GLP-1 Receptor Agonists and Diabetic Kidney Disease: A Call of Attention to Nephrologists

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Management of Diabetic Kidney Disease
2.1. BP Control
2.2. Blood Glucose Control
2.3. Obesity
3. GLP-1 Receptor Agonists
- Immunogenicity. Exendin-4 analogs are immunogenic, and, in some patients, the drug is inactivated by antibodies, whereas human GLP-1RA rarely induce antibody formation.
- Tolerance. Exendin-4 analogs are metabolized and eliminated by the kidneys, so they accumulate in CKD patients (precisely those with the highest cardiovascular risk), which may favor their withdrawal due to gastrointestinal intolerance. Human GLP-1RA, in contrast, are not eliminated by the kidneys.
- Production of GLP-19-36. Exendin-4 analogs are fully resistant to inactivation by DPP-4. Conversely, human GLP-1RA may be partially metabolized to small amounts of the metabolite GLP-19-36, which could have an additional cardioprotective effect, acting in the endothelial mitochondria through a non-GLP-1 receptor pathway.
4. GLP-1RA in Diabetic Kidney Disease Patients
4.1. Pharmacokinetics
4.2. Antihyperglycemic Efficacy of GLP-1RA in Patients with DKD
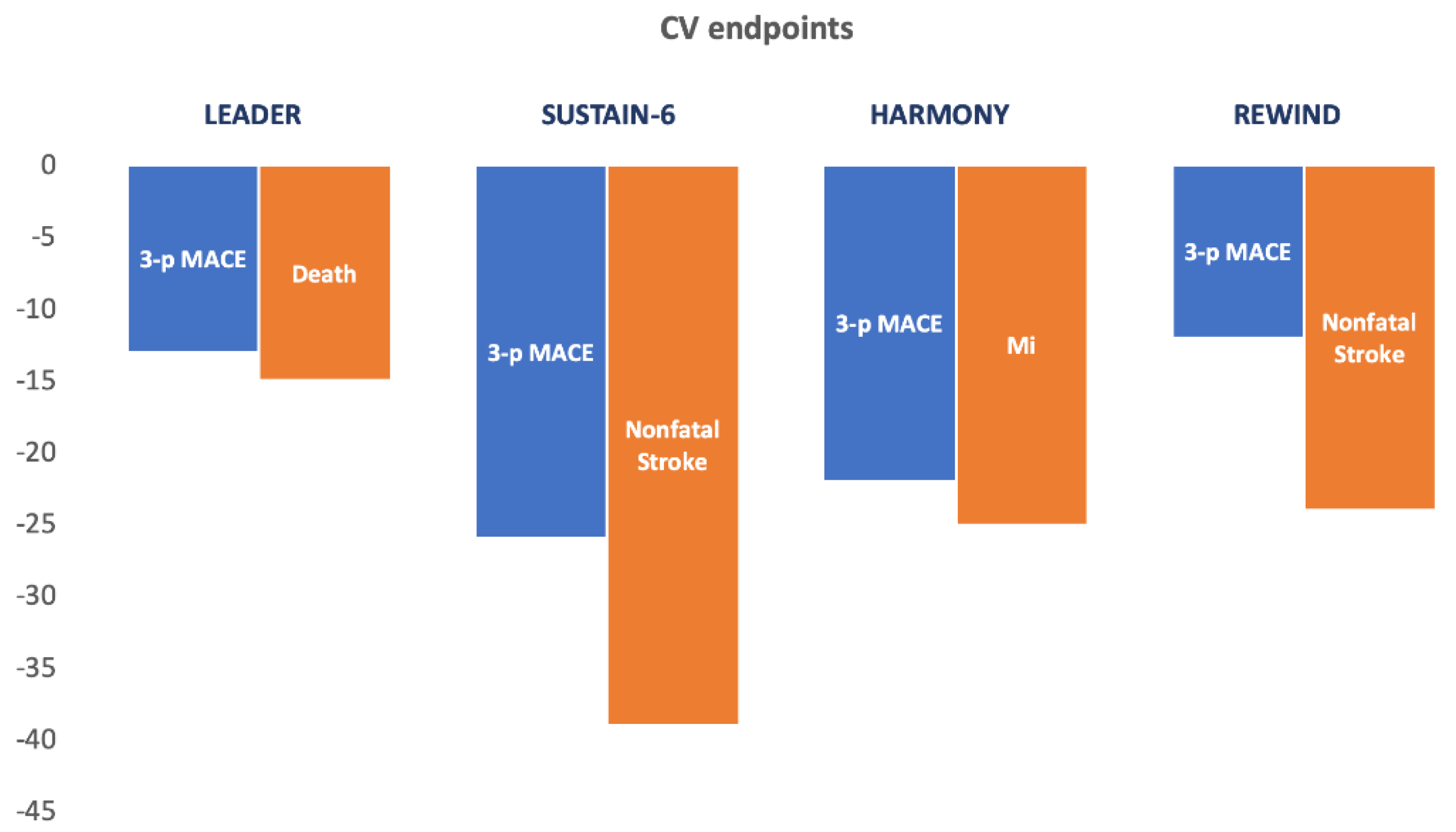
5. GLP-1 Receptor Agonists and Cardiovascular Outcomes
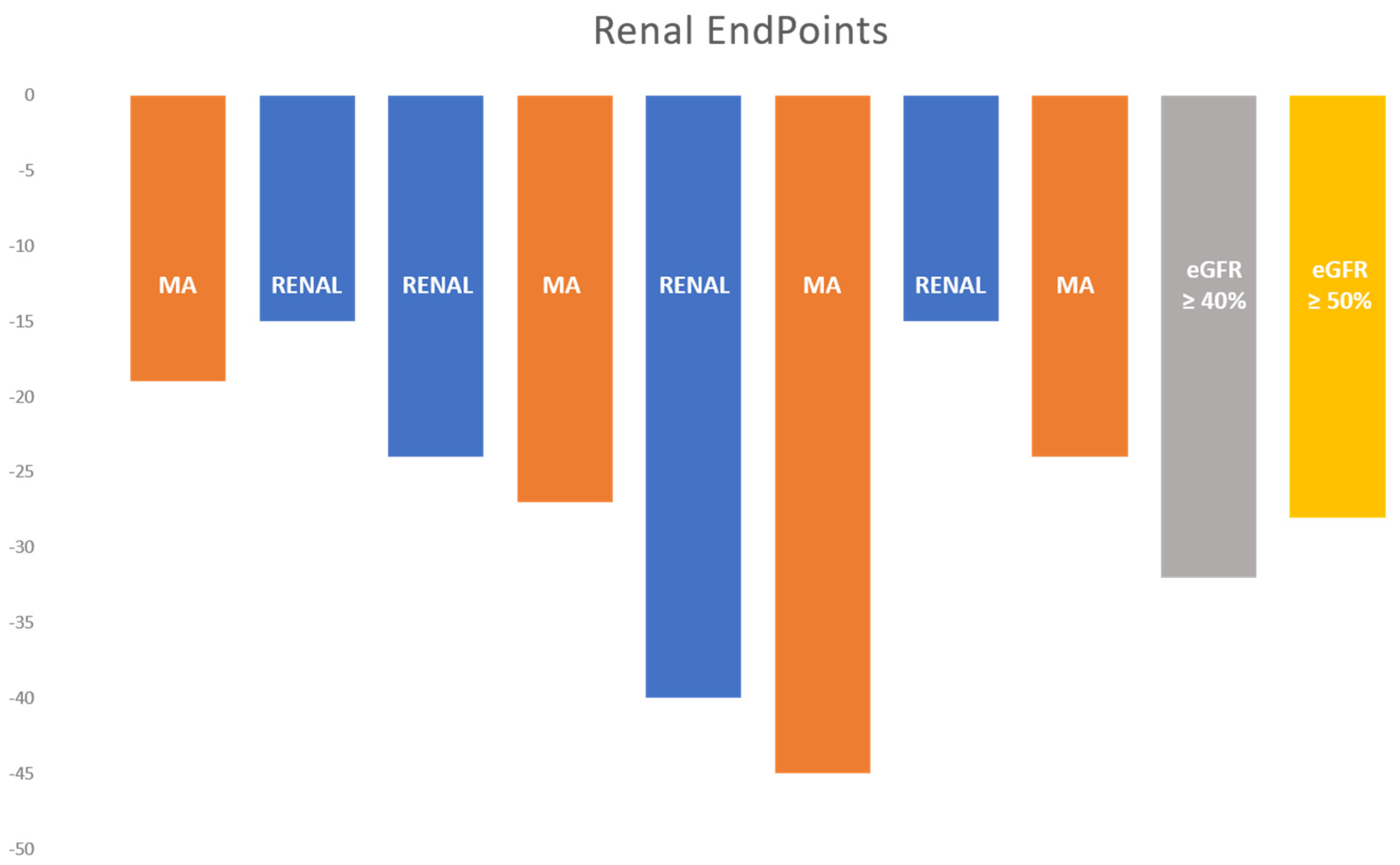
6. GLP-1 Receptor Agonists on Kidney Outcomes
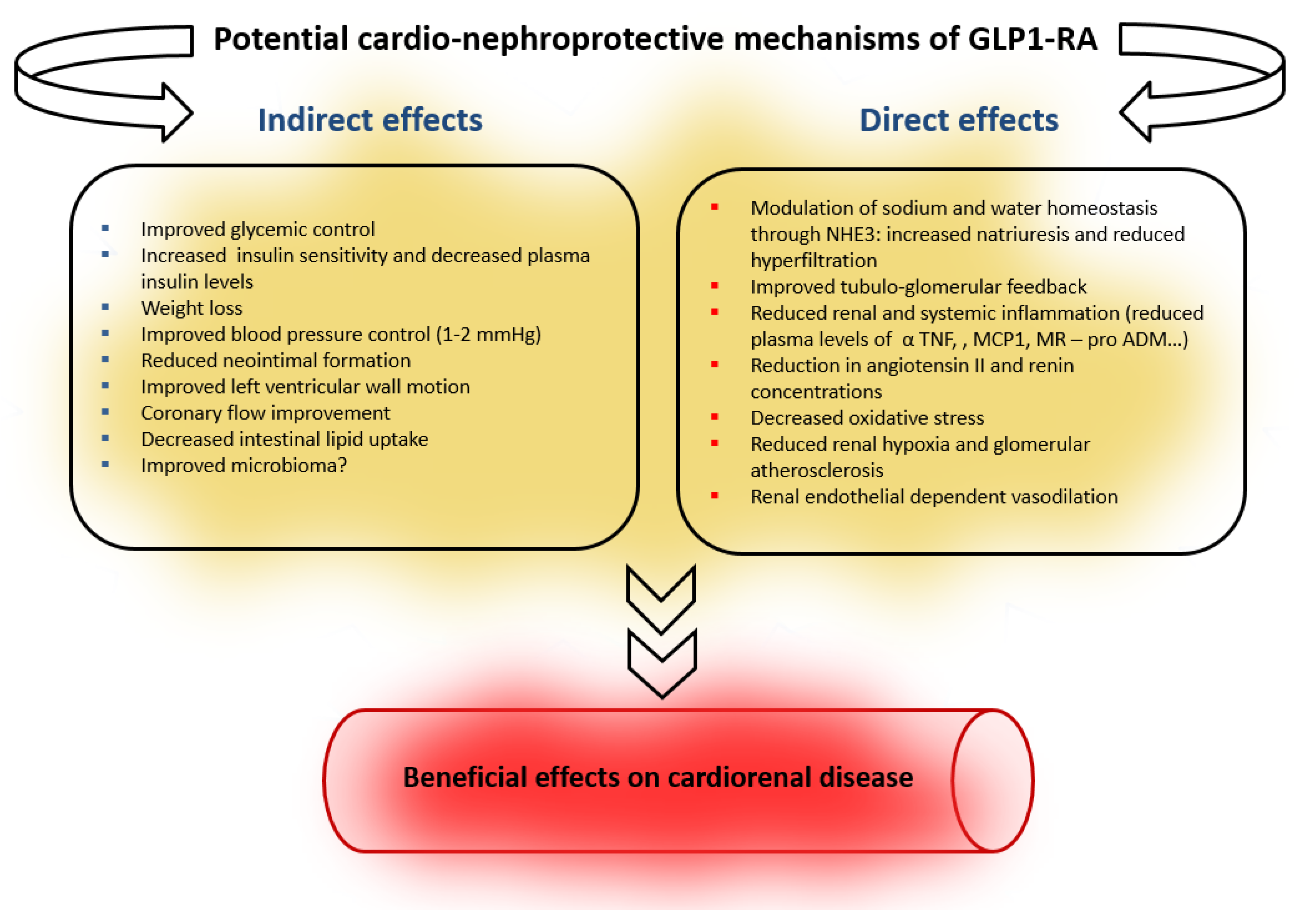
7. Potential Mechanisms for GLP-1RA-Associated Nephroprotection
7.1. GLP-1RA and Renal Hemodynamics
7.2. Modulation of Cyclic Adenosine Monophosphate–Protein Kinase a (Camp/PKA) Signaling and Other Anti-Inflammatory Pathways
8. Ongoing Studies and Unanswered Questions
9. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rodriguez-Poncelas, A.; Garre-Olmo, J.; Franch-Nadal, J.; Diez-Espino, J.; Mundet-Tuduri, X.; Barrot-De la Puente, J.; Coll-de Tuero, G.; RedGDPS Study Group. Prevalence of chronic kidney disease in patients with type 2 diabetes in Spain: PERCEDIME2 study. BMC Nephrol. 2013, 14, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, R.A.; Wang, Y.; Zhu, V.; Rupnow, M.F.T. Chronic kidney disease in US adults with type 2 diabetes: An updated national estimate of prevalence based on Kidney Disease: Improving Global Outcomes (KDIGO) staging. BMC Res. Notes 2014, 7, 415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adler, A.I.; Stevens, R.J.; Manley, S.E.; Bilous, R.W.; Cull, C.A.; Holman, R.R.; UKPDS GROUP. Development and progression of nephropathy in type 2 diabetes: The United Kingdom Prospective Diabetes Study (UKPDS 64). Kidney Int. 2003, 63, 225–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afkarian, M.; Sachs, M.C.; Kestenbaum, B.; Hirsch, I.B.; Tuttle, K.R.; Himmelfarb, J.; de Boer, I.H. Kidney disease and increased mortality risk in type 2 diabetes. J. Am. Soc. Nephrol. JASN 2013, 24, 302–308. [Google Scholar] [CrossRef]
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.-W.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [Green Version]
- Alicic, R.Z.; Rooney, M.T.; Tuttle, K.R. Diabetic Kidney Disease: Challenges, Progress, and Possibilities. Clin. J. Am. Soc. Nephrol. CJASN 2017, 12, 2032–2045. [Google Scholar] [CrossRef]
- United States Renal Data System. USRDS Annual Data Report Executive Summary USA. 2014. Available online: https://www.usrds.org/2014/view/v2_01.aspx (accessed on 28 March 2020).
- American Diabetes Association. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42 (Suppl. 1), S103–S123. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Castelao, A.; Górriz, J.L.; Segura-de la Morena, J.; Cebollada, J.; Escalada, J.; Esmatjes, E.; Fácila, L.; Gamarra, J.; Gràcia, S.; Hernánd-Moreno, J.; et al. Consensus document for the detection and management of chronic kidney disease. Nefrologia 2014, 34, 243–262. [Google Scholar]
- Factors in Development of Diabetic Neuropathy. Baseline analysis of neuropathy in feasibility phase of Diabetes Control and Complications Trial (DCCT). The DCCT Research Group. Diabetes 1988, 37, 476–481. [Google Scholar] [CrossRef]
- Ginsberg, J.S.; Zhan, M.; Diamantidis, C.J.; Woods, C.; Chen, J.; Fink, J.C. Patient-reported and actionable safety events in CKD. J. Am. Soc. Nephrol. 2014, 25, 1564–1573. [Google Scholar] [CrossRef] [Green Version]
- Farrington, K.; Covic, A.; Nistor, I.; Aucella, F.; Clyne, N.; de Vos, L.; Findlay, A.; Fouque, D.; Grodzicki, T.; Iyasere, O.; et al. Clinical Practice Guideline on management of older patients with chronic kidney disease stage 3b or higher (eGFR &alt; 45 mL/min/1.73 m2): A summary document from the European Renal Best Practice Group. Nephrol. Dial. Transplant. 2017, 32, 9–16. [Google Scholar]
- Martínez-Castelao, A.; Górriz, J.L.; Ortiz, A.; Navarro-González, J.F. ERBP guideline on management of patients with diabetes and chronic kidney disease stage 3B or higher. Metformin for all? Nefrologia 2017, 37, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Górriz, J.; Nieto, J.; Navarro-González, J.; Molina, P.; Martínez-Castelao, A.; Pallardó, L. Nephroprotection by Hypoglycemic Agents: Do We Have Supporting Data? J. Clin. Med. 2015, 4, 1866–1889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wanner, C.; Inzucchi, S.E.; Lachin, J.M.; Fitchett, D.; von Eynatten, M.; Mattheus, M.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Zinman, B.; et al. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scirica, B.M.; Bhatt, D.L.; Braunwald, E.; Steg, P.G.; Davidson, J.; Hirshberg, B.; Ohman, P.; Frederich, R.; Wiviott, S.D.; Hoffman, E.B.; et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N. Engl. J. Med. 2013, 369, 1317–1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- Mann, J.F.E.; Brown-Frandsen, K.; Marso, S.P.; Poulter, N.R.; Rasmussen, S.; Rsted, D.D. Committee and Investigators. Liraglutide and renal outcomes in type 2 diabetes. N. Engl. J. Med. 2017, 31, 839–848. [Google Scholar] [CrossRef] [Green Version]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef] [Green Version]
- Tuttle, K.R.; Lakshmanan, M.C.; Rayner, B.; Busch, R.S.; Zimmermann, A.G.; Woodward, D.B.; Botros, F.T. Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7): A multicentre, open-label, randomised trial. Lancet Diabetes Endocrinol. 2018, 6, 605–617. [Google Scholar] [CrossRef]
- Soriguer, F.; Goday, A.; Bosch-Comas, A.; Bordiú, E.; Calle-Pascual, A.; Carmena, R.; Casamitjana, R.; Castaño, L.; Castell, C.; Catalá, M.; et al. Prevalence of diabetes mellitus and impaired glucose regulation in Spain: The [email protected] Study. Diabetologia 2012, 55, 88–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morales, E.; Praga, M. The effect of weight loss in obesity and chronic kidney disease. Curr. Hypertens. Rep. 2012, 14, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Cuevas-Ramos, D.; Campos-Barrera, E.; Durán-Pérez, E.G.; Almeda-Valdés, P.; Muñoz-Hernández, L.; Gómez-Pérez, F.J. Treatment of metabolic syndrome slows progression of diabetic nephropathy. Metab. Syndr. Relat. Disord. 2011, 9, 483–489. [Google Scholar]
- Friedman, A.N.; Chambers, M.; Kamendulis, L.M.; Temmerman, J. Short-term changes after a weight reduction intervention in advanced diabetic nephropathy. Clin. J. Am. Soc. Nephrol. 2013, 8, 1892–1898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shulman, A.; Peltonen, M.; Sjöström, C.D.; Andersson-Assarsson, J.C.; Taube, M.; Sjöholm, K.; le Roux, C.W.; Carlsson, L.M.; Svensson, P.A. Incidence of end-stage renal disease following bariatric surgery in the Swedish Obese Subjects Study. Int. J. Obes. 2018, 42, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Gautier, J.-F.; Choukem, S.-P.; Girard, J. Physiology of incretins (GIP and GLP-1) and abnormalities in type 2 diabetes. Diabetes Metab. 2008, 34 (Suppl. 2), S65–S72. [Google Scholar] [CrossRef]
- Müller, T.D.; Finan, B.; Bloom, S.R.; D’Alessio, D.; Drucker, D.J.; Flatt, P.R.; Fritsche, A.; Gribble, F.; Grill, H.J.; Habener, J.F.; et al. Glucagon-like peptide 1 (GLP-1). Mol. Metab. 2019, 30, 72–130. [Google Scholar] [CrossRef]
- Skov, J. Effects of GLP-1 in the kidney. Rev. Endocr. Metab. Disord. 2014, 15, 197–207. [Google Scholar] [CrossRef]
- Muskiet, M.H.A.; Tonneijck, L.; Smits, M.M.; van Baar, M.J.B.; Kramer, M.H.H.; Hoorn, E.J.; Joles, J.A.; van Raalte, D.H. GLP-1 and the kidney: From physiology to pharmacology and outcomes in diabetes. Nat. Rev. Nephrol. 2017, 13, 605–628. [Google Scholar] [CrossRef]
- Heni, M.; Ketterer, C.; Thamer, C.; Herzberg-Schäfer, S.A.; Guthoff, M.; Stefan, N.; Machicao, F.; Staiger, H.; Fritsche, A.; Häring, H.-U. Glycemia determines the effect of type 2 diabetes risk genes on insulin secretion. Diabetes 2010, 59, 3247–3252. [Google Scholar] [CrossRef] [Green Version]
- Herzberg-Schäfer, S.; Heni, M.; Stefan, N.; Häring, H.-U.; Fritsche, A. Impairment of GLP1-induced insulin secretion: Role of genetic background, insulin resistance and hyperglycaemia. Diabetes Obes. Metab. 2012, 14 (Suppl. 3), 85–90. [Google Scholar] [CrossRef]
- Gorgojo-Martínez, J.J. New glucose-lowering drugs for reducing cardiovascular risk in patients with type2 diabetes mellitus. Hipertens. Riesgo Vasc. 2019, 36, 145–161. [Google Scholar] [CrossRef] [PubMed]
- Takayanagi, R.; Uchida, T.; Kimura, K.; Yamada, Y. Evaluation of Drug Efficacy of GLP-1 Receptor Agonists and DPP-4 Inhibitors Based on Target Molecular Binding Occupancy. Biol. Pharm. Bull. 2018, 41, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Lee, D.Y. Glucagon-like peptide-1 and glucagon-like peptide-1 receptor agonists in the treatment of type 2 diabetes. Ann. Pediatric Endocrinol. Metab. 2017, 22, 15–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marbury, T.C.; Flint, A.; Jacobsen, J.B.; Derving Karsbøl, J.; Lasseter, K. Pharmacokinetics and Tolerability of a Single Dose of Semaglutide, a Human Glucagon-Like Peptide-1 Analog, in Subjects with and without Renal Impairment. Clin. Pharmacokinet. 2017, 56, 1381–1390. [Google Scholar] [CrossRef] [Green Version]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Riesmeyer, J.S.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. Lancet 2019, 394, 121–130. [Google Scholar] [CrossRef]
- Nauck, M.A.; Meier, J.J.; Cavender, M.A.; el Aziz, M.A.; Drucker, D.J. Cardiovascular actions and clinical outcomes with glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors. Circulation 2017, 136, 849–870. [Google Scholar] [CrossRef]
- Thomas, M.C. The potential and pitfalls of GLP-1 receptor agonists for renal protection in type 2 diabetes. Diabetes Metab. 2017, 43 (Suppl. 1), S20–S27. [Google Scholar] [CrossRef]
- Greco, E.V.; Russo, G.; Giandalia, A.; Viazzi, F.; Pontremoli, R.; de Cosmo, S. GLP-1 Receptor Agonists and Kidney Protection. Medicina 2019, 55, 233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, A.; Guess, N.; Dornhorst, A.; Taheri, S.; Frost, G. Insulin-associated weight gain in obese type 2 diabetes mellitus patients: What can be done? Diabetes Obes. Metab. 2017, 19, 1655–1668. [Google Scholar] [CrossRef]
- Ramirez, G.; Morrison, A.; Bittle, P. Clinical practice considerations and review of the literature for the use of DPP-4 inhibitors in patients with type 2 diabetes and chronic kidney disease. Endocr. Pract. 2013, 19, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Scheen, A.J. Cardiovascular effects of new oral glucose-lowering agents DPP-4 and SGLT-2 inhibitors. Circ. Res. 2018, 122, 1439–1459. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Fernandez, B.; Fernandez-Prado, R.; Górriz, J.L.; Martinez-Castelao, A.; Navarro-González, J.F.; Porrini, E.; Soler, M.J.; Ortiz, A. Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation and Study of Diabetic Nephropathy with Atrasentan: What was learned about the treatment of diabetic kidney disease with canagliflozin and atrasentan? Clin. Kidney J. 2019, 12, 313–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarafidis, P.; Ferro, C.J.; Morales, E.; Ortiz, A.; Malyszko, J.; Hojs, R.; Khazim, K.; Ekart, R.; Valdivielso, J.; Fouque, D.; et al. SGLT-2 inhibitors and GLP-1 receptor agonists for nephroprotection and cardioprotection in patients with diabetes mellitus and chronic kidney disease. A consensus statement by the EURECA-m and the DIABESITY working groups of the ERA-EDTA. Nephrol. Dial. Transplant. 2019, 34, 208–230. [Google Scholar] [CrossRef] [PubMed]
- Kapitza, C.; Nosek, L.; Jensen, L.; Hartvig, H.; Jensen, C.B.; Flint, A. Semaglutide, a once-weekly human GLP-1 analog, does not reduce the bioavailability of the combined oral contraceptive, ethinylestradiol/levonorgestrel. J. Clin. Pharmacol. 2015, 55, 497–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosenzon, O.; Blicher, T.M.; Rosenlund, S.; Eriksson, J.W.; Heller, S.; Hels, O.H.; Pratley, R.; Sathyapalan, T.; Desouza, C.; PIONEER 5 Investigators. Efficacy and safety of oral semaglutide in patients with type 2 diabetes and moderate renal impairment (PIONEER 5): A placebo-controlled, randomised, phase 3a trial. Lancet Diabetes Endocrinol. 2019, 7, 515–527. [Google Scholar] [CrossRef] [Green Version]
- Idorn, T.; Knop, F.K.; Jørgensen, M.B.; Jensen, T.; Resuli, M.; Hansen, P.M.; Christensen, K.B.; Holst, J.J.; Hornum, M.; Feldt-Rasmussen, B. Safety and Efficacy of Liraglutide in Patients with Type 2 Diabetes and End-Stage Renal Disease: An Investigator-Initiated, Placebo-Controlled, Double-Blind, Parallel-Group, Randomized Trial. Diabetes Care 2016, 39, 206–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, M.J.; Bain, S.C.; Atkin, S.L.; Rossing, P.; Scott, D.; Shamkhalova, M.S.; Bosch-Traberg, H.; Syrén, A.; Umpierrez, G.E. Efficacy and Safety of Liraglutide Versus Placebo as Add-on to Glucose-Lowering Therapy in Patients With Type 2 Diabetes and Moderate Renal Impairment (LIRA-RENAL): A Randomized Clinical Trial. Diabetes Care 2015, 39, 222–230. [Google Scholar] [CrossRef] [Green Version]
- Pfeffer, M.A.; Claggett, B.; Diaz, R.; Dickstein, K.; Gerstein, H.C.; Køber, L.V.; Lawson, F.C.; Ping, L.; Wei, X.; Lewis, E.F.; et al. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N. Engl. J. Med. 2015, 373, 2247–2257. [Google Scholar] [CrossRef] [PubMed]
- Holman, R.R.; Bethel, M.A.; Mentz, R.J.; Thompson, V.P.; Lokhnygina, Y.; Buse, J.B.; Chan, J.C.N.; Choi, J.; Gustavson, S.M.; Iqbal, N.; et al. Effects of Once-Weekly Exenatide on Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez, A.F.; Green, J.B.; Janmohamed, S.; D’Agostino, R.B.; Granger, C.B.; Jones, N.P.; Leiter, L.A.; E Rosenberg, A.; Sigmon, K.N.; Somerville, M.C.; et al. Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes): A double-blind, randomised placebo-controlled trial. Lancet 2018, 392, 1519–1529. [Google Scholar] [CrossRef] [Green Version]
- Husain, M.; Birkenfeld, A.L.; Donsmark, M.; Dungan, K.; Eliaschewitz, F.G.; Franco, D.R.; Jeppesen, O.K.; Lingvay, I.; Mosenzon, O.; Pedersen, S.D.; et al. Oral Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2019, 381, 841–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cefalu, W.T.; Kaul, S.; Gerstein, H.; Holman, R.R.; Zinman, B.; Skyler, J.S.; Green, J.B.; Buse, J.B.; Inzucchi, S.E.; Leiter, L.A.; et al. Cardiovascular Outcomes Trials in Type 2 Diabetes: Where Do We Go From Here? Reflections From aDiabetes CareEditors’ Expert Forum. Diabetes Care 2017, 41, 14–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kristensen, S.L.; Rørth, R.; Jhund, P.S.; Docherty, K.F.; Sattar, N.; Preiss, D.; Køber, L.; Petrie, M.C.; McMurray, J.J.V. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: A systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol. 2019, 7, 776–785. [Google Scholar] [CrossRef]
- Muskiet, M.; Tonneijck, L.; Huang, Y.; Liu, M.; Saremi, A.; Heerspink, H.J.L.; Van Raalte, D.H. Lixisenatide and renal outcomes in patients with type 2 diabetes and acute coronary syndrome: An exploratory analysis of the ELIXA randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2018, 6, 859–869. [Google Scholar] [CrossRef]
- Bethel, M.A.; Mentz, R.J.; Merrill, P.; Buse, J.B.; Chan, J.C.N.; Goodman, S.G.; Iqbal, N.; Jakuboniene, N.; Katona, B.G.; Lokhnygina, Y.; et al. Renal Outcomes in the EXenatide Study of Cardiovascular Event Lowering (EXSCEL). Diabetes 2018, 67, 522. [Google Scholar] [CrossRef]
- Perkovic, V.; Koitka-Weber, A.; E Cooper, M.; Schernthaner, G.; Pfarr, E.; Woerle, H.J.; Von Eynatten, M.; Wanner, C. Choice of endpoint in kidney outcome trials: Considerations from the EMPA-REG OUTCOME® trial. Nephrol. Dial. Transplant. 2019. [Google Scholar] [CrossRef]
- Perkovic, V.; Bain, S.; Bakris, G.; Buse, J.; Gondolf, T. eGFR loss with glucagon-like peptide-1 (GLP-1) analogue treatment: Data from SUSTAIN 6 and LEADER. In Proceedings of the 56th ERAEDTA Congress, Budapest, Hungary, 13–16 June 2019; pp. 13–16. [Google Scholar]
- Pyke, C.; Heller, R.S.; Kirk, R.K.; Ørskov, C.; Reedtz-Runge, S.; Kaastrup, P.; Hvelplund, A.; Bardram, L.; Calatayud, D.; Knudsen, L.B. GLP-1 Receptor Localization in Monkey and Human Tissue: Novel Distribution Revealed With Extensively Validated Monoclonal Antibody. Endocrinol. 2014, 155, 1280–1290. [Google Scholar] [CrossRef]
- Pyke, C.; Knudsen, L.B. The glucagon-like peptide-1 receptor-or not? Endocrinology 2013, 154, 4–8. [Google Scholar] [CrossRef] [Green Version]
- Tsimihodimos, V.; Elisaf, M. Effects of incretin-based therapies on renal function. Eur. J. Pharmacol. 2018, 818, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Katout, M.; Rutsky, J.; Shah, P.; Zhu, H.; Brook, R.D.; Zhong, J.; Rajagopalan, S. Effect of GLP-1 Mimetics on Blood Pressure and Relationship to Weight Loss and Glycemia Lowering: Results of a Systematic Meta-Analysis and Meta-Regression. Am. J. Hypertens. 2013, 27, 130–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Li, P.; Tang, Z.; Yan, X.; Feng, B. Structural modulation of the gut microbiota and the relationship with body weight: Compared evaluation of liraglutide and saxagliptin treatment. Sci. Rep. 2016, 6, 33251. [Google Scholar] [CrossRef] [PubMed]
- Gutzwiller, J.-P.; Tschopp, S.; Bock, A.; Zehnder, C.E.; Huber, A.R.; Kreyenbuehl, M.; Gutmann, H.; Drewe, J.; Henzen, C.; Goeke, B.; et al. Glucagon-Like Peptide 1 Induces Natriuresis in Healthy Subjects and in Insulin-Resistant Obese Men. J. Clin. Endocrinol. Metab. 2004, 89, 3055–3061. [Google Scholar] [CrossRef] [PubMed]
- Sloan, L.A. Review of glucagon-like peptide-1 receptor agonists for the treatment of type 2 diabetes mellitus in patients with chronic kidney disease and their renal effects. J. Diabetes 2019, 11, 938–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, S.C.; Kashkouli, A.; Singh, P. Glucagon-like peptide-1 receptor stimulation increases GFR and suppresses proximal reabsorption in the rat. Am. J. Physiol. Ren. Physiol. 2013, 304, F137–F144. [Google Scholar] [CrossRef] [Green Version]
- Tonneijck, L.; Smits, M.M.; Muskiet, M.; Hoekstra, T.; Kramer, M.H.H.; Danser, A.H.J.; Diamant, M.; Joles, J.A.; Van Raalte, D.H. Acute renal effects of the GLP-1 receptor agonist exenatide in overweight type 2 diabetes patients: A randomised, double-blind, placebo-controlled trial. Diabetol. 2016, 59, 1412–1421. [Google Scholar] [CrossRef] [Green Version]
- Yin, W.-Q.; Xu, S.; Wang, Z.; Liu, H.; Peng, L.; Fang, Q.; Deng, T.; Zhang, W.; Lou, J. Recombinant human GLP-1(rhGLP-1) alleviating renal tubulointestitial injury in diabetic STZ-induced rats. Biochem. Biophys. Res. Commun. 2018, 495, 793–800. [Google Scholar] [CrossRef]
- Study, F. Study to See How Semaglutide Works Compared to Placebo in People with Type 2 Diabetes and Chronic Kidney Disease (FLOW). ClinicalTrials.gov Identifier: NCT0383. 1915. Available online: https://clinicaltrials.gov/ct2/show/NCT0383 (accessed on 28 March 2020).




{kind=link}
{kind=link}
{kind=link}
| Risk Factor | Susceptibility | Initiation | Progression |
|---|---|---|---|
| Demographic | |||
| Older age | + | ||
| Sex (men) | + | ||
| Race (black, other ethnic minorities) | + | + | |
| Reduced renal mass | + | + | |
| Low birth weight | + | ||
| Low socioeconomic level | + | + | |
| Hereditary | |||
| Family history of DKD | + | ||
| Genetic kidney disease | + | ||
| Systemic conditions | |||
| Hyperglycemia (poorly controlled) | + | + | + |
| Obesity | + | + | + |
| Hypertension (poorly controlled) | + | + | |
| Kidney injuries | |||
| Acute kidney injury | + | + | |
| Toxins, nephrotoxic drugs, mainly NSAIDs | + | + | |
| Smoking | + | ||
| Urological problems (infection, obstruction) | + | + | |
| Dietary factors | |||
| High protein intake | + | + |
| Drug (Ref) | Trial | n | Studied Population | Mean Duration | Composite Primary CV Endpoint | Result HR (95% CI; p) | Individual Primary CV Endpoint | Result HR (95% CI; p) |
|---|---|---|---|---|---|---|---|---|
| Lixisenatide [45] | ELIXA | 6068 | T2D and acute coronary syndrome | 25 m | 3P-MACE | Neutral | None | Neutral |
| Exenatide [46] | EXSCEL | 14,752 | T2D with or without CVD | 3.2 y | 3P-MACE | Neutral | None | Neutral |
| Liraglutide [19,47] | LEADER | 9340 | T2D and high CV risk | 3.8 y | 3P-MACE | 0.87 (0.78–0.97; p < 0.001) | Death from any cause | 0.85 (0.74–0.97; p = 0.02) |
| Semaglutide [20] (sc) | SUSTAIN-6 | 3297 | T2D 50 y or more with established CVD, CHF or CKD G3 or higher or >60 y w/CV risk factor | 2.1 y | 3P-MACE | 0.74 (0.58–0.95; p = 0.02) | Nonfatal stroke | 0.61 (0.38–0.99; p = 0.04) |
| Albiglutide [48] | HARMONY | 9469 | T2D and CVD or CV risk factors | 3.8 y | 3P-MACE | 0.78 (0.68–0.90; p = 0.0006) | Fatal or nonfatal myocardial infarction | 0.75 (0.61–0.90, p = 0.003) |
| Dulaglutide [28] | REWIND | 9901 | T2D and CVD or CV risk factors | 5.4 y | 3P-MACE | 0.88 (0.79–0.99; p = 0.026) | Nonfatal Stroke | 0.76 (0.61–0.95; p = 0.017) |
| Semaglutide [49] (oral) | PIONEER-6 | 3183 | T2D and CVD or CV risk factors | 15.9 m | 3P-MACE | Neutral | None | Neutral |
| Exenatide [22] | FREEDOM-CVO | 4000 | T2D and CV disease | UK | UK | UK | UK | UK |
| Drugs | Trials | % n eGFR < 60 | Composite Kidney Endpoint | Results | Individual Kidney Endpoint | Result HR (95% CI; p) |
|---|---|---|---|---|---|---|
| Lixisenatide [45] | ELIXA | 23 | NA | NA | New onset macroalbuminuria | 0.808 (0.660–0.991; p = 0.0404) |
| Exenatide [46] | EXSCEL | 17 | 40% reduction in eGFR loss, onset of dialysis or transplantation, renal death and onset of macroalbuminuria | 0.85 (0.73–0.98; p = 0.027) | None | Neutral |
| Liraglutide [19,47] | LEADER | 23 | New onset macroalbuminuria, sustained serum creatinine duplication, initiation of renal replacement therapy or renal death | 0.78 (0.67–0.92; p = 0.003) | New onset macroalbuminuria | 0.74 (0.37–0.77; p = 0.001) |
| Semaglutide [20] (sc) | SUSTAIN-6 | 28.5 | New onset macroalbuminuria, doubling serum creatinine reaching an eGFR <45 mL/min/1.73 m2, initiation of renal replacement therapy or renal death | 0.64 (0.46–0.88; p = 0.005) | Persistent macroalbuminuria | 0.54 (0.60–0.91; p = 0.004) |
| Albiglutide [48] | HARMONY | 11 | UK | UK | UK | UK |
| Dulaglutide [28] | REWIND | 22 | New onset macroalbuminuria, sustained decreased of eGFR <30% or the initiation of renal replacement therapy | 0.85 (0.77–0.93, p = 0.0004) | New onset macroalbuminuria; Sustained decline in eGFR of ≥40%; Sustained decline in eGFR of ≥50% | 0.77 (0.68–0.87; p < 0.0001); 0.70 (0.57–0.85; p = 0.0004); 0.74 (0.66–0.84; p < 0.0001) |
| Semaglutide [49] (oral) | PIONEER-6 | 27 | UK | UK | UK | UK |
| Exenatide [22] | FREEDOM-CVO | UK | UK | UK | UK | UK |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Górriz, J.L.; Soler, M.J.; Navarro-González, J.F.; García-Carro, C.; Puchades, M.J.; D’Marco, L.; Martínez Castelao, A.; Fernández-Fernández, B.; Ortiz, A.; Górriz-Zambrano, C.; et al. GLP-1 Receptor Agonists and Diabetic Kidney Disease: A Call of Attention to Nephrologists. J. Clin. Med. 2020, 9, 947. https://doi.org/10.3390/jcm9040947
Górriz JL, Soler MJ, Navarro-González JF, García-Carro C, Puchades MJ, D’Marco L, Martínez Castelao A, Fernández-Fernández B, Ortiz A, Górriz-Zambrano C, et al. GLP-1 Receptor Agonists and Diabetic Kidney Disease: A Call of Attention to Nephrologists. Journal of Clinical Medicine. 2020; 9(4):947. https://doi.org/10.3390/jcm9040947
Chicago/Turabian StyleGórriz, José Luis, María José Soler, Juan F. Navarro-González, Clara García-Carro, María Jesús Puchades, Luis D’Marco, Alberto Martínez Castelao, Beatriz Fernández-Fernández, Alberto Ortiz, Carmen Górriz-Zambrano, and et al. 2020. "GLP-1 Receptor Agonists and Diabetic Kidney Disease: A Call of Attention to Nephrologists" Journal of Clinical Medicine 9, no. 4: 947. https://doi.org/10.3390/jcm9040947