patients with thick melanomas and clinically negative nodal basins to allow proper entry and stratification in adjuvant therapy trials.
Similar content being viewed by others

References
Breslow A, Macht SD. Optimal size of resection for thin cutaneous melanoma.Surg Gynecol Obstet 1977;145:691–2.
Balch CM, Murad TM, Soong S-J, Ingalls AL, Richards PC, Maddox W. Tumor thickness as a guide to surgical management of clinical stage I melanoma patients.Cancer 1979;43:883–8.
Aitken DR, James AG, Carey LC. Local cutaneous recurrence after conservative excision of malignant melanoma.Arch Surg 1984;119:643–6.
Cascinelli N, van der Esch EP, Breslow A, Morabito A, Bufalino R. W.H.O. Collaborating Centres for Evaluation of Methods of Diagnosis and Treatment of Melanoma. Stage I melanoma of the skin: the problem of resection margins.Eur J Cancer Clin Oncol 1980;16:1079–85.
Cosimi AB, Sober AJ, Mihm MC, Fitzpatrick TB. Conservative surgical management of superficially invasive cutaneous melanoma.Cancer 1984;53:1256–9.
Elder DE, Guerry D, Heiberger RM, et al. Optimal resection margins for cutaneous malignant melanoma.Plast Reconstr Surg 1983;71:66–72.
Everall JD, Dowd PM. Diagnosis, prognosis, and treatment of melanoma.Lancet 1977;2:286–9.
Kelly KW, Sagebiel RW, Calderon W, Murillo L, Dakin RL, Blois MS. The frequency of local recurrence and microsatellites as a guide to reexcision margins for cutaneous malignant melanoma.Ann Surg 1984;200:759–61.
Taylor BA, Hughes LE. A policy of selective excision for primary cutaneous malignant melanoma.Eur J Surg Oncol 1985;11:7–13.
Veronesi U, Bajetta E, Cascinelli N, Clemente C, Rilke F. New trends in the treatment of malignant melanoma.Int Adv Surg Oncol 1978;1:113–56.
Day CL Jr, Mihm MC, Sober AJ, Fitzpatrick TB, Malt RA. Narrow margins for clinical stage I malignant melanoma.N Engl J Med 1982;306:479–82.
Veronesi U, Cascinelli N, Adamus J, Balch C, Bandeira D, et al. Thin stage I primary cutaneous malignant melanoma: comparison of excision with margins of 1 or 3 cm.N Engl J Med 1988;318:1159–1162.
Veronesi U, Cascinelli N. Narrow excision (1-cm margin): a safe procedure for thin cutaneous melanoma.Arch Surg 1991;126:438–41.
Balch C, Urist M, Karakousis C, Smith T, Temple W, et al. Efficacy of 2-cm surgical margins for intermediate-thickness melanomas (1 to 4 mm).Ann Surg 1993;218:262–9.
Beahrs O, Henson D, Hutter R, Kennedy B, eds.Manual for Staging of Cancer, 4th ed. Philadelphia: JB Lippincott, 1993:155–160.
Balch C, Soong S-J, Shaw H, Urist M, McCarthy W. An analysis of prognostic factors in 8500 patients with cutaneous melanoma. In: Balch C, Houghton A, Milton G, Sober A, Soong S-J, eds.Cutaneous Melanoma. Philadelphia: JB Lippincott, 1992:165–91.
Parker S, Tong T, Bolden S, Wingo P. Cancer statistics 1997.CA Cancer J Clin 1997;47:5–27.
Ames F, Balch C, Reintgen D. Local recurrences and their management. In: Balch C, Houghton A, Milton G, Sober A, Soong S-J, eds.Cutaneous Melanoma. Philadelphia: JB Lippincott, 1992:287–94.
Karakousis C, Balch C, Urist M, Ross M, Smith T, Bartolucci A. Local recurrence in malignant melanoma: long-term results in the multiinstitutional randomized surgical trial.Ann Surg Oncol 1996;3:446–52.
Lewis M, Hill J, Leopold J, Hughes L. Guidelines for management of malignant melanoma of the lower limb based on a study of long-term behaviour.Clin Oncol 1982;8:341–9.
McNeer G, Cantin J. Local failure in the treatment of melanoma. The Janeway Lecture.Am J Roentgenol 1967;99:791–5.
Roses D, Harris M, Rigel D, Carrey Z, Friedman R, Kopf A. Local and in-transit metastases following definitive excision for primary cutaneous malignant melanoma.Ann Surg 1983;198:65–9.
O'Rourke M, Altmann C. Melanoma recurrence after excision: is a wide margin justified?Ann Surg 1993;217:2–5.
Reintgen D, Vollmer R, Tso C, Seigler H. Prognosis for recurrent stage I malignant melanoma.Arch Surg 1987;122:1338–42.
Kirkwood J, Strawderman M, Ernstoff M, Smith T, Borden E, Blum R. Interferon alpha-2b adjuvant therapy of high-risk resected cutaneous melanoma: The Eastern Cooperative Oncology Group Trial EST 1684.J Clin Oncol 1996;14:7–17.
Cole B, Gelber R, Kirkwood J, Goldhirsch A, Barylak E, Borden E. Quality of life adjusted survival analysis of interferon alpha-2b adjuvant treatment of high risk resected cutaneous melanoma: an ECOG study.J Clin Oncol 1996;14:2666–73.
Crowley N, Seigler H. The role of elective lymph node dissection in the management of patients with thick cutaneous melanoma.Cancer 1990;6:2522–7.
Balch C, Soong S, Bartolucci A, et al. Efficacy of an elective lymph node dissection of 1 to 4 mm thick melanomas for patients 60 years of age and younger.Ann Surg 1996;224:255–66.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Heaton, K.M., Sussman, J.J., Gershenwald, J.E. et al. Surgical margins and prognostic factors in patients with thick (>4 mm) primary melanoma. Annals of Surgical Oncology 5, 322–328 (1998). https://doi.org/10.1007/BF02303495
Issue Date:
DOI: https://doi.org/10.1007/BF02303495