
Abstract
Head and neck squamous cell carcinoma (HNSCC) is a common malignant cancer that accounts for 5–10% of all cancers. This study aimed to identify essential genes associated with the prognosis of HNSCC and construct a powerful prognostic model for the risk assessment of HNSCC. RNAseq expression profile data for the patients with HNSCC were obtained from the TCGA database (GEO). A total of 500 samples with full clinical following-up were randomly divided into a training set and a validation set. The training set was used to screen for differentially expressed lncRNAs. Single-factor survival analysis was performed to obtain lncRNAs that associated with prognosis. A robust likelihood-based survival model was constructed to identify the lncRNAs that are essential for the prognosis of HNSCC. A co-expression network between genes and lncRNAs was also constructed to identify lncRNAs co-expressed with genes to serve as the final signature lncRNAs for prognosis. Finally, the prognostic effect of the signature lncRNAs was tested by multi-factor survival analysis and a scoring model for the prognosis of HNSCC was constructed. Moreover, the results of the validation set and the relative expression levels of the signature lncRNAs in the tumour and the adjacent tissue were consistent with the results of the training set. The 5 lncRNAs were distributed among 3 expression modules. Further KEGG pathway enrichment analysis showed that these 3 co-expressed modules participate in different pathways, and many of these pathways are associated with the development and progression of disease. Therefore, we proposed that the 5 validated lncRNAs can be used to predict the prognosis of HNSCC patients and can be applied in postoperative treatment and follow-up.
Similar content being viewed by others


Introduction
Head and neck squamous cell carcinomas (HNSCCs) are the most common cancer of the head and neck region1. Of these cancers, pharyngeal squamous cell carcinoma (PSCC), laryngeal squamous cell carcinoma (LSCC), and oral squamous cell carcinoma (OSCC) are the most common ones. These cancers account for approximately 5–10% of all cancers and have an average incidence of approximately 10–15 per 100,000 individuals2. Moreover, studies have shown an increasing trend in the incidence of a highly malignant form of these cancers in recent years. Despite the rapid development of medical techniques and the continuous improvement of techniques for early diagnosis of HNSCC, advanced cases still account for approximately 50% of clinical diagnoses. Although, surgical procedures, radiotherapy, and chemotherapy have been greatly improved in the past 20 years, but the 5-year survival rate of HNSCC has not been significantly improved, especially for the advanced patients. Therefore, determination of core hallmarks of early-stage cancer is urgently required to improve patient prognosis.
An increasing number of studies have shown that head and neck cancer is a genetic disease in which many oncogenes and tumour suppressor genes participate in a synergistic process involving many stages and pathways3. The mechanisms for the pathogenesis and progression of head and neck cancer have been thoroughly studied at the cell and molecular levels, especially at the gene and long non-coding RNA (lncRNA) levels. These studies searched for genes and lncRNAs associated with head and neck cancer and found that some of these genes played important roles in prognosis, treatment, and prevention4. Early detection of these genes and markers has resulted in a new method for investigation of the pathogenic mechanisms of head and neck cancer and to increased accuracy of clinical treatment and prognostic evaluation.
With the rapid development of experimental techniques and computational studies for lncRNA discovery, a large number of lncRNAs have been discovered in various eukaryotic organisms. However, the function of lncRNAs in head and neck squamous cell carcinoma remains unintelligible. In particular, there are no robust lncRNA sets to predict the prognosis of HNSCC. Therefore, in this study, we tried to identify essential lncRNAs associated with HNSCC prognosis and construct a powerful prognostic model for risk assessment of HNSCC.
Results
Data source and pre-processing
A total of 500 head and neck cancer samples and a total of 14448 lncRNA expression values were obtained from TCGA RNAseq data5. Then, the 500 samples were randomly and equally divided into a training set and a validation set, as shown in Table 1. The training set was then used to construct the model; Fig. 1 is a flowchart of the model construction process.

Flowchart of the model construction process. A total of 500 samples with full clinical follow-up were randomly divided into a training set and a validation set. The training set was used to screen for differentially expressed lncRNAs. Single-factor survival analysis was used to obtain lncRNAs associated with prognosis. A robust likelihood-based survival model was constructed to identify lncRNAs that are essential for disease prognosis. A co-expression network of genes and lncRNAs was also constructed to identify lncRNAs co-expressed with genes to serve as the final signature lncRNAs for disease prognosis. Then, the prognostic effects of the signature lncRNAs were tested by multi-factor survival analysis, and a disease prognosis-scoring model was constructed.
Screening for differentially expressed genes
6654 altered lncRNAs were identified among the 14448 lncRNAs in the training set according to the screening criteria. The expression levels of the 6654 lncRNAs in the 250 samples obtained from screening were subjected to single-factor survival analysis with coxph, and 685 differentially expressed lncRNAs with prognostic significance were identified (p < 0.05, Table 2). The 685 lncRNAs were subsequently used as seed lncRNAs. Table 2 shows the 20 most significant lncRNAs.
Screening for signature lncRNAs that affect prognosis
A total of 644 lncRNAs emerged from the results of 1000 cycles of robust likelihood-based survival modelling (Table 3). Table 3 shows the 20 lncRNAs with the highest frequencies. Figure 2 shows the frequency histogram of the 644 lncRNAs. There was a large gap between lncRNAs with frequencies of 123 and 143. Finally, we selected lncRNAs with a frequency of 143 or more as signature lncRNAs that affected prognosis.

Frequency histogram (1000 cycles) of random lncRNAs. A total of 644 lncRNAs emerged from the results of 1000 cycles of robust likelihood-based survival modelling. Figure 2 shows a frequency histogram of the 644 lncRNAs. The horizontal axis shows all the lncRNAs sorted by frequency from low to high; the vertical axis shows the frequency of the lncRNA in 1000 cycles of robust likelihood-based survival modelling. There was a large gap between lncRNAs with frequencies of 123 and 143. Finally, we selected lncRNAs with a frequency of 143 or more as signature lncRNAs affecting prognosis.
Unsupervised clustering analysis and prognostic signature analysis of the expression profiles of signature lncRNAs
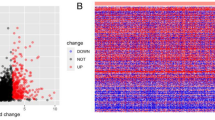
Six disease prognostic signature lncRNA expression profiles were extracted, and unsupervised hierarchical clustering was performed on the expression profiles of signature lncRNAs. Euclidean distance clustering was used. As shown in Fig. 3A, the expression levels of the 6 lncRNAs were used to divide the samples into two groups, cluster 1 and cluster 2, with 77 and 173 samples, respectively.

Unsupervised clustering analysis and prognostic signature analysis of the expression profiles of signature lncRNAs. (A) Expression profile clustering results of the 6 disease prognostic signature lncRNAs. Values in dendrogram 3A represent the lncRNA expression levels from the hierarchical cluster analysis using Euclidean distances. The horizontal axis represents samples, and the vertical axis represents lncRNAs. Euclidean distance was used to calculate distance. (B) Unsupervised clustering yielded the two groups: cluster 1 and cluster 2. The prognostic differences between the two groups was further analysed. (C) Correlation analysis of the expression of the 6 lncRNAs. Scatter plots of the expression levels between lncRNAs are presented in the lower left corner. Correlation of expression shown from red to blue with correlation coefficients from −1 to +1 in the upper right corner. A distribution histogram of lncRNA expression is shown along the diagonal (a high-resolution image is presented in Fig. 2).
Kaplan-Meier survival analysis was used for further analysis of the prognostic differences between cluster 1 and cluster 2 (Fig. 3B). The figure shows that patients in cluster 1 and cluster 2 had significant differences in prognosis, demonstrating that the expression levels of these 6 lncRNAs could be used to effectively distinguish low- and high-risk patients in the clinic. The expression correlation of the 6 lncRNAs was calculated (Fig. 3C). The expression correlation of most of the lncRNAs was low, showing that there was little intersection in the information carried between these lncRNAs, and redundancy was low.
Construction of the lncRNA-gene co-expression network
Network construction was performed after combining genes with differential lncRNA expression using the WGCNA R package. Studies have shown that the co-expression network was scale independent, with a correlation coefficient greater than 0.8. We selected the appropriate β value (β = 6) to ensure that the network was scale independent (Fig. 4A,B). Next, the expression matrix was converted into an adjacency matrix, and then the adjacency matrix was converted into a topological matrix. Based on topological overlap measure (TOM), we used the average-linkage hierarchical clustering method to cluster the genes according to the mixed dynamic tree cut standards, and set the minimum number of genes in each gene (lncRNA) network module to 30. After using the dynamic tree cut method to confirm the gene modules, we successively calculated the eigengenes of each module and then performed clustering analysis on the modules. Modules that were close together were combined into new modules, and the height was set to 0.25. A total of 71 modules were obtained (Fig. 4C). Notably, the grey modules could not be clustered with any other modules. Of the 6 lncRNAs, 5 were matched to 3 modules: green (RP11-180M15.7, RP11-474D1.3), magenta (RP11-197N18.2, RP11-347C18.5), and brown (AC021188.4). These 3 modules contained 637, 334, and 752 genes/lncRNAs, respectively.

Construction of a lncRNA-gene co-expression network. (A,B) Depict analyses of network topology for various soft-thresholding powers. (C) Depicts a gene dendrogram, and the modules are shown in different colours.
Enrichment analysis of the genes in the three co-expressed modules
The clusterProfiler R package was used for enrichment analysis of the genes in the 3 co-expressed modules.Fifty-five KEGG pathways were enriched in the 3 modules, as shown in Fig. 5D, and different pathways were enriched in different modules. There were very few pathways shared between the modules, suggesting that these modules have mutually independent functions. The pathways enriched in the green module were cell cycle, DNA replication, oocyte meiosis, p53 signalling, mismatch repair, and other pathways closely associated with cancer development and progression (Fig. 5A). The pathways enriched in the brown module were associated with signal transduction (Fig. 5B), and those in the magenta module were associated with the spliceosome and mRNA surveillance pathway (Fig. 5C). The pathways enriched in these 3 modules are closely associated with cancer development and progression.

Enrichment analysis of the genes in the three co-expressed modules. (A–C) Show the most significant enrichment results for the genes in the modules shown in green, brown, and magenta, respectively. (D) Shows all enrichment results for the three modules; the lncRNA dendrogram was obtained by average linkage hierarchical clustering. The row of colours underneath the dendrogram shows the module assignment determined by Dynamic Tree Cut.
Prognostic value of lncRNA signatures for assessing clinical outcome of head and neck cancer
A prognostic risk model was constructed from the 5 disease prognostic signature lncRNAs. First, multi-factor survival analysis was used to construct a prognostic risk assessment system from the lncRNAs in the 3 modules using the Equation 1
The concordance index of this model was 0.743, indicating that this model had high reliability. We calculated the risk score for each sample according to the risk assessment model and determined the lncRNA expression status and prognosis associated with different risk scores (Fig. 6). The figure shows that patient mortality risk increased as the risk score increased and that as the risk score increased, the expression levels of the 5 lncRNAs gradually decreased.

A prognostic risk model was constructed from the 5 disease prognostic signature lncRNAs. The horizontal axis represents samples. (A) Samples sorted by risk score; (B) Disease prognosis and survival time corresponding to different risk scores in (A). Green, alive at follow-up, red, already deceased. The figure shows that as risk scores increased, patient mortality risk increased. (C) Expression levels of the 5 signature lncRNAs corresponding to different risk scores in (A). The figure shows that as the risk score increased, the expression levels of the 5 lncRNAs gradually decreased.
ROC analysis of the scoring model for screening the best classification threshold values
He risk score of the test set was calculated according to the risk assessment system. The survival ROC R package was used to perform ROC analysis of the risk assessment system6. The results in Fig. 7A show that the AUC was 0.762. A best threshold value of -1.47 was further selected for classification, and prognostic difference analysis was performed after classification (Fig. 7B). The results showed that there was a significant difference in prognosis and survival between the high- and low-risk groups.

ROC analysis of the scoring model for screening the best classification threshold values. (A) ROC curve of the risk score model. (B) Prognostic difference analysis after classifying samples into high- and low-risk groups according to the best threshold value.
Data validation by the validation set
To validate the repeatability and portability of these 5 head and neck cancer prognosis-related lncRNAs, we performed survival analysis using the validation set. Multi-factor survival analysis was performed on the 5 lncRNAs (Fig. 8). The results showed that the 5 lncRNAs also had good classification results with the validation set and that the classification of patient prognosis was highly significant. This finding further showed that the 5 signature lncRNAs screened are essential lncRNAs that significantly affect head and neck cancer prognosis.

Validation of the 5-lncRNA prognostic model using the validation set. (A) AUC curve of the 5-lncRNA prognostic model. (B) K-M curve of the prognostic model.
Expression of the signature lncRNAs in tumour cell lines and tissues
The relative expression level of the signature lncRNAs in tumour cell lines and tissues was verified by qRT-PCR. The results showed that the relative expression levels of the signature lncRNAs were significantly lower in tumour cell lines (6-10B, 5-8F, Tu-686 and Fadu) than in a human immortalized normal cell line (DOK) (Fig. 9). In addition, the four signature lncRNAs were significantly down-regulated in the tumour compared with the adjacent tissue (Fig. 10). We could not determine the relative expression levels of lncRNA RP11-347C18.5 in the tumour cell lines and tissues because no appropriate primers were found for analysis of this lncRNA. Therefore, analysis only four lncRNAs are shown in in Figs 9 and 10.

Relative expression levels of four signature lncRNAs in head and neck tumour cell lines. The relative expression levels of four signature lncRNAs in head and neck tumour cell lines (6–10B, 5–8 F, Tu-686 and Fadu) and a human immortalized normal cell line (DOK). (A) The expression level of RP11-197N18.2; (B) The expression level of RP11-474D1.3; (C) The expression level of RP11-180M15.7; (D) The expression level of AC021188.4. The results showed that the relative expression levels of the signature lncRNAs were significantly lower in tumour cell lines (6-10B, 5–8 F, Tu-686 and Fadu) than in a human immortalized normal cell line (DOK).

Relative expression levels of four signature lncRNAs in head and neck tumours and adjacent tissues. The relative expression levels of four signature lncRNAs in 28 pairs of head and neck tumours and adjacent tissues. (A) The expression level of RP11-197N18.2,it is was down-regulated in tumours in 22 cases; (B) The expression level of RP11-474D1.3 was down-regulated in tumours in 21 cases; (C) The expression level of RP11-180M15.7 was down-regulated in tumours in 24 cases; (D) The expression level of AC021188.4 was down-regulated in tumours in 24 cases. The four signature lncRNAs were significantly down-regulated in tumours compared with the adjacent tissue.
Discussion
LncRNAs are defined as RNA molecules greater than 200 nucleotides in length7. Due to the special characteristics of lncRNAs, i.e., low expression levels and highly tissue-specific patterns, lncRNAs were previously misidentified as merely “transcriptional noise”. However, accumulating evidence from biological experiments has indicated that lncRNAs carry out various crucial functions, clearly contradicting the conventional viewpoint8. An increasing number of studies have shown that lncRNAs are essential factors in the regulation of various cellular processes, including nuclear substructure organization, changes in chromatin state, and regulation of gene expression and activity via interactions with effector proteins9. Moreover, recent studies have indicated that lncRNAs play important roles in pathological conditions. Dysfunction of lncRNAs is clearly associated with the development and progression of a wide range of cancers, such as leukaemia, breast cancer, lung cancer, prostate cancer, and ovarian cancer. For example, there is increasing evidence that lncRNAs may exert their effects by regulating protein complexes essential for the regulation of cellular functions and metabolism, and transcription and chromatin state are dynamically regulated by lncRNAs10,11,12. Many reports have already shown that dysregulation of lncRNAs can also affect the regulation of the eukaryotic genome, resulting in cancer progression and uncontrolled growth13,14,15. Therefore, lncRNAs play an important role in cancer and tumour suppressor networks. It has been reported that lncRNAs participate in human cancer progression by regulating cell growth, apoptosis, and invasion16,17,18.
However, the role of lncRNAs in head and neck cancer remains unknown. In particular, there are no robust lncRNA sets to predict the prognosis of head and neck cancer. Fortunately, an increasing number of computational models have been developed to analyse the associations between lncRNAs and disease in recent years. These models provide the most promising lncRNA-disease associations for further experimental validation, hence decreasing the time and cost of biological experiments19,20,21. For example, LRLSLDA is a global ranking approach that can prioritize potential lncRNA-disease associations for all diseases simultaneously. LRLSLDA represents a novel, important and powerful tool in biomedical research for disease treatment and drug discovery, and a cancer hallmark network-based framework for modelling genome sequencing data to predict clonal evolution of cancer and the associated clinical phenotypes was developed by Edwin Wanga et al.22.
This study screened and analysed for lncRNAs that affect the prognosis of HNSCC using a bioinformatic method, and 5 lncRNAs, namely, RP11-180M15.7, RP11-197N18.2, AC021188.4, RP11-474D1.3, and RP11-347C18.5, were identified. These lncRNAs are closely associated with head and neck cancer prognosis and participate in many KEGG pathways that are involved in cancer development and progression23. Moreover, the relative expression levels in the four cancer cell lines, tumours and adjacent tissue are were consistent with previous predictions. There have been very few studies on RP11-180M15.7, RP11-197N18.2, AC021188.4, RP11-474D1.3, and RP11-347C18.5. Zhiqun Li et al. found that Homo sapiens 12 BAC RP11-180M15 interacts with the middle hepatitis B virus surface protein using a yeast two-hybrid screen and hypothesized that this interaction was closely associated with the development and progression of different forms of cancer24. The other four lncRNAs have not been reported in the literature. Three co-expression modules obtained from enrichment analysis by the clusterProfiler R package showed that pathways closely associated with cancer development and progression were enriched, such as signal transduction, cell cycle, DNA replication, oocyte meiosis, the p53 signalling pathway, mismatch repair, the spliceosome, the mRNA surveillance pathway. We constructed a prognostic risk model using these 5 disease prognostic signature lncRNAs. This model can effectively assess prognostic differences in patients. Simultaneously, the validation set data were used for survival analysis. The results of multi-factor survival analysis of the 5 lncRNAs in the validation set also showed effective classification, which is highly significant for patient prognosis classification. The results of our study show that the 5 lncRNAs are essential lncRNAs that significantly affect head and neck cancer prognosis.
Materials and Methods
Data download and pre-processing
Head and neck cancer RNAseq expression profile data were downloaded from the TCGA database. The database contained a total of 500 samples with clinical and follow-up data, from which coding genes and lncRNAs were isolated. Simultaneously, the samples were randomly divided into a training set and a validation set. The training set was used to construct the model, and the validation set data were used as external data to validate the effectiveness of the model25.
Initial screening of differentially expressed lncRNAs in cancerous tissues from head and neck cancer patients
Survival time and lncRNA expression level are closely associated among different patients with the same disease. First, we needed to screen for lncRNAs that strongly interfered with expression in different patients and for lncRNAs that exhibited differential expression in disease samples. The criteria for these lncRNAs was according to the report of Li, J.25.
Seed lncRNA screening
Survival analysis refers to the analysis and inference of animal or human survival time based on data obtained from experiments or surveys and is a method for studying the relationship between many influencing factors and survival time, endpoint, size and extent.
We used the survival R package to perform single-factor survival analysis on the lncRNAs obtained from disease samples that met the criteria for change and selected lncRNAs with a significance level of p < 0.05 as seed lncRNAs26,27.
Screening of key prognostic lncRNAs
There were excess seed lncRNAs obtained from preliminary screening, making it difficult to use these lncRNAs for clinical diagnosis. We constructed a robust likelihood-based survival model to screen signature lncRNAs using the rbsurv R package28,29. The procedure was according to the report of Zhiqiang Wang30.
We randomly selected 125 samples for 1000 cycles of robust likelihood-based survival modelling. The several lncRNAs with the highest frequencies that emerged were designated the final prognostic signature lncRNAs.
Expression profile clustering of prognostic signature lncRNAs
The samples were sorted using unsupervised hierarchical clustering according to the expression profile of the signature lncRNAs. Kaplan-Meier survival analysis was used to further sort prognostic differences among samples31.
Construction of a gene-lncRNA co-expression network
Weighted gene co-expression network analysis (WGCNA) is a systems biological method that uses gene expression data to construct a scale-independent network. The basic concept was as follows32: First, a gene expression similarity matrix was constructed by calculating the absolute value of the Pearson correlation coefficients between pairs of genes. The Pearson correlation coefficient between gene i and gene j was calculated using Equation 2, in which i and j represent the expression of the ith and jth genes, respectively.
Next, Equation 3 was used to convert the gene expression similarity matrix into an adjacency matrix. The graph type was signed. In this equation, β is the soft threshold, which is actually the Pearson correlation coefficient of each pair of genes raised to the power of β. This step can strengthen strong correlations and weaken weak correlations from the index scale.
Next, Equation 4 was used to convert the adjacency matrix into a topological matrix. TOM was used to describe the degree of association between genes.
1-TOM represents the degree of dissimilarity between gene i and gene j. 1-TOM was used as the distance for hierarchical clustering of genes. Next, the Dynamic Tree Cut method was used to distinguish between modules. The most representative gene in each module was designated the module eigengene (ME), which represented the overall gene expression level of that module; the ME was the first principal component of each module. Equation 5 was used to calculate the ME, where i represents a gene in module q, and l represents the microarray sample of module q.
We used the Pearson correlation coefficient between the expression profile of a given gene among all samples and the expression profile of the ME to measure the membership of the gene in the module; this is known as module membership (MM). Equation 6 was used to calculate MM, where represents the expression profile of the ith gene, which represents the ME of module q, and represents the membership of gene i in module q. = 0 indicates that gene i is not present in module q, and the closer is to +1 or −1, the more closely gene i is associated with module q. The sign indicate whether gene i is positively or negatively correlated with module q.
Gene significance (GS) was used to measure the degree of association between a gene and external information. Higher values of GS indicate that the gene has greater biological significance. GS = 0 indicates that the gene does not participate in the biological question of interest.
We selected expression data for differentially expressed lncRNAs and differentially expressed genes. The WGCNA R package was used to construct a weighted co-expression network. A soft threshold of 6 was selected for screening of co-expressed modules.
Co-expression module enrichment analysis
To determine the functions of lncRNAs involved in each co-expression module, we used the clusterProfiler R package to perform KEGG pathway enrichment analysis on each module33.
Risk assessment model construction and evaluation
Multi-factor Cox regression was used on the obtained prognostic signature lncRNAs participating in co-expressed modules34,35. A patient risk assessment system based on the regression coefficients combined with lncRNA expression weighted by the regression coefficients was constructed, and the risk score for each patient was obtained. In other words, the risk score was the linear combination of the lncRNA expression values weighted by the regression coefficients. The risk assessment score of each patient was calculated according to Equation 1. Simultaneously, we used the β value obtained from the training set to assess risk in the cancer patients in the validation set.
Correlation analysis between the risk assessment model and clinical characteristics
The risk score of each sample was calculated according to the risk assessment system. Using the median risk score as the boundary, the samples were divided into high-risk and low-risk types. In addition, these values were combined with the corresponding clinical characteristics of each sample to analyse the relationship between risk score and each clinical characteristic.
Patients and tissue preparation
This study was conducted on a total of 28 head and neck tumour samples, which were histopathologically and clinically diagnosed at Xiangya Hospital, Central South University. For the use of these clinical materials for research purposes, prior consent was obtained from all patients, who provided written informed consent, and all research was performed in accordance with relevant guidelines. This study was approved by the Ethics Committee of the Xiangya Hospital of Central South University (ethics committee reference number: 201512549). The patients included 26 males and 2 females. None of the patients had a history of previous malignancies, radiotherapy or chemotherapy. The clinical information for and pathological characteristics of all patients are summarized in Table 4.
Cell culture
Four head and neck cancer cell lines (6-10B, 5-8F, Tu-686 and Fadu) and one human immortalized normal cell line (DOK) were used in this study, all of which were cultured in complete medium (RPMI-1640) supplemented with 10% foetal bovine serum (Gibco; Thermo Fisher Scientific, Inc., Waltham, MA, USA), streptomycin (100 mg/ml), penicillin (100 U/ml), 25 mM 4-(2-hydroxyethyl)-1-piperazineethanesulphonic acid (HEPES) and 2 mM glutamine. All of the cell lines were maintained as monolayers in a 10-cm plastic dish and cultured in an incubator with a humidified atmosphere containing 5% CO2 at 37 °C.
Quantitative reverse transcription polymerase chain reaction (RT-qPCR)
TThe relative expression levels of four signature lncRNAs in head and neck tumours and adjacent tissues were determined using RT-qPCR assays. Total RNA was extracted with TRIzol reagent (Invitrogen; Thermo Fisher Scientific Thermo Fisher Scientific, Inc.), and reverse transcription was performed using the All-in-One First Strand Synthesis Kit (GeneCopoeia, Rockville, MD, USA) according to the manufacturer’s protocol. The primer sequences for RP11-197N18.2, RP11-474D1.3, RP11-180M15.7, and AC021188.4 were determined using Primer Premier 5.0 software (Premier Biosoft, Palo Alto, CA, USA), and glyceraldehyde-3-phosphate hydrogenase (GAPDH) was used as a control. The primer sequences for RP11-197N18.2 were as follows: 5′-CCGGGTTCCCATTCTGCTTC-3′ (sense) and 5′-TCTTCCACAATGACAGCCGC-3′ (antisense). The primer sequences for RP11-474D1.3 were as follows: 5′-ACTTGCGCTTCACACTGGAC-3′ (sense) and 5′-GAAATTCTCCTGCGGGGACC-3′ (antisense). The primer sequences for RP11-180M15.7 were as follows: 5′-CCATCGGGTAGGAAGGTCGT-3′ (sense) and 5′-TCGGACTGAGGGAGTACCCTA-3′ (antisense). The primer sequences for RP11-180M15.7 were as follows: 5′-TACAGAAACAGAGTGGAATCTCCG-3′ (sense) and 5′-TTTTATTCCATGATCAGGCTGTGGC-3′ (antisense). The primer sequences for GAPDH were as follows: 5′-ATCAAGAAGGTGGTGAAGCAG-3′ (sense) and 5′-TGGAGGAGTGGGTGTCGC-3′ (antisense). Products were amplified by PCR using the All-in-One qPCR mix (GeneCopoeia, Rockville, MD, USA) and data was obtained and analyzed with a Applied Biosystems ViiA™ 7 Real-Time PCR system. All RT reactions were performed in triplicate, and experimental procedures of qPCR were based on MIQE guidelines. The relative expression levels determined by the 2−ΔΔct method.
References
Lin, Y. C. et al. Metformin sensitizes anticancer effect of dasatinib in head and neck squamous cell carcinoma cells through AMPK-dependent ER stress. Oncotarget 5, 298–308 (2014).
Pickhard, A. et al. The response of head and neck squamous cell carcinoma to cetuximab treatment depends on Aurora kinase A polymorphism. Oncotarget 5, 5428–5438 (2014).
Bonnin, N. et al. MiR-422a promotes loco-regional recurrence by targeting NT5E/CD73 in head and neck squamous cell carcinoma. Oncotarget 7, 44023–44038 (2016).
Ma, X. et al. LncRNAs as an intermediate in HPV16 promoting myeloid-derived suppressor cell recruitment of head and neck squamous cell carcinoma. Oncotarget 8, 42061–42075 (2017).
Wang, Z., Jensen, M. A. & Zenklusen, J. C. A Practical Guide to The Cancer Genome Atlas (TCGA). Methods in molecular biology 1418, 111–141 (2016).
Heagerty, P. J., Lumley, T. & Pepe, M. S. Time-dependent ROC curves for censored srvival data and a diagnostic marker. Biometrics 56, 337–344 (2000).
Toiber, D., Leprivier, G. & Rotblat, B. Long noncoding RNA: noncoding and not coded. Cell death discovery 3, 17035 (2017).
Xing, C. et al. FMLNCSIM: fuzzy measure-based lncRNA functional similarity calculation model. Oncotarget 7, 45948–45957 (2016).
Li, Y., Syed, J. & Sugiyama, H. RNA-DNA Triplex Formation by Long Noncoding RNAs. Cell chemical biology 23, 1325–1333 (2016).
Zhang, Y., Tao,Y. & Liao, Q. Long noncoding RNA: a crosslink in biological regulatory network. Briefings in bioinformatics. 2017.
Mach, J. The Long-noncoding RNA ELENA1 functions in plant immunity. The Plant cell 29, 916 (2017).
Weikard, R., Demasius, W. & Kuehn, C. Mining long noncoding RNA in livestock. Animal genetics 48, 3–18 (2017).
Xu, S., Kong, D., Chen, Q., Ping, Y. & Pang, D. Oncogenic long noncoding RNA landscape in breast cancer. Molecular cancer 16, 129 (2017).
Luo, Y., Morgan, S. L. & Wang, K. C. PICSAR: Long Noncoding RNA in cutaneous squamous cell carcinoma. The Journal of investigative dermatology 136, 1541–1542 (2016).
Yang, F., Wang, L. H. & Zhu, R. F. Prognostic value of long noncoding RNA TUG1 in human cancers. Minerva medica 108, 101–102 (2017).
Liu, D. et al. The gain and loss of long noncoding RNA associated-competing endogenous RNAs in prostate cancer. Oncotarget 7, 57228–57238 (2016).
Tian, J. et al. Identification of the long noncoding RNA LET as a novel tumor suppressor in gastric cancer. Molecular medicine reports 15, 2229–2234 (2017).
Li, C. et al. Increased long noncoding RNA SNHG20 predicts poor prognosis in colorectal cancer. BMC cancer 16, 655 (2016).
Chen, X. & Yan, G. Y. Novel human lncRNA-disease association inference based on lncRNA expression profiles. Bioinformatics 29, 2617–2624 (2013).
Huang, Y.-A. et al. ILNCSIM: improved lncRNA functional similarity calculation model. Oncotarget 7, 25902–25914 (2016).
Li, J. et al. Identification of high-quality cancer prognostic markers and metastasis network modules. Nat Commun 1, 2617–2624 (2010).
Wang, E. et al. Predictive genomics: a cancer hallmark network framework for predicting tumor clinical phenotypes using genome sequencing data. Seminars in cancer biology 30, 4–12 (2015).
Kanehisa, M. & Goto, S. KEGG: kyoto encyclopedia of genes and genomes. Nucleic acids research 28, 27–30 (2000).
Li, Z., Ling, H. E. & Cheng, J. Screening of hepatocyte proteins binding with the middle surface protein of the hepatitis B virus by the yeast two-hybrid system. Molecular medicine reports 9, 2342–2346 (2014).
Li, J., Wang, J., Chen, Y., Yang, L. & Chen, S. A prognostic 4-gene expression signature for squamous cell lung carcinoma. Journal of cellular physiology 232, 3702–3713 (2017).
Friedman, J., Hastie, T. & Tibshirani, R. Regularization paths for generalized linear models via coordinate descent. Journal of statistical software 33, 1–22 (2010).
Hakulinen, T. & Abeywickrama, K. H. A computer program package for relative survival analysis. Computer programs in biomedicine 19, 197–207 (1985).
Wang, J. Y. & Tai, J. J. Robust quantitative trait association tests in the parent-offspring triad design: conditional likelihood-based approaches. Annals of human genetics 73, 231–244 (2009).
Kendall, W. L., Pollock, K. H. & Brownie, C. A likelihood-based approach to capture-recapture estimation of demographic parameters under the robust design. Biometrics 51, 293–308 (1995).
Wang, Z., Chen, G., Wang, Q., Lu, W. & Xu, M. Identification and validation of a prognostic 9-genes expression signature for gastric cancer. Oncotarget 8, 73826–73836 (2017).
Lacny, S. et al. Kaplan-Meier survival analysis overestimates the risk of revision arthroplasty: A meta-analysis. Clinical orthopaedics and related research 473, 3431–3442 (2015).
Langfelder, P. & Horvath, S. WGCNA: an R package for weighted correlation network analysis. BMC bioinformatics 9, 559 (2008).
Yu, G., Wang, L. G., Han, Y. & He, Q. Y. ClusterProfiler: an R package for comparing biological themes among gene clusters. Omics: a journal of integrative biology 16, 284–287 (2012).
Zhou, M. et al. Characterization of long non-coding RNA-associated ceRNA network to reveal potential prognostic lncRNA biomarkers in human ovarian cancer. Oncotarget 7, 12598–12611 (2016).
O’Quigley, J. & Moreau, T. Cox’s regression model: computing a goodness of fit statistic. Computer methods and programs in biomedicine 22, 253–256 (1986).
Acknowledgements
The Natural Science Foundation of Fujian Province (no. 2015J01512). The Middle- and Young-Aged Key Personnel Projects of Fujian Provincial Health and Family Planning Commission, China (no. 2015-ZQN-JC-39). The Medical Innovation Project of Fujian Provincial Health and Family Planning Commission, China. The Science and Technology Projects of Quanzhou Science and Technology Bureau, Quanzhou, Fujian, China (no. 2014Z22). The Natural Science Youth Founds of Jiangxi Province (no. 2016BAB215249). The Natural Science Foundation of China (nos. 81660294, 81602389, 81472696, 81202128, 81272974).
Author information
Authors and Affiliations
Contributions
Liu Guancheng, Zhu Gangcai, Pi Leiming, Wang Junchen, Chen Changhan, and Li Zhexuan collected the tumours, adjacent tissues and clinical information; Zhuang Liming, Liu Jiangyi, Zheng Jinyang and Zhang Xin performed the data analysis; Chen Liangjuan and Lv Yunxia prepared all the figures; Liu Guancheng performed the RT-qPCR and Cai Gengming wrote the article. All authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, G., Zheng, J., Zhuang, L. et al. A Prognostic 5-lncRNA Expression Signature for Head and Neck Squamous Cell Carcinoma. Sci Rep 8, 15250 (2018). https://doi.org/10.1038/s41598-018-33642-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-33642-1
Keywords
This article is cited by
-
Signature Based on Six Autophagy-related Genes to Predict Prognosis of Head and Neck Squamous Cell Carcinoma
Current Medical Science (2022)
-
Transcriptomics and Epigenomics in head and neck cancer: available repositories and molecular signatures
Cancers of the Head & Neck (2020)
-
A transcriptional metabolic gene-set based prognostic signature is associated with clinical and mutational features in head and neck squamous cell carcinoma
Journal of Cancer Research and Clinical Oncology (2020)
-
An integrated nomogram combining lncRNAs classifier and clinicopathologic factors to predict the recurrence of head and neck squamous cell carcinoma
Scientific Reports (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
