The Role of Periodontitis and Periodontal Bacteria in the Onset and Progression of Alzheimer’s Disease: A Systematic Review

 , , ,
, , , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
- To include all those studies describing the association between Alzheimer’s disease and periodontal disease.
- To include all articles describing the role of bacteria such as Porphyromonas gingivalis, Aggregatibacter actinomycetemcomitans, Fusobacterium nucleatum and Treponema denticola in the onset and progression of the Alzheimer’s disease.
- To exclude all studies that were not written in English and were published before 1990.
- To exclude non-systematic literature reviews.
2.2. Research Methodology
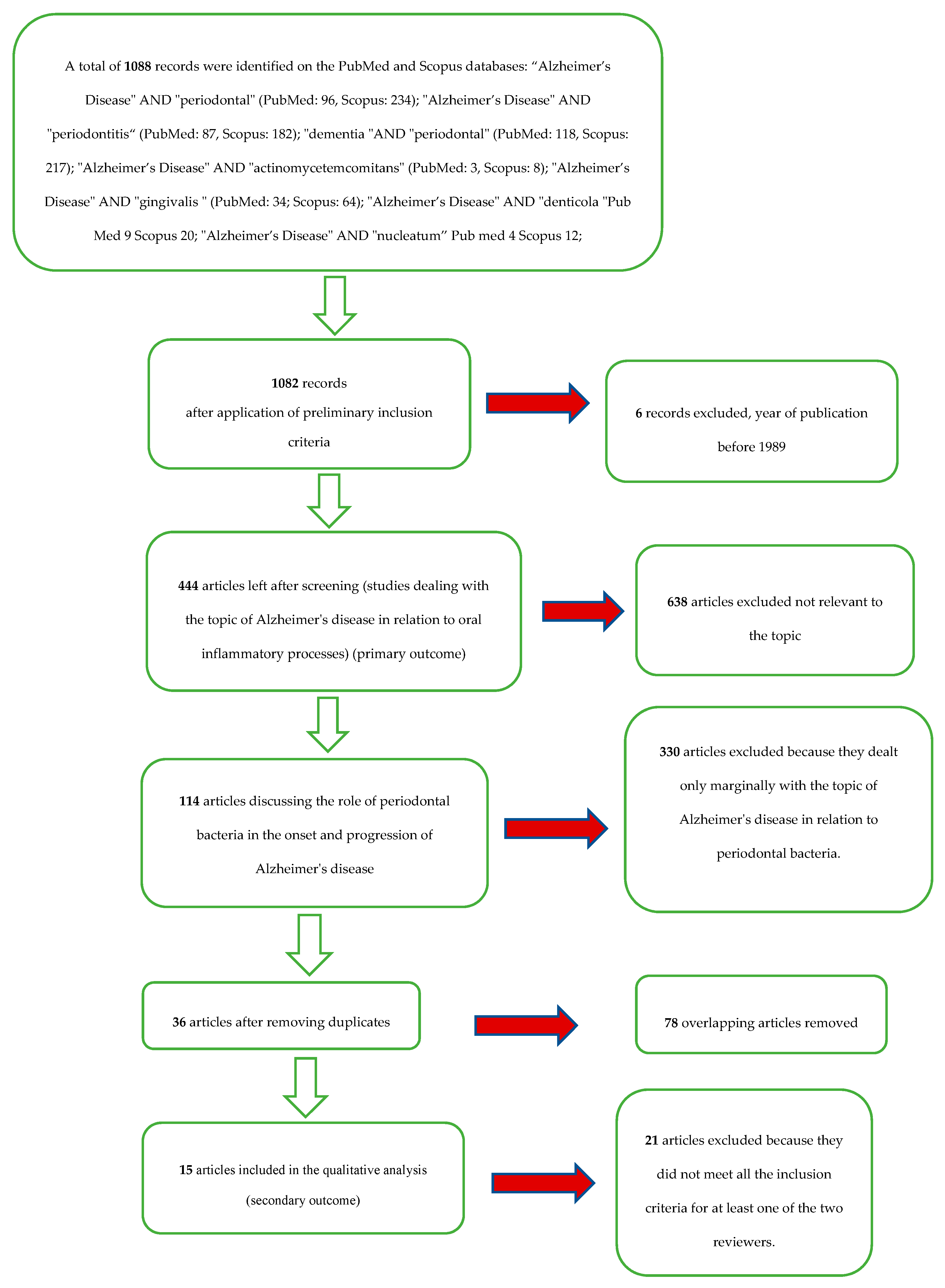
2.3. Screening Methodology
- (1)
- Primary outcome: associations between periodontitis and Alzheimer’s disease.
- (2)
- Secondary outcome: associations between bacteria involved in the pathogenesis of periodontal disease and Alzheimer’s disease.
3. Results
Study Characteristics and Data Extraction
- First outcome: The articles included for the first outcome (associations between periodontitis and Alzheimer’s disease) after the elimination of overlaps were about a hundred. The articles were then studied to deepen and update the reviewers’ knowledge on the subject of the association between Alzheimer’s disease and periodontitis. Articles were used to draft the discussion on the correlations between the two diseases and their respective etiopathogenesis.
- Second outcome: the articles included for the second outcome (associations between bacteria involved in the pathogenesis of periodontal disease and Alzheimer’s disease) were Wu et al. 2017 [9], Hayashi et al. 2019 [10], Poole et al. 2013 [11], Carter et al. 2017 [12], Liu et al. 2017 [13], Laugish et al. 2018 [14], Ide et al. 2016 [15], Ishida et al. 2017 [16], Dominy et al. 2019 [17], Nie et al. 2019 [18], Diaz-Zuniga et al. 2019 [6], Sparks Stein et al. 2012 [19], Noble et al. 2014 [20], Carter et al. 2017 [21], and Kamer et al. 2009 [22].
4. Discussion
4.1. Periodontal disease
4.2. Alzheimer’s disease
4.3. Inflammatory Theory
4.4. Associative Hypotheses between Periodontitis and Neurodegenerative Diseases: Aspects in Common
4.5. Analysis of the Evidence on the Role of P. gingivalis on the Etiopathogenesis of A.D.
4.6. Health and Oral Hygiene in Patients with Alzheimer’s Disease
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lane, C.A.; Hardy, J.; Schott, J.M. Alzheimer’s disease. Eur. J. Neurol. 2018, 25, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Dye, B.A. Global periodontal disease epidemiology. Periodontology 2000 2012, 58, 10–25. [Google Scholar] [CrossRef] [PubMed]
- Singhrao, S.K.; Harding, A.; Simmons, T.; Robinson, S.; Kesavalu, L.; Crean, S. Oral inflammation, tooth loss, risk factors, and association with progression of Alzheimer’s disease. J. Alzheimers Dis. 2014, 42, 723–737. [Google Scholar] [CrossRef] [Green Version]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [Google Scholar] [CrossRef]
- Holmer, J.; Eriksdotter, M.; Schultzberg, M.; Pussinen, P.J.; Buhlin, K. Association between periodontitis and risk of Alzheimer’s disease, mild cognitive impairment and subjective cognitive decline: A case-control study. J. Clin. Periodontol. 2018, 45, 1287–1298. [Google Scholar] [CrossRef]
- Diaz-Zuniga, J.; Munoz, Y.; Melgar-Rodriguez, S.; More, J.; Bruna, B.; Lobos, P.; Monasterio, G.; Vernal, R.; Paula-Lima, A. Serotype b of Aggregatibacter actinomycetemcomitans triggers pro-inflammatory responses and amyloid beta secretion in hippocampal cells: A novel link between periodontitis and Alzheimer s disease? J. Oral Microbiol. 2019, 11, 1586423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganesh, P.; Karthikeyan, R.; Muthukumaraswamy, A.; Anand, J. A Potential Role of Periodontal Inflammation in Alzheimer’s Disease: A Review. Oral Health Prev. Dent. 2017, 15, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S.; Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Chichester, UK; Hoboken, NJ, USA, 2008; pp. xxi, 649. [Google Scholar]
- Wu, Z.; Ni, J.; Liu, Y.; Teeling, J.L.; Takayama, F.; Collcutt, A.; Ibbett, P.; Nakanishi, H. Cathepsin B plays a critical role in inducing Alzheimer’s disease-like phenotypes following chronic systemic exposure to lipopolysaccharide from Porphyromonas gingivalis in mice. Brain Behav. Immun. 2017, 65, 350–361. [Google Scholar] [CrossRef]
- Hayashi, K.; Hasegawa, Y.; Takemoto, Y.; Cao, C.; Takeya, H.; Komohara, Y.; Mukasa, A.; Kim-Mitsuyama, S. Continuous intracerebroventricular injection of Porphyromonas gingivalis lipopolysaccharide induces systemic organ dysfunction in a mouse model of Alzheimer’s disease. Exp. Gerontol. 2019, 120, 1–5. [Google Scholar] [CrossRef]
- Poole, S.; Singhrao, S.K.; Kesavalu, L.; Curtis, M.A.; Crean, S. Determining the presence of periodontopathic virulence factors in short-term postmortem Alzheimer’s disease brain tissue. J. Alzheimers Dis. 2013, 36, 665–677. [Google Scholar] [CrossRef]
- Carter, C.J. Genetic, Transcriptome, Proteomic, and Epidemiological Evidence for Blood-Brain Barrier Disruption and Polymicrobial Brain Invasion as Determinant Factors in Alzheimer’s Disease. J. Alzheimer’s Dis. Rep. 2017, 1, 125–157. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wu, Z.; Nakanishi, Y.; Ni, J.; Hayashi, Y.; Takayama, F.; Zhou, Y.; Kadowaki, T.; Nakanishi, H. Infection of microglia with Porphyromonas gingivalis promotes cell migration and an inflammatory response through the gingipain-mediated activation of protease-activated receptor-2 in mice. Sci. Rep. 2017, 7, 11759. [Google Scholar] [CrossRef] [PubMed]
- Laugisch, O.; Johnen, A.; Maldonado, A.; Ehmke, B.; Burgin, W.; Olsen, I.; Potempa, J.; Sculean, A.; Duning, T.; Eick, S. Periodontal Pathogens and Associated Intrathecal Antibodies in Early Stages of Alzheimer’s Disease. J. Alzheimers Dis. 2018, 66, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Ide, M.; Harris, M.; Stevens, A.; Sussams, R.; Hopkins, V.; Culliford, D.; Fuller, J.; Ibbett, P.; Raybould, R.; Thomas, R.; et al. Periodontitis and Cognitive Decline in Alzheimer’s Disease. PLoS ONE 2016, 11, e0151081. [Google Scholar] [CrossRef] [Green Version]
- Ishida, N.; Ishihara, Y.; Ishida, K.; Tada, H.; Funaki-Kato, Y.; Hagiwara, M.; Ferdous, T.; Abdullah, M.; Mitani, A.; Michikawa, M.; et al. Periodontitis induced by bacterial infection exacerbates features of Alzheimer’s disease in transgenic mice. NPJ Aging Mech. Dis. 2017, 3, 15. [Google Scholar] [CrossRef] [Green Version]
- Dominy, S.S.; Lynch, C.; Ermini, F.; Benedyk, M.; Marczyk, A.; Konradi, A.; Nguyen, M.; Haditsch, U.; Raha, D.; Griffin, C.; et al. Porphyromonas gingivalis in Alzheimer’s disease brains: Evidence for disease causation and treatment with small-molecule inhibitors. Sci. Adv. 2019, 5, eaau3333. [Google Scholar] [CrossRef] [Green Version]
- Nie, R.; Wu, Z.; Ni, J.; Zeng, F.; Yu, W.; Zhang, Y.; Kadowaki, T.; Kashiwazaki, H.; Teeling, J.L.; Zhou, Y. Porphyromonas gingivalis Infection Induces Amyloid-beta Accumulation in Monocytes/Macrophages. J. Alzheimers Dis. 2019, 72 (Suppl. 4), 4–16. [Google Scholar] [CrossRef]
- Sparks Stein, P.; Steffen, M.J.; Smith, C.; Jicha, G.; Ebersole, J.L.; Abner, E.; Dawson, D., 3rd. Serum antibodies to periodontal pathogens are a risk factor for Alzheimer’s disease. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2012, 8, 196–203. [Google Scholar] [CrossRef] [Green Version]
- Noble, J.M.; Scarmeas, N.; Celenti, R.S.; Elkind, M.S.; Wright, C.B.; Schupf, N.; Papapanou, P.N. Serum IgG antibody levels to periodontal microbiota are associated with incident Alzheimer disease. PLoS ONE 2014, 9, e114959. [Google Scholar] [CrossRef] [Green Version]
- Carter, C.J.; France, J.; Crean, S.; Singhrao, S.K. The Porphyromonas gingivalis/Host Interactome Shows Enrichment in GWASdb Genes Related to Alzheimer’s Disease, Diabetes and Cardiovascular Diseases. Front. Aging Neurosci. 2017, 9, 408. [Google Scholar] [CrossRef] [Green Version]
- Kamer, A.R.; Craig, R.G.; Pirraglia, E.; Dasanayake, A.P.; Norman, R.G.; Boylan, R.J.; Nehorayoff, A.; Glodzik, L.; Brys, M.; de Leon, M.J. TNF-alpha and antibodies to periodontal bacteria discriminate between Alzheimer’s disease patients and normal subjects. J. Neuroimmunol. 2009, 216, 92–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonsekar, P.P.; Jiang, S.S.; Yue, G. Periodontal disease, tooth loss and dementia: Is there a link? A systematic review. Gerodontology 2017, 34, 151–163. [Google Scholar] [CrossRef] [PubMed]
- Socransky, S.S.; Haffajee, A.D. Dental biofilms: Difficult therapeutic targets. Periodontology 2000 2002, 28, 12–55. [Google Scholar] [CrossRef] [PubMed]
- Paster, B.J.; Olsen, I.; Aas, J.A.; Dewhirst, F.E. The breadth of bacterial diversity in the human periodontal pocket and other oral sites. Periodontology 2000 2006, 42, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Zhurakivska, K.; Troiano, G.; Caponio, V.C.A.; Dioguardi, M.; Laino, L.; Maffione, A.B.; Lo Muzio, L. Do Changes in Oral Microbiota Correlate With Plasma Nitrite Response? A Systematic Review. Front. Physiol. 2019, 10, 1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez Leo, E.E.; Segura Campos, M.R. Effect of ultra-processed diet on gut microbiota and thus its role in neurodegenerative diseases. Nutrition 2019, 71, 110609. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D. The nature of periodontal diseases. Ann. Periodontol. 1997, 2, 3–10. [Google Scholar] [CrossRef]
- Troiano, G.; Laino, L.; Dioguardi, M.; Giannatempo, G.; Lo Muzio, L.; Lo Russo, L. Mandibular Class II Furcation Defect Treatment: Effects of the Addition of Platelet Concentrates to Open Flap: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. J. Periodontol. 2016, 87, 1030–1038. [Google Scholar] [CrossRef]
- Haerian, A.; Adonogianaki, E.; Mooney, J.; Docherty, J.P.; Kinane, D.F. Gingival crevicular stromelysin, collagenase and tissue inhibitor of metalloproteinases levels in healthy and diseased sites. J. Clin. Periodontol. 1995, 22, 505–509. [Google Scholar] [CrossRef]
- Berglundh, T.; Donati, M. Aspects of adaptive host response in periodontitis. J. Clin. Periodontol. 2005, 32 (Suppl. 6), 87–107. [Google Scholar] [CrossRef]
- Troiano, G.; Dioguardi, M.; Giannatempo, G.; Laino, L.; Testa, N.F.; Cocchi, R.; De Lillo, A.; Lo Muzio, L. Orofacial granulomatosis: Clinical signs of different pathologies. Med. Princ. Pract. Int. J. Kuwait Univ. Health Sci. Cent. 2015, 24, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Dioguardi, M.; Caloro, G.A.; Troiano, G.; Giannatempo, G.; Laino, L.; Petruzzi, M.; Lo Muzio, L. Oral manifestations in chronic uremia patients. Ren. Fail. 2016, 38, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troiano, G.; Dioguardi, M.; Limongelli, L.; Tempesta, A.; Favia, G.; Giuliani, M.; Sanguedolce, F.; Lo Muzio, L. Can Inspection of the Mouth Help Clinicians Diagnose Crohn’s Disease? A Review. Oral Health Prev. Dent. 2017, 15, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Wang, X.; Geng, M. Alzheimer’s disease hypothesis and related therapies. Transl. Neurodegener. 2018, 7, 2. [Google Scholar] [CrossRef] [Green Version]
- Bertogliat, M.J.; Morris-Blanco, K.C.; Vemuganti, R. Epigenetic mechanisms of neurodegenerative diseases and acute brain injury. Neurochem. Int. 2019, 104642. [Google Scholar] [CrossRef]
- Hampel, H.; Vergallo, A.; Perry, G.; Lista, S.; Alzheimer Precision Medicine, I. The Alzheimer Precision Medicine Initiative. J. Alzheimer’s Dis. JAD 2019, 68, 1–24. [Google Scholar] [CrossRef]
- Monfort, J.C. A population-based study of dementia in 85-year-olds. N. Engl. J. Med. 1993, 329, 63–64. [Google Scholar]
- van der Kant, R.; Goldstein, L.S.B.; Ossenkoppele, R. Amyloid-beta-independent regulators of tau pathology in Alzheimer disease. Nat. Rev. Neurosci. 2020, 21, 21–35. [Google Scholar] [CrossRef]
- Zhou, R.; Yang, G.; Shi, Y. Macromolecular complex in recognition and proteolysis of amyloid precursor protein in Alzheimer’s disease. Curr. Opin. Struct. Biol. 2019, 61, 1–8. [Google Scholar] [CrossRef]
- Lopez Sanchez, M.I.G.; van Wijngaarden, P.; Trounce, I.A. Amyloid precursor protein-mediated mitochondrial regulation and Alzheimer’s disease. Br. J. Pharmacol. 2019, 176, 3464–3474. [Google Scholar] [CrossRef]
- Hunter, S.; Brayne, C. Understanding the roles of mutations in the amyloid precursor protein in Alzheimer disease. Mol. Psychiatr. 2018, 23, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Bi, C.; Bi, S.; Li, B. Processing of Mutant beta-Amyloid Precursor Protein and the Clinicopathological Features of Familial Alzheimer’s Disease. Aging Dis. 2019, 10, 383–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, G.J.; Drego, R.; Hakimian, E.; Masliah, E. Mechanisms of cell signaling and inflammation in Alzheimer’s disease. Curr. Drug Targets Inflamm. Allergy 2005, 4, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Johnson-Wood, K.; Lee, M.; Motter, R.; Hu, K.; Gordon, G.; Barbour, R.; Khan, K.; Gordon, M.; Tan, H.; Games, D.; et al. Amyloid precursor protein processing and A beta42 deposition in a transgenic mouse model of Alzheimer disease. Proc. Natl. Acad. Sci. USA 1997, 94, 1550–1555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klegeris, A.; Walker, D.G.; McGeer, P.L. Interaction of Alzheimer beta-amyloid peptide with the human monocytic cell line THP-1 results in a protein kinase C-dependent secretion of tumor necrosis factor-alpha. Brain Res. 1997, 747, 114–121. [Google Scholar] [CrossRef]
- Wang, W.Y.; Tan, M.S.; Yu, J.T.; Tan, L. Role of pro-inflammatory cytokines released from microglia in Alzheimer’s disease. Ann. Transl. Med. 2015, 3, 136. [Google Scholar] [CrossRef]
- Li, Q.X.; Fuller, S.J.; Beyreuther, K.; Masters, C.L. The amyloid precursor protein of Alzheimer disease in human brain and blood. J. Leukoc. Biol. 1999, 66, 567–574. [Google Scholar] [CrossRef] [Green Version]
- Baune, B.T.; Ponath, G.; Rothermundt, M.; Riess, O.; Funke, H.; Berger, K. Association between genetic variants of IL-1beta, IL-6 and TNF-alpha cytokines and cognitive performance in the elderly general population of the MEMO-study. Psychoneuroendocrinology 2008, 33, 68–76. [Google Scholar] [CrossRef]
- Holmes, C. Review: Systemic inflammation and Alzheimer’s disease. Neuropathol. Appl. Neurobiol. 2013, 39, 51–68. [Google Scholar] [CrossRef]
- Kisby, B.; Jarrell, J.T.; Agar, M.E.; Cohen, D.S.; Rosin, E.R.; Cahill, C.M.; Rogers, J.T.; Huang, X. Alzheimer’s Disease and Its Potential Alternative Therapeutics. J. Alzheimers Dis. Parkinsonism 2019, 9. [Google Scholar] [CrossRef]
- de Jong, D.; Jansen, R.; Hoefnagels, W.; Jellesma-Eggenkamp, M.; Verbeek, M.; Borm, G.; Kremer, B. No effect of one-year treatment with indomethacin on Alzheimer’s disease progression: A randomized controlled trial. PLoS ONE 2008, 3, e1475. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.L.; Guan, P.P.; Liang, Y.Y.; Huang, X.S.; Wang, P. Cyclooxygenase-2 is Essential for Mediating the Effects of Calcium Ions on Stimulating Phosphorylation of Tau at the Sites of Ser 396 and Ser 404. J. Alzheimer’s Dis. JAD 2019, 68, 1095–1111. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Guan, P.P.; Yu, X.; Guo, Y.S.; Zhang, Y.J.; Wang, Z.Y.; Wang, P. COX-2 metabolic products, the prostaglandin I2 and F2alpha, mediate the effects of TNF-alpha and Zn(2+) in stimulating the phosphorylation of Tau. Oncotarget 2017, 8, 99296–99311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mrak, R.E.; Griffin, W.S. Interleukin-1 and the immunogenetics of Alzheimer disease. J. Neuropathol. Exp. Neurol. 2000, 59, 471–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corder, E.H.; Saunders, A.M.; Strittmatter, W.J.; Schmechel, D.E.; Gaskell, P.C.; Small, G.W.; Roses, A.D.; Haines, J.L.; Pericak-Vance, M.A. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science 1993, 261, 921–923. [Google Scholar] [CrossRef] [PubMed]
- Banks, W.A. Blood-brain barrier transport of cytokines: A mechanism for neuropathology. Curr. Pharm. Des. 2005, 11, 973–984. [Google Scholar] [CrossRef] [PubMed]
- Al-Obaidi, M.M.J.; Desa, M.N.M. Mechanisms of Blood Brain Barrier Disruption by Different Types of Bacteria, and Bacterial-Host Interactions Facilitate the Bacterial Pathogen Invading the Brain. Cell. Mol. Neurobiol. 2018, 38, 1349–1368. [Google Scholar] [CrossRef]
- Blatteis, C.M.; Sehic, E.; Li, S. Pyrogen sensing and signaling: Old views and new concepts. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2000, 31 (Suppl. 5), S168–S177. [Google Scholar] [CrossRef]
- Konsman, J.P.; Drukarch, B.; Van Dam, A.M. (Peri)vascular production and action of pro-inflammatory cytokines in brain pathology. Clin. Sci. 2007, 112, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Bradl, M.; Bauer, J.; Flugel, A.; Wekerle, H.; Lassmann, H. Complementary contribution of CD4 and CD8 T lymphocytes to T-cell infiltration of the intact and the degenerative spinal cord. Am. J. Pathol. 2005, 166, 1441–1450. [Google Scholar] [CrossRef] [Green Version]
- Dantzer, R.; Konsman, J.P.; Bluthe, R.M.; Kelley, K.W. Neural and humoral pathways of communication from the immune system to the brain: Parallel or convergent? Auton. Neurosci. 2000, 85, 60–65. [Google Scholar] [CrossRef]
- Kamer, A.R.; Pirraglia, E.; Tsui, W.; Rusinek, H.; Vallabhajosula, S.; Mosconi, L.; Yi, L.; McHugh, P.; Craig, R.G.; Svetcov, S.; et al. Periodontal disease associates with higher brain amyloid load in normal elderly. Neurobiol. Aging 2015, 36, 627–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gil-Montoya, J.A.; Barrios, R.; Santana, S.; Sanchez-Lara, I.; Pardo, C.C.; Fornieles-Rubio, F.; Montes, J.; Ramirez, C.; Gonzalez-Moles, M.A.; Burgos, J.S. Association Between Periodontitis and Amyloid beta Peptide in Elderly People With and Without Cognitive Impairment. J. Periodontol. 2017, 88, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Itzhaki, R.F.; Wozniak, M.A. Alzheimer’s disease and infection: Do infectious agents contribute to progression of Alzheimer’s disease? Alzheimers Dement. 2010, 6, 83–84. [Google Scholar] [CrossRef]
- Sochocka, M.; Zwolinska, K.; Leszek, J. The Infectious Etiology of Alzheimer’s Disease. Curr. Neuropharmacol. 2017, 15, 996–1009. [Google Scholar] [CrossRef] [Green Version]
- Kamer, A.R.; Craig, R.G.; Dasanayake, A.P.; Brys, M.; Glodzik-Sobanska, L.; de Leon, M.J. Inflammation and Alzheimer’s disease: Possible role of periodontal diseases. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2008, 4, 242–250. [Google Scholar] [CrossRef]
- Kamer, A.R.; Dasanayake, A.P.; Craig, R.G.; Glodzik-Sobanska, L.; Bry, M.; de Leon, M.J. Alzheimer’s disease and peripheral infections: The possible contribution from periodontal infections, model and hypothesis. J. Alzheimer’s Dis. JAD 2008, 13, 437–449. [Google Scholar] [CrossRef] [Green Version]
- Kempuraj, D.; Thangavel, R.; Natteru, P.A.; Selvakumar, G.P.; Saeed, D.; Zahoor, H.; Zaheer, S.; Iyer, S.S.; Zaheer, A. Neuroinflammation Induces Neurodegeneration. J. Neurol. Neurosurg. Spine 2016, 1, 1003. [Google Scholar]
- Watts, A.; Crimmins, E.M.; Gatz, M. Inflammation as a potential mediator for the association between periodontal disease and Alzheimer’s disease. Neuropsychiatr. Dis. Treat. 2008, 4, 865–876. [Google Scholar] [CrossRef] [Green Version]
- Singhrao, S.K.; Harding, A.; Poole, S.; Kesavalu, L.; Crean, S. Porphyromonas gingivalis Periodontal Infection and Its Putative Links with Alzheimer’s Disease. Med. Inflamm. 2015, 2015, 137357. [Google Scholar] [CrossRef] [Green Version]
- Offenbacher, S.; Riche, E.L.; Barros, S.P.; Bobetsis, Y.A.; Lin, D.; Beck, J.D. Effects of Maternal Campylobacter rectus Infection on Murine Placenta, Fetal and Neonatal Survival, and Brain Development. J. Periodontol. 2005, 76 (Suppl. 11S), 2133–2143. [Google Scholar] [CrossRef] [PubMed]
- Belkhelfa, M.; Rafa, H.; Medjeber, O.; Arroul-Lammali, A.; Behairi, N.; Abada-Bendib, M.; Makrelouf, M.; Belarbi, S.; Masmoudi, A.N.; Tazir, M.; et al. IFN-gamma and TNF-alpha are involved during Alzheimer disease progression and correlate with nitric oxide production: A study in Algerian patients. J. Interferon Cytokine Res. 2014, 34, 839–847. [Google Scholar] [CrossRef] [PubMed]
- Riviere, G.R.; Riviere, K.H.; Smith, K.S. Molecular and immunological evidence of oral Treponema in the human brain and their association with Alzheimer’s disease. Oral Microbiol. Immunol. 2002, 17, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Dioguardi, M.; Gioia, G.D.; Caloro, G.A.; Capocasale, G.; Zhurakivska, K.; Troiano, G.; Russo, L.L.; Muzio, L.L. The Association between Tooth Loss and Alzheimer’s Disease: A Systematic Review with Meta-Analysis of Case Control Studies. Dent. J. 2019, 7, 49. [Google Scholar] [CrossRef] [Green Version]
- Stein, P.S.; Desrosiers, M.; Donegan, S.J.; Yepes, J.F.; Kryscio, R.J. Tooth loss, dementia and neuropathology in the Nun study. J. Am. Dent. Assoc. 2007, 138, 1314–1322. [Google Scholar] [CrossRef]
- Delwel, S.; Binnekade, T.T.; Perez, R.; Hertogh, C.; Scherder, E.J.A.; Lobbezoo, F. Oral hygiene and oral health in older people with dementia: A comprehensive review with focus on oral soft tissues. Clin. Oral Investig. 2018, 22, 93–108. [Google Scholar] [CrossRef] [Green Version]
- Dioguardi, M.; Troiano, G.; Laino, L.; Lo Russo, L.; Giannatempo, G.; Lauritano, F.; Cicciu, M.; Lo Muzio, L. ProTaper and WaveOne systems three-dimensional comparison of device parameters after the shaping technique. A micro-CT study on simulated root canals. Int. J. Clin. Exp. Med. 2015, 8, 17830–17834. [Google Scholar]
- Orr, M.E.; Reveles, K.R.; Yeh, C.K.; Young, E.H.; Han, X. Can Oral Health and Oral-derived Biospecimens Predict Progression of Dementia? Oral Dis. 2019, 00, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, T.; Kubota, M.; Takahashi, T.; Nakasato, A.; Nomura, T.; Furuya, J.; Kondo, H. Effects of tooth loss on brain structure: A voxel-based morphometry study. J. Prosthodont. Res. 2018, 62, 337–341. [Google Scholar] [CrossRef]
- Takagi, D.; Hirano, H.; Watanabe, Y.; Edahiro, A.; Ohara, Y.; Yoshida, H.; Kim, H.; Murakami, K.; Hironaka, S. Relationship between skeletal muscle mass and swallowing function in patients with Alzheimer’s disease. Geriatr. Gerontol. Int. 2017, 17, 402–409. [Google Scholar] [CrossRef]
- Yamamoto, T.; Hirayama, A. Effects of soft-diet feeding on synaptic density in the hippocampus and parietal cortex of senescence-accelerated mice. Brain Res. 2001, 902, 255–263. [Google Scholar] [CrossRef]
- Delwel, S.; Binnekade, T.T.; Perez, R.S.; Hertogh, C.M.; Scherder, E.J.; Lobbezoo, F. Oral health and orofacial pain in older people with dementia: A systematic review with focus on dental hard tissues. Clin. Oral Investig. 2017, 21, 17–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pritchard, A.B.; Crean, S.; Olsen, I.; Singhrao, S.K. Periodontitis, Microbiomes and their Role in Alzheimer’s Disease. Front. Aging Neurosci. 2017, 9, 336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo Muzio, L.; Pannone, G.; Santarelli, A.; Bambini, F.; Mascitti, M.; Rubini, C.; Testa, N.F.; Dioguardi, M.; Leuci, S.; Bascones, A.; et al. Is expression of p120ctn in oral squamous cell carcinomas a prognostic factor? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 789–798. [Google Scholar] [CrossRef] [Green Version]
- Stewart, R.; Sabbah, W.; Tsakos, G.; D’Aiuto, F.; Watt, R.G. Oral health and cognitive function in the Third National Health and Nutrition Examination Survey (NHANES III). Psychosom. Med. 2008, 70, 936–941. [Google Scholar] [CrossRef]
- Chen, C.K.; Wu, Y.T.; Chang, Y.C. Association between chronic periodontitis and the risk of Alzheimer’s disease: A retrospective, population-based, matched-cohort study. Alzheimer’s Res. Ther. 2017, 9, 56. [Google Scholar] [CrossRef]
- de Souza Rolim, T.; Fabri, G.M.; Nitrini, R.; Anghinah, R.; Teixeira, M.J.; de Siqueira, J.T.; Cestari, J.A.; de Siqueira, S.R. Oral infections and orofacial pain in Alzheimer’s disease: A case-control study. J. Alzheimer’s Dis. JAD 2014, 38, 823–829. [Google Scholar] [CrossRef]
- Leira, Y.; Dominguez, C.; Seoane, J.; Seoane-Romero, J.; Pias-Peleteiro, J.M.; Takkouche, B.; Blanco, J.; Aldrey, J.M. Is Periodontal Disease Associated with Alzheimer’s Disease? A Systematic Review with Meta-Analysis. Neuroepidemiology 2017, 48, 21–31. [Google Scholar] [CrossRef]


{kind=link}
| Database—Provider | Key Words | Search Details | Number of Records | Number of Records) after Limiting by Year of Publication (last 30 years) | Number of Studies Dealing with the Topic of Alzheimer’s Disease in Relation to Oral Inflammatory Processes and Bacteria | Number of Articles Investigating the Role of Periodontal Bacteria in the Onset and Progression of Alzheimer’s Disease | Articles after Removing Overlaps | Number of Articles Included in the Qualitative Analysis |
|---|---|---|---|---|---|---|---|---|
| PubMed | “Alzheimer’s Disease” AND “periodontal” | “Alzheimer’s Disease” (All Fields) AND “periodontal” (All Fields) | 96 | 96 | 48 | 7 | ||
| PubMed | “Alzheimer’s Disease” AND “periodontitis” | “Alzheimer’s Disease” (All Fields) AND “periodontitis” (All Fields] | 87 | 87 | 56 | 9 | ||
| PubMed | “dementia “AND “periodontal” | “dementia “(All Fields] AND “periodontal” (All Fields) | 118 | 117 | 41 | 3 | ||
| PubMed | “Alzheimer’s Disease” AND “actinomycetemcomitans” | “Alzheimer’s Disease” (All Fields] AND “actinomycetemcomitans” (All Fields) | 3 | 3 | 3 | 2 | ||
| PubMed | “Alzheimer’s Disease” AND “gingivalis “ | “Alzheimer’s Disease” (All Fields) AND “gingivalis” (All Fields) | 34 | 34 | 20 | 20 | ||
| PubMed | “Alzheimer’s Disease” AND “denticola “ | “Alzheimer’s Disease” (All Fields) AND “denticola” (All Fields) | 9 | 9 | 7 | 6 | ||
| PubMed | “Alzheimer’s Disease” AND “nucleatum” | “Alzheimer’s Disease” (All Fields) AND “nucleatum” (All Fields) | 4 | 4 | 4 | 3 | ||
| Scopus | “Alzheimer’s Disease” AND “periodontal“ | TITLE-ABS-KEY (“Alzheimer’s Disease” AND “periodontal”) | 234 | 232 | 84 | 8 | ||
| Scopus | “Alzheimer’s Disease” AND “periodontitis” | TITLE-ABS-KEY (“Alzheimer’s Disease” AND “periodontitis”) | 182 | 182 | 48 | 11 | ||
| Scopus | “dementia “AND “periodontal” | TITLE-ABS-KEY (“dementia” AND “periodontal”) | 217 | 214 | 71 | 4 | ||
| Scopus | “Alzheimer’s Disease” AND “actinomycetemcomitans” | TITLE-ABS-KEY (“Alzheimer’s Disease” AND “actinomycetemcomitans”) | 8 | 8 | 7 | 7 | ||
| Scopus | “Alzheimer’s Disease” AND “gingivalis “ | TITLE-ABS-KEY (“Alzheimer’s Disease” AND “gingivalis “) | 64 | 64 | 31 | 19 | ||
| Scopus | “Alzheimer’s Disease” AND “denticola “ | TITLE-ABS-KEY (“Alzheimer’s Disease” AND “denticola”) | 20 | 20 | 16 | 9 | ||
| Scopus | “Alzheimer’s Disease” AND “nucleatum” | TITLE-ABS-KEY (“Alzheimer’s Disease” AND “nucleatum”) | 12 | 12 | 8 | 6 | ||
| Total records | 1088 | 1082 | 444 | 114 | 36 | 15 |
| Reviewer 2 | Reviewer 2 | Reviewer 2 | |||
|---|---|---|---|---|---|
| Include | Exclude | Unsure | Total | ||
| Reviewer 1 | include | 15 | 2 | 1 | 18 |
| Reviewer 1 | exclude | 0 | 13 | 0 | 13 |
| Reviewer 1 | unsure | 1 | 3 | 1 | 5 |
| total | 16 | 18 | 2 | 36 |
| Author, Data, and Journal | Type of Study | Cell Lines, Tissue, Animals, and Databases | Antibodies, Antigens, Enzyme, and Proteins Investigated | Investigated Microorganisms | Results |
|---|---|---|---|---|---|
| Wu et al., 2017, Brain Behav Immun [9] | Experimental study on mice and cell lines | (CatB−/−) mice, MG6 microglia cell line, | Pg- LPS, CatB | P. gingivalis | CatB plays a critical role in the link between periodontitis and AD. |
| Hayashi et al. 2019, Exp Gerontol [10] | Experimental study on mice | Mice | Pg- LPS | P. gingivalis | LPS pg exposure worsens the prognosis in AD |
| Poole rt al. 2013, J Alzheimers Dis [11] | Experimental study on brain tissue and cell lines | Postmortem brain tissue, SVGp12 cells | LPS | T. denticola T. forsythia P. gingivalis | Associative hypothesis between LPS pg and AD |
| Carter et al 2017, Journal of Alzheimer’s disease reports [12] | Bioinformatics study on databases | GWAS databases | 78 AD genes (GWAS) | Bacteria, viruses, fungi | The use of antibiotics and antifungals could reduce the effects of AD |
| Liu et al. 2017, Sci Rep [13] | Experimental study on mice and cell lines | Mice, MG6 microglia cell line | Arg-gingipain (Rgp) and Lys-gingipain (Kgp) | P. gingivalis | Data supports the infection hypothesis of Alzheimer’s disease |
| Laugish et al.2018, J Alzheimers Dis [14] | Clinical study | Patients with dementia (N = 20 in AD and N = 20 dementia non AD) | Tau protein (T-tau) and Amyloid β (Aβ1-42) in CFS(Cerebro spinal fluid) and Antibody levels in CFS e serum | P. gingivalis T. forsythia T. denticola T. socranskii A.actinomycetemcom | The data does not support an associative hypothesis |
| Ide et al. 2016, PLoS One [15] | Observational cohort study | Patients with dementia (n = 60) | Serum inflammation, antibody and DNA assays | P.gingivalis | Study suggests there is a direct relationship between periodontitis and cognitive decline |
| Ishida et al. 2017, NPJ aging and mechanisms of disease [16] | Experimental study on mice | Mice | Amiloid β (Aβ) deposition, Aβ40, Aβ42, IL-1β and TNF-α | P. gingivalis | Concludes that periodontitis is truly a risk factor for AD |
| Dominy et al. 2019, Sci Adv [17] | Prospective pilot study | Mice and AD patients. | (Kgp), (Rgp), P. gingivalis 16S rRNA gene, P. gingivalis DNA in CFS, Aβ1–42 in cerebral mice tissue | P. gingivalis | P. gingivalis and gingipains in the brain play a central role in the pathogenesis of AD |
| Nie et al. 2019, J Alzheimers Dis [18] | Experimental study on mice | Mice | IL-1β, AβPP770, CatB, Aβ1-42, and Aβ3-42 in macrophage/monocites | P. gingivalis | Taken together, CatB may be a novel therapeutic target for preventing the periodontitis-related AD initiation and pathological progression. |
| Diaz-Zuniga et al. 2019, J Oral Microbiol [6] | Experimental study on cell line rat | Line rat cell (Mixed hippocampal cultures, Microglial cultures) | IL-1β, IL-6, TNF-α and Aβ1-42 | A. actinomycetemcomitans | Probable association between aparodontal disease sustained by Aggregatibacter and AD etiopathology |
| Sparks Stein et al. 2012, Alzheimer’s Dement [19] | Longitudinal study | Patient AD = 35, MCI = 46 and control = 76 | Antibody levels | A. actinomycetemcomitans P. gingivalis, C. rectus, T. denticola, Fusobacterium nucleatum, T. forsythia | Possible association between antibody levels and onset and progression of AD |
| Noble et al. 2014, PLoS One [20] | Case–cohort study | Patients who developed AD in follow-up | Serum IgG | P. gingivalis, T. forsythia A. actinomycetemcomitans T. denticola, C. rectus, E. nodatum and A. naeslundii | Serum IgG levels to common periodontal microbiota are associated with risk for developing incident AD |
| Carter et al. 2017, Front Aging Neurosci [21] | Bioinformatics study on databases | GWAS databases | P. gingivalis/host interactome | P. gingivalis | Supports the many documented relationships between P. gingivalis infection and AD or its comorbid conditions |
| Kamer et al. 2009, J Neuroimmunol [22] | Observational Study | 18 with AD and 16 cognitively normal | Plasma TNF-α, IL-1β and IL-6 levels, IgG antibody | A. actinomycetemcomitans serotype b, T. forsythia and P. gingivalis | Antibody levels to periodontal bacteria associate with AD and may help improve the clinical diagnosis of AD |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dioguardi, M.; Crincoli, V.; Laino, L.; Alovisi, M.; Sovereto, D.; Mastrangelo, F.; Lo Russo, L.; Lo Muzio, L. The Role of Periodontitis and Periodontal Bacteria in the Onset and Progression of Alzheimer’s Disease: A Systematic Review. J. Clin. Med. 2020, 9, 495. https://doi.org/10.3390/jcm9020495
Dioguardi M, Crincoli V, Laino L, Alovisi M, Sovereto D, Mastrangelo F, Lo Russo L, Lo Muzio L. The Role of Periodontitis and Periodontal Bacteria in the Onset and Progression of Alzheimer’s Disease: A Systematic Review. Journal of Clinical Medicine. 2020; 9(2):495. https://doi.org/10.3390/jcm9020495
Chicago/Turabian StyleDioguardi, Mario, Vito Crincoli, Luigi Laino, Mario Alovisi, Diego Sovereto, Filiberto Mastrangelo, Lucio Lo Russo, and Lorenzo Lo Muzio. 2020. "The Role of Periodontitis and Periodontal Bacteria in the Onset and Progression of Alzheimer’s Disease: A Systematic Review" Journal of Clinical Medicine 9, no. 2: 495. https://doi.org/10.3390/jcm9020495