Genotypic and Phenotypic Resistance to Clarithromycin in Helicobacter pylori Strains

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Culture and Antimicrobial Susceptibility Test
2.2. Detection of Mutations in the 23S rRNA Genes, Using Next-Generation Sequencing
2.3. Statistical Analysis
3. Results
3.1. Prevalence of Antimicrobial Resistance to Clarithromycin
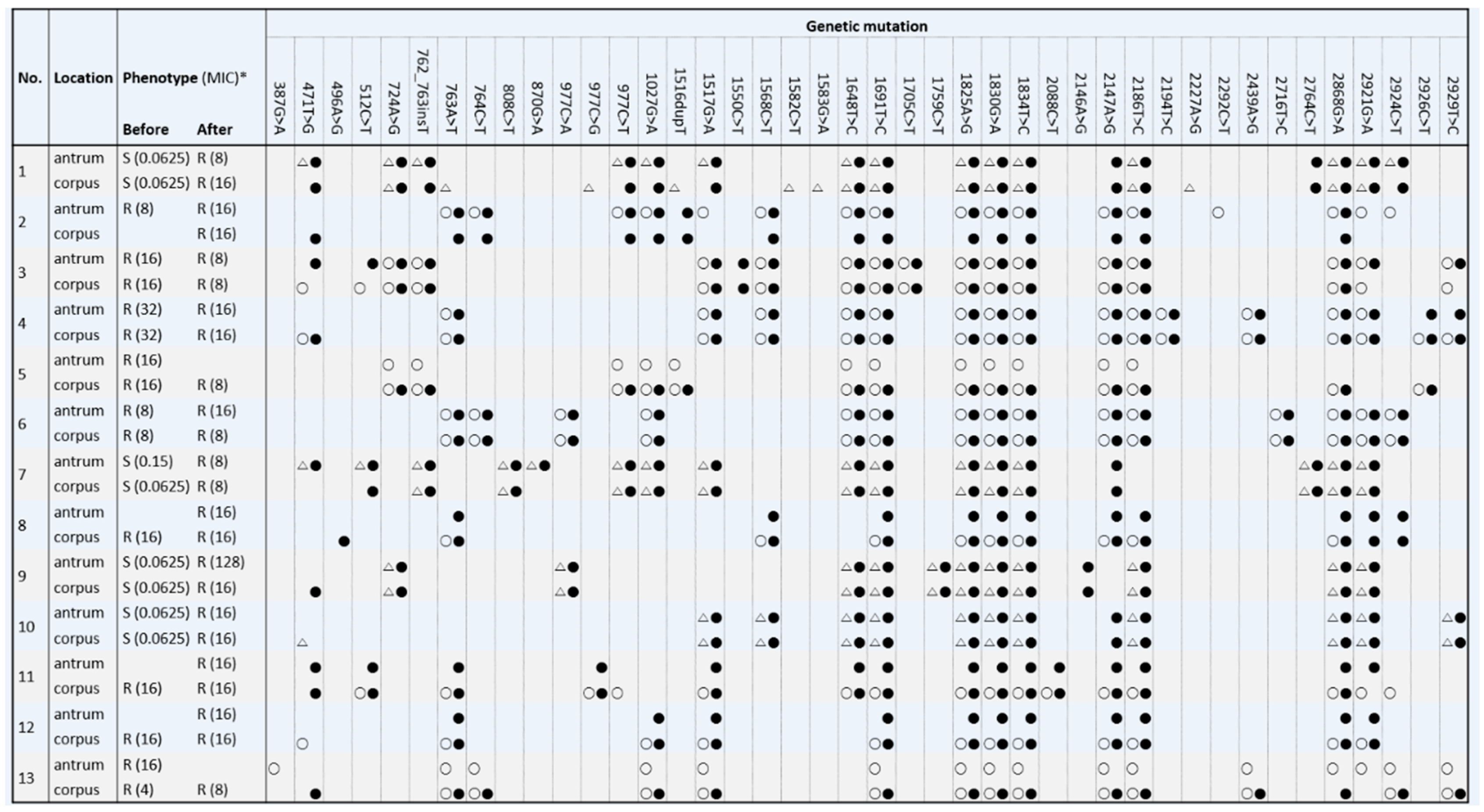
3.2. Mutations in the 23S rRNA Genes
3.3. Genotypic and Phenotypic Resistance to Clarithromycin
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Suerbaum, S.; Michetti, P. Helicobacter pylori Infection. N. Engl. J. Med. 2002, 347, 1175–1186. [Google Scholar] [CrossRef] [Green Version]
- Malfertheiner, P.; Megraud, F.; A O’Morain, C.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection—the Maastricht V/Florence Consensus Report. Gut 2016, 66, 6–30. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Choi, K.D.; Jung, H.-Y.; Baik, G.H.; Park, J.K.; Kim, S.S.; Kim, B.-W.; Hong, S.J.; Lim, H.; Shin, C.M.; et al. Seroprevalence of Helicobacter pylori in Korea: A multicenter, nationwide study conducted in 2015 and 2016. Helicobacter 2018, 23, e12463. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.G.; Jung, H.K.; Lee, H.L.; Jang, J.Y.; Lee, H.; Kim, C.G.; Shin, W.G.; Shin, E.S.; Lee, Y.C. Guidelines for the diagnosis and treatment of Helicobacter pylori infection in Korea, 2013 revised edition. Korean J. Gastroenterol. 2013, 62, 3–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mégraud, F. H pylori antibiotic resistance: Prevalence, importance, and advances in testing. Gut 2004, 53, 1374–1384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gong, E.J.; Yun, S.-C.; Jung, H.-Y.; Lim, H.; Choi, K.-S.; Ahn, J.Y.; Lee, J.H.; Kim, D.H.; Choi, K.D.; Song, H.J.; et al. Meta-Analysis of First-Line Triple Therapy for Helicobacter pylori Eradication in Korea: Is It Time to Change? J. Korean Med. Sci. 2014, 29, 704–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thung, I.; Aramin, H.; Vavinskaya, V.; Gupta, S.; Park, J.Y.; Crowe, S.E.; Valasek, M.A. Review article: The global emergence of Helicobacter pylori antibiotic resistance. Aliment. Pharmacol. Ther. 2015, 43, 514–533. [Google Scholar] [CrossRef] [Green Version]
- Graham, D.Y.; Fischbach, L. Helicobacter pylori treatment in the era of increasing antibiotic resistance. Gut 2010, 59, 1143–1153. [Google Scholar] [CrossRef] [PubMed]
- Cosme, A.; Montes, M.; Martos, M.; Gil, I.; Mendarte, U.; Salicio, Y.; Piñeiro, L.; Recasens, M.; Ibarra, B.; Sarasqueta, C.; et al. Usefulness of antimicrobial susceptibility in the eradication of Helicobacter pylori. Clin. Microbiol. Infect. 2013, 19, 379–383. [Google Scholar] [CrossRef] [Green Version]
- Park, C.-S.; Lee, S.-M.; Park, C.-H.; Koh, H.-R.; Jun, C.H.; Park, S.-Y.; Lee, W.-S.; Joo, Y.-E.; Kim, H.-S.; Choi, S.-K.; et al. Pretreatment Antimicrobial Susceptibility-Guided Vs. Clarithromycin-Based Triple Therapy for Helicobacter pylori Eradication in a Region With High Rates of Multiple Drug Resistance. Am. J. Gastroenterol. 2014, 109, 1595–1602. [Google Scholar] [CrossRef]
- López-Góngora, S.; Puig, I.; Calvet, X.; Villoria, A.; Baylina, M.; Muñoz, N.; Sanchez-Delgado, J.; Suarez, D.; García-Hernando, V.; Gisbert, J.P. Systematic review and meta-analysis: Susceptibility-guided versus empirical antibiotic treatment for Helicobacter pylori infection. J. Antimicrob. Chemother. 2015, 70, 2447–2455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Versalovic, J.; Osato, M.S.; Spakovsky, K.; Dore, M.P.; Reddy, R.; Stone, G.G.; Shortridge, D.; Flamm, R.K.; Tanaka, S.K.; Graham, D.Y. Point mutations in the 23S rRNA gene of Helicobacter pylori associated with different levels of clarithromycin resistance. J. Antimicrob. Chemother. 1997, 40, 283–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Arata, M.I.; Baquero, F.; De Rafael, L.; De Argila, C.M.; Gisbert, J.P.; Bermejo, F.; Boixeda, D.; Cantón, R. Mutations in 23S rRNA in Helicobacter pylori Conferring Resistance to Erythromycin Do Not Always Confer Resistance to Clarithromycin. Antimicrob. Agents Chemother. 1999, 43, 374–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gong, E.J.; Ahn, J.Y. Antimicrobial Resistance of Helicobacter pylori Isolates in Korea. Korean J. Helicobacter Up. Gastrointest. Res. 2018, 18, 82–88. [Google Scholar] [CrossRef] [Green Version]
- Tuan, V.P.; Narith, D.; Tshibangu-Kabamba, E.; Dung, H.D.Q.; Viet, P.T.; Sokomoth, S.; Binh, T.T.; Sokhem, S.; Tri, T.D.; Ngov, S.; et al. A Next-Generation Sequencing-Based Approach to Identify Genetic Determinants of Antibiotic Resistance in Cambodian Helicobacter pylori Clinical Isolates. J. Clin. Med. 2019, 8, 858. [Google Scholar] [CrossRef] [Green Version]
- Hulten, K.G.; Gibreel, A.; Sköld, O.; Engstrand, L. Macrolide resistance in Helicobacter pylori: Mechanism and stability in strains from clarithromycin-treated patients. Antimicrob. Agents Chemother. 1997, 41, 2550–2553. [Google Scholar] [CrossRef] [Green Version]
- Khan, R.; Nahar, S.; Sultana, J.; Ahmad, M.M.; Rahman, M. T2182C Mutation in 23S rRNA Is Associated with Clarithromycin Resistance in Helicobacter pylori Isolates Obtained in Bangladesh. Antimicrob. Agents Chemother. 2004, 48, 3567–3569. [Google Scholar] [CrossRef] [Green Version]
- EUCAST clinical breakpoint tables v. 10.0, valid from 2020-01-01. Helicobacter pylori. Available online: http://www.eucast.org/clinical_breakpoints (accessed on 17 May 2020).
- Kim, J.M.; Kim, J.S.; Kim, N.; Kim, S.G.; Jung, H.C.; Song, I.S. Comparison of primary and secondary antimicrobial minimum inhibitory concentrations for Helicobacter pylori isolated from Korean patients. Int. J. Antimicrob. Agents 2006, 28, 6–13. [Google Scholar] [CrossRef]
- Taylor, D.E.; Ge, Z.; Purych, D.; Lo, T.; Hiratsuka, K. Cloning and sequence analysis of two copies of a 23S rRNA gene from Helicobacter pylori and association of clarithromycin resistance with 23S rRNA mutations. Antimicrob. Agents Chemother. 1997, 41, 2621–2628. [Google Scholar] [CrossRef] [Green Version]
- Saranathan, R.; Levi, M.H.; Wattam, A.R.; Malek, A.; Asare, E.; Behin, D.S.; Pan, D.H.; Jacobs, W.R.; Szymczak, W. Helicobacter pylori Infections in the Bronx, New York: Surveying Antibiotic Susceptibility and Strain Lineage by Whole-Genome Sequencing. J. Clin. Microbiol. 2019, 58, 58. [Google Scholar] [CrossRef]
- Lauener, F.N.; Imkamp, F.; Lehours, P.; Buissonnière, A.; Bénejat, L.; Zbinden, R.; Keller, P.M.; Wagner, K. Genetic Determinants and Prediction of Antibiotic Resistance Phenotypes in Helicobacter pylori. J. Clin. Med. 2019, 8, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, T.J.; Kim, N.; Kim, W.J.; Lee, B.H.; Nam, R.H.; Park, J.H.; Lee, M.K.; Park, Y.S.; Lee, N.H.; Jung, H.C.; et al. Change in Antibiotic Resistance of Helicobacter pylori Strains and the Effect of A2143G Point Mutation of 23S rRNA on the Eradication of H. pylori in a Single Center of Korea. J. Clin. Gastroenterol. 2010, 44, 1. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Cunningham, S.A.; Cole, N.C.; Kohner, P.C.; Mandrekar, J.N.; Patel, R. Phenotypic and Molecular Antimicrobial Susceptibility of Helicobacter pylori. Antimicrob. Agents Chemother. 2017, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerrits, M.M.; Van Vliet, A.H.; Kuipers, E.J.; Kusters, J.G. Helicobacter pylori and antimicrobial resistance: Molecular mechanisms and clinical implications. Lancet Infect. Dis. 2006, 6, 699–709. [Google Scholar] [CrossRef]
- Occhialini, A.; Urdaci, M.C.; Doucet-Populaire, F.; Bebear, C.; Lamouliatte, H.; Mégraud, F. Macrolide resistance in Helicobacter pylori: Rapid detection of point mutations and assays of macrolide binding to ribosomes. Antimicrob. Agents Chemother. 1997, 41, 2724–2728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, V.H.; Ha, T.M.T.; Le, P.T.Q.; Phan, T.N.; Tran, T.N.H. Characterisation of point mutations in domain V of the 23S rRNA gene of clinical Helicobacter pylori strains and clarithromycin-resistant phenotype in central Vietnam. J. Glob. Antimicrob. Resist. 2019, 16, 87–91. [Google Scholar] [CrossRef]
- Kim, S.J.; Kim, J.G.; Jung, K.; Hong, Y.H.; Kim, J.H.; Jung, H.R.; Kwon, J.H.; Yang, Y.H.; Kim, H.J.; Do, J.H.; et al. Antimicrobial resistance rate of Helicobacter pylori isolates and detection of mechanism of clarithromycin resistance. Korean J. Med. 2001, 61, 470–478. [Google Scholar]
- Kim, J.M.; Kim, J.S.; Kim, N.; Kim, Y.-J.; Kim, I.Y.; Chee, Y.J.; Lee, C.-H.; Jung, H.C. Gene mutations of 23S rRNA associated with clarithromycin resistance in Helicobacter pylori strains isolated from Korean patients. J. Microbiol. Biotechnol. 2008, 18, 1584–1589. [Google Scholar]
- Binh, T.T.; Shiota, S.; Suzuki, R.; Matsuda, M.; Trang, T.T.H.; Kwon, D.H.; Iwatani, S.; Yamaoka, Y. Discovery of novel mutations for clarithromycin resistance in Helicobacter pylori by using next-generation sequencing. J. Antimicrob. Chemother. 2014, 69, 1796–1803. [Google Scholar] [CrossRef] [Green Version]
- Rimbara, E.; Noguchi, N.; Kijima, H.; Yamaguchi, T.; Kawai, T.; Sasatsu, M. Mutations in the 23S rRNA gene of clarithromycin-resistant Helicobacter pylori from Japan. Int. J. Antimicrob. Agents 2007, 30, 250–254. [Google Scholar] [CrossRef]
- Lee, H.K.; Chae, H.S.; Kang, J.O.; Lee, M.-K.; Sung, H.; Kim, M.-N.; Lee, J.; Lee, M.; Shim, K.-N. Multicenter Study for the Frequency of 23S rRNA Point Mutations Associated with Clarithromycin Resistance in Helicobacter pylori in Korea. Korean J. Clin. Microbiol. 2008, 11, 84. [Google Scholar] [CrossRef]
- De Francesco, V.; Margiotta, M.; Zullo, A.; Hassan, C.; Troiani, L.; Burattini, O.; Stella, F.; Di Leo, A.; Russo, F.; Marangi, S.; et al. Clarithromycin-resistant genotypes and eradication of Helicobacter pylori. Ann. Intern. Med. 2006, 144, 94–100. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, V.; Zullo, A.; Ierardi, E.; Giorgio, F.; Perna, F.; Hassan, C.; Panella, C.; Vaira, D. The A2143G Point Mutation of Clarithromycin Resistance Affects Helicobacter pylori Eradication. J. Clin. Gastroenterol. 2009, 43, 386. [Google Scholar] [CrossRef]
- De Francesco, V.; Zullo, A.; Ierardi, E.; Giorgio, F.; Perna, F.; Hassan, C.; Morini, S.; Panella, C.; Vaira, D. Phenotypic and genotypic Helicobacter pylori clarithromycin resistance and therapeutic outcome: Benefits and limits. J. Antimicrob. Chemother. 2009, 65, 327–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Shin, J.-H.; Roe, I.H.; Sohn, S.G.; Lee, J.H.; Kang, G.H.; Lee, H.-K.; Jeong, B.C.; Lee, S.H. Impact of Clarithromycin Resistance on Eradication of Helicobacter pylori in Infected Adults. Antimicrob. Agents Chemother. 2005, 49, 1600–1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liou, J.; Chang, C.-Y.; Sheng, W.-H.; Wang, Y.-C.; Chen, M.-J.; Lee, Y.; Hung, H.-W.; Chian, H.; Chang, S.-C.; Wu, M.-S.; et al. Genotypic Resistance in Helicobacter pylori Strains Correlates with Susceptibility Test and Treatment Outcomes after Levofloxacin- and Clarithromycin-Based Therapies. Antimicrob. Agents Chemother. 2010, 55, 1123–1129. [Google Scholar] [CrossRef] [Green Version]
- Burucoa, C.; Landron, C.; Garnier, M.; Fauchere, J.-L.; Khan, R.; Rahman, M. T2182C Mutation Is Not Associated with Clarithromycin Resistance in Helicobacter pylori. Antimicrob. Agents Chemother. 2005, 49, 868–870. [Google Scholar] [CrossRef] [Green Version]
- Garrido, L.; Toledo, H. Novel Genotypes in Helicobacter pylori Involving Domain V of the 23S rRNA Gene. Helicobacter 2007, 12, 505–509. [Google Scholar] [CrossRef]


{kind=link}
| Strain No. | Phenotype | Allele at 2146 | Allele at 2147 | Strain No. | Phenotype | Allele at 2146 | Allele at 2147 |
|---|---|---|---|---|---|---|---|
| 1 | Susceptible | A | A | 24 | Susceptible | A | A |
| 2 | Susceptible | A | A | 25 | Resistant | A | G |
| 3 | Resistant | A | G | 26 | Resistant | A | G |
| 4 | Resistant | A | G | 27 | Resistant | A | G |
| 5 | Resistant | A | G | 28 | Resistant | A | G |
| 6 | Resistant | A | G | 29 | Resistant | A | G |
| 7 | Resistant | A | G | 30 | Susceptible | A | A |
| 8 | Resistant | A | G | 31 | Susceptible | A | A |
| 9 | Resistant | A | G | 32 | Resistant | G | A |
| 10 | Resistant | A | G | 33 | Resistant | G | A |
| 11 | Resistant | A | G | 34 | Susceptible | A | A |
| 12 | Resistant | A | G | 35 | Susceptible | A | A |
| 13 | Resistant | A | G | 36 | Resistant | A | G |
| 14 | Resistant | A | G | 37 | Resistant | A | G |
| 15 | Resistant | A | G | 38 | Resistant | A | G |
| 16 | Resistant | A | G | 39 | Resistant | A | G |
| 17 | Resistant | A | G | 40 | Resistant | A | G |
| 18 | Resistant | A | G | 41 | Resistant | A | G |
| 19 | Resistant | A | G | 42 | Resistant | A | G |
| 20 | Resistant | A | G | 43 | Resistant | A | G |
| 21 | Resistant | A | G | 44 | Resistant | A | G |
| 22 | Resistant | A | G | 45 | Resistant | A | G |
| 23 | Susceptible | A | A | 46 | Resistant | A | G |
| Mutation * | Corresponding Allele | Frequency, n (%) | Mutant: Wild Type (Frequency, %) | p-Value | |
|---|---|---|---|---|---|
| Susceptible | Resistant | ||||
| 387G>A (383) | A | 1 (2.2) | 0:8 (0) | 1:37 (2.6) | >0.999 |
| 471T>G (467) | T | 16 (34.8) | 5:3 (62.5) | 27:11 (71.1) | 0.684 |
| 496A>G (492) | G | 1 (2.2) | 0:8 (0) | 1:37 (2.6) | >0.999 |
| 512C>T (508) | T | 8 (17.4) | 1:7 (12.5) | 7:31 (18.4) | >0.999 |
| 724A>G (720) | A | 15 (32.6) | 4:4 (50.0) | 27:11 (71.1) | 0.407 |
| 762_763insT (758) | No ins | 14 (30.4) | 5:3 (62.5) | 27:11 (71.1) | 0.684 |
| 763A>T (759) | T | 24 (52.2) | 1:7 (12.5) | 23:15 (60.5) | 0.020 |
| 764C>T (760) | T | 10 (21.7) | 0:8 (0) | 10:28 (26.3) | 0.171 |
| 808C>T (804) | C | 4 (8.7) | 6:2 (75.0) | 36:2 (94.7) | 0.134 |
| 870G>A (866) | G | 2 (4.3) | 7:1 (87.5) | 37:1 (97.4) | 0.321 |
| 977C>A (973) | C | 8 (17.4) | 6:2 (75.0) | 32:6 (84.2) | 0.613 |
| 977C>G (973) | C | 4 (8.7) | 7:1 (87.5) | 35:3 (92.1) | 0.548 |
| 977C>T (973) | C | 13 (28.3) | 5:3 (62.5) | 28:10 (73.7) | 0.669 |
| 1027G>A (1023) | A | 23 (50.0) | 3:5 (37.5) | 20:18 (52.6) | 0.700 |
| 1516dupT (1512) | TT | 6 (13.0) | 1:7 (12.5) | 5:33 (13.2) | >0.999 |
| 1517G>A (1513) | A | 29 (63.0) | 5:3 (62.5) | 24:14 (63.2) | >0.999 |
| 1550C>T (1546) | T | 2 (4.3) | 0:8 (0) | 2:36 (5.3) | >0.999 |
| 1568C>T (1564) | T | 18 (39.1) | 2:6 (25.0) | 16:22 (42.1) | 0.453 |
| 1582C>T (1578) | C | 1 (2.2) | 7:1 (87.5) | 38:0 (100.0) | 0.174 |
| 1583G>A (1579) | G | 1 (2.2) | 7:1 (87.5) | 38:0 (100.0) | 0.174 |
| 1648T>C (1644) | T | 37 (80.4) | 0:8 (0) | 9:29 (23.7) | 0.324 |
| 1705C>T (1701) | T | 4 (8.7) | 0:8 (0) | 4:34 (10.5) | >0.999 |
| 1759C>T (1755) | C | 4 (8.7) | 6:2 (75.0) | 36:2 (94.7) | 0.134 |
| 2088C>G (2084) | T | 3 (6.5) | 0:8 (0) | 3:35 (7.9) | >0.999 |
| 2146A>G (2142) | G | 2 (4.3) | 0:8 (0) | 2:36 (5.3) | >0.999 |
| 2147A>G (2143) | G | 36 (78.3) | 0:8 (0) | 36:2 (94.7) | <0.001 |
| 2186T>C (2182) | C | 42 (91.3) | 6:2 (75.0) | 36:2 (94.7) | 0.134 |
| 2194T>C (2190) | C | 4 (8.7) | 0:8 (0) | 4:34 (10.5) | >0.999 |
| 2227A>G (2223) | A | 1 (2.2) | 7:1 (87.5) | 38:0 (100.0) | 0.174 |
| 2292C>T (2288) | T | 1 (2.2) | 0:8 (0) | 1:37 (2.6) | >0.999 |
| 2439A>G (2434) | G | 7 (15.2) | 0:8 (0) | 7:31 (18.4) | 0.325 |
| 2716T>C (2711) | C | 4 (8.7) | 0:8 (0) | 4:34 (10.5) | >0.999 |
| 2764C>T (2759) | C | 6 (13.0) | 6:2 (75.0) | 34:4 (89.5) | 0.277 |
| 2868G>A (2860) | G | 44 (95.7) | 0:8 (0) | 2:36 (5.3) | >0.999 |
| 2921G>A (2913) | G | 36 (78.3) | 0:8 (0) | 10:28 (26.3) | 0.171 |
| 2924C>T (2916) | T | 14 (30.4) | 1:7 (12.5) | 13:25 (34.2) | 0.403 |
| 2926C>T (2918) | T | 5 (10.9) | 0:8 (0) | 5:33 (13.2) | 0.569 |
| 2929T>C (2921) | C | 13 (28.3) | 2:6 (25.0) | 11:27 (28.9) | >0.999 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gong, E.J.; Ahn, J.Y.; Kim, J.M.; Lee, S.M.; Na, H.K.; Lee, J.H.; Jung, K.W.; Choi, K.D.; Kim, D.H.; Song, H.J.; et al. Genotypic and Phenotypic Resistance to Clarithromycin in Helicobacter pylori Strains. J. Clin. Med. 2020, 9, 1930. https://doi.org/10.3390/jcm9061930
Gong EJ, Ahn JY, Kim JM, Lee SM, Na HK, Lee JH, Jung KW, Choi KD, Kim DH, Song HJ, et al. Genotypic and Phenotypic Resistance to Clarithromycin in Helicobacter pylori Strains. Journal of Clinical Medicine. 2020; 9(6):1930. https://doi.org/10.3390/jcm9061930
Chicago/Turabian StyleGong, Eun Jeong, Ji Yong Ahn, Jung Mogg Kim, Sun Mi Lee, Hee Kyong Na, Jeong Hoon Lee, Kee Wook Jung, Kee Don Choi, Do Hoon Kim, Ho June Song, and et al. 2020. "Genotypic and Phenotypic Resistance to Clarithromycin in Helicobacter pylori Strains" Journal of Clinical Medicine 9, no. 6: 1930. https://doi.org/10.3390/jcm9061930