
Predicting Silent Atrial Fibrillation in the Elderly: A Report from the NOMED-AF Cross-Sectional Study

 ,
,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
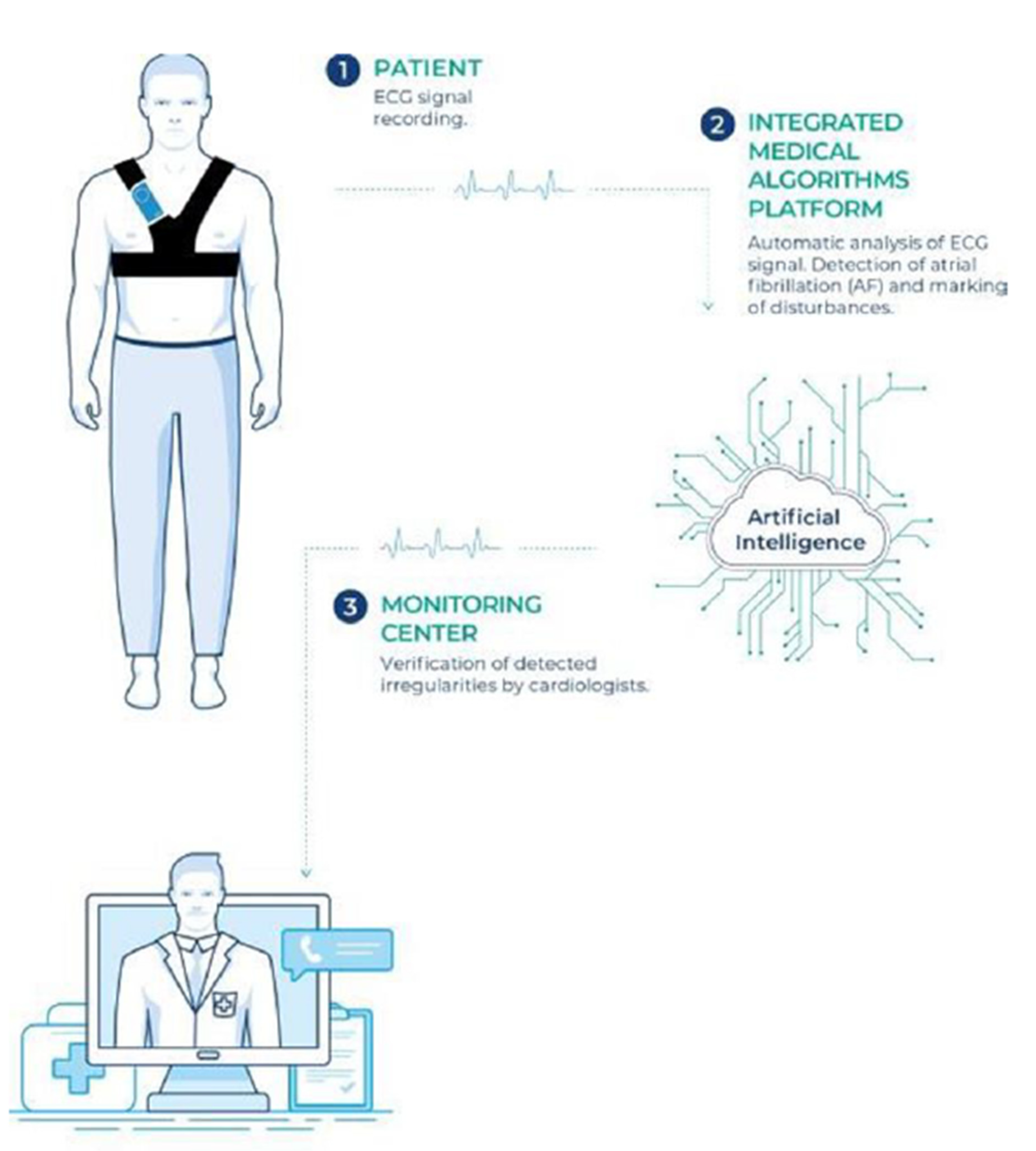
2.1. ECG Monitoring and Clinical Assessments
2.2. Statistical Analysis
3. Results
3.1. Independent Risk Factors for Atrial Fibrillation
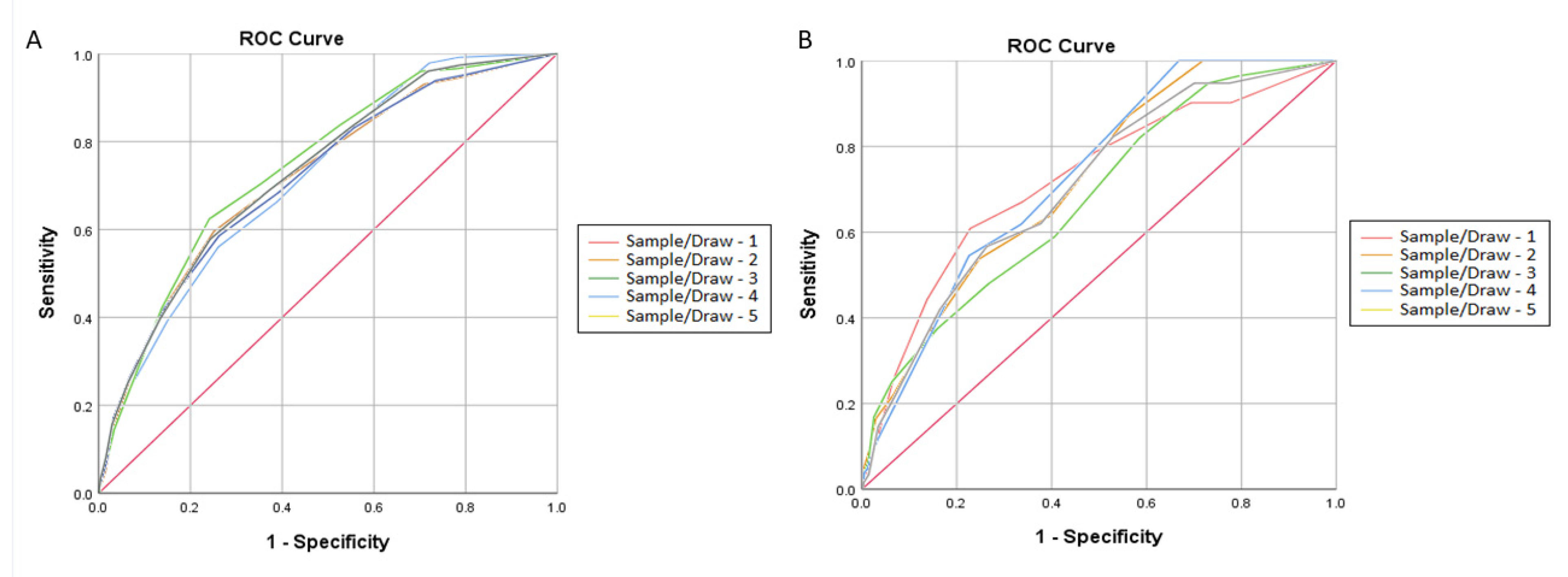
3.2. Predicting Silent Atrial Fibrillation in Subjects Aged over 65 Years
4. Discussion
Strengths and Limitations
5. Conclusions
6. Clinical Perspectives
6.1. Competency in Medical Knowledge
6.2. Competency in Patient Care
6.3. Translational Outlook
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AF | Atrial fibrillation |
| CKD | Chronic kidney disease |
| DM | Diabetes mellitus |
| ECG | Electrocardiogram |
| ESC | European Society of Cardiology |
| HF | Heart failure |
| NT-pro-BNP | N-terminal pro-b-type natriuretic peptide |
| SAF | Silent atrial fibrillation |
References
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Schnabel, R.B.; Yin, X.; Gona, P.; Larson, M.G.; Beiser, A.S.; McManus, D.D.; Newton-Cheh, C.; Lubitz, S.A.; Magnani, J.W.; Ellinor, P.T.; et al. 50 years trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: A cohort study. Lancet 2015, 386, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Allan, V.; Honarbakhsh, S.; Casas, J.P.; Wallace, J.; Hunter, R.; Schilling, R.; Perel, P.; Morley, K.; Banerjee, A.; Hemingway, H. Are cardiovascular risk factors also associated with the incidence of atrial fibrillation? A systematic review and field synopsis of 23 factors in 32 population-based cohorts of 20 million participants. Thromb. Haemost. 2017, 117, 837–850. [Google Scholar] [CrossRef] [Green Version]
- Ninni, S.; Lemesle, G.; Meurice, T.; Tricot, O.; Lamblin, N.; Bauters, C. Real-Life Incident Atrial Fibrillation in Outpatients with Coronary Artery Disease. J. Clin. Med. 2020, 9, 2367. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; Laroche, C.; Diemberger, I.; Fantecchi, E.; Popescu, M.I.; Rasmussen, L.H.; Sinagra, G.; Petrescu, L.; Tavazzi, L.; Maggioni, A.P.; et al. Asymptomatic Atrial Fibrillation: Clinical Correlates, Management, and Outcomes in the EORP-AF Pilot General Registry. Am. J. Med. 2015, 128, 509–518.e2. [Google Scholar] [CrossRef] [PubMed]
- Kalarus, Z.; Balsam, P.; Bandosz, P.; Grodzicki, T.; Kaźmierczak, J.; Kiedrowicz, R.; Mitręga, K.; Noczyński, M.; Opolski, G.; Rewiuk, K.; et al. NOninvasive Monitoring for Early Detection of Atrial Fibrillation: Rationale and design of the NOMED-AF study. Kardiol. Pol. 2018, 10, 1482–1485. [Google Scholar] [CrossRef] [Green Version]
- Dobreanu, D.; Svendsen, J.H.; Lewalter, T.; Hernández-Madrid, A.; Lip, G.Y.; Blomström-Lundqvist, C. Current practice for diagnosis and management of silent atrial fibrillation: Results of the European Heart Rhythm Association survey. Europace 2013, 15, 1223–1225. [Google Scholar] [CrossRef] [Green Version]
- Gladstone, D.J.; Spring, M.; Dorian, P.; Panzov, V.; Thorpe, K.E.; Hall, J.; Vaid, H.; O’Donnell, M.; Laupacis, A.; Côté, R.; et al. Atrial Fibrillation in Patients with Cryptogenic Stroke. N. Engl. J. Med. 2014, 370, 2467–2477. [Google Scholar] [CrossRef] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart. J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, prediabetes, and cardiovascular diseases developed in collaboration with the EASD The Task Force for diabetes, pre-diabetes, and cardiovascular diseases of the European Society of Cardiology (ESC) and the European Association for the Study of Diabetes (EASD). Eur. Heart J. 2020, 41, 255–323. [Google Scholar]
- American Diabetes Association. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef] [Green Version]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J.; et al. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Boriani, G.; Palmisano, P.; Malavasi, V.; Fantecchi, E.; Vitolo, M.; Bonini, N.; Imberti, J.; Valenti, A.; Schnabel, R.; Freedman, B. Clinical Factors Associated with Atrial Fibrillation Detection on Single-Time Point Screening Using a Hand-Held Single-Lead ECG Device. J. Clin. Med. 2021, 10, 729. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Wang, H.; Zhang, H.; Chen, Y.; Lip, G.Y.H. Population-Based Screening or Targeted Screening Based on Initial Clinical Risk Assessment for Atrial Fibrillation: A Report from the Huawei Heart Study. J. Clin. Med. 2020, 9, 1493. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Inker, L.A.; Levey, A.S. Pro: Estimating GFR using the chronic kidney disease epidemiology collaboration (CKD-EPI) 2009 creat-inine equation: The time for change is now. Nephrol. Dial. Transpl. 2013, 28, 1390–1396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation 2014, 130, 2071–2104. [Google Scholar] [CrossRef] [Green Version]
- Camm, A.J.; Kirchhof, P.; Lip, G.Y.; Schotten, U.; Savelieva, I.; Ernst, S.; Van Gelder, I.C.; Al-Attar, N. Guidelines for the management of atrial fibrillation: The Task Force for the Manage-ment of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur. Heart J. 2010, 31, 2369–2429. [Google Scholar]
- Kirchhof, P.; Lip, G.Y.; Van Gelder, I.C.; Bax, J.; Hylek, E.; Kaab, S.; Schotten, U.; Wegscheider, K.; Boriani, G.; Brandes, A.; et al. Comprehensive risk reduction in patients with atrial fibrillation: Emerging diagnostic and therapeutic options—A report from the 3rd Atrial Fibrillation Competence NETwork/European Heart Rhythm Association consensus conference. Europace 2012, 14, 8–27. [Google Scholar] [CrossRef]
- Kennedy, H.L. Silent Atrial Fibrillation: Definition, Clarification, and Unanswered Issues. Ann. Noninvasive Electrocardiol. 2015, 20, 518–525. [Google Scholar] [CrossRef]
- Marfella, R.; Sasso, F.C.; Siniscalchi, M.; Cirillo, M.; Paolisso, P.; Sardu, C.; Barbieri, M.; Rizzo, M.R.; Mauro, C.; Paolisso, G. Brief Episodes of Silent Atrial Fibrillation Predict Clinical Vascular Brain Disease in Type 2 Diabetic Patients. J. Am. Coll. Cardiol. 2013, 62, 525–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christophersen, I.E.; Yin, X.; Larson, M.G.; Lubitz, S.A.; Magnani, J.W.; McManus, D.D.; Ellinor, P.T.; Benjamin, E.J. A comparison of the CHARGE–AF and the CHA2DS2-VASc risk scores for pre-diction of atrial fibrillation in the Framingham Heart Study. Am. Heart J. 2016, 178, 45–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnabel, R.B.; Sullivan, L.; Levy, D.; Pencina, M.J.; Massaro, J.M.; D’Agostino, R.B.; Newton-Cheh, C.; Yamamoto, J.F.; Magnani, J.W.; Tadros, T.M.; et al. Development of a risk score for atrial fibrillation (Framingham Heart Study): A community-based cohort study. Lancet 2009, 373, 739–745. [Google Scholar] [CrossRef] [Green Version]
- Everett, B.M.; Cook, N.R.; Conen, D.; Chasman, D.I.; Ridker, P.M.; Albert, C.M. Novel genetic markers improve measures of atrial fibrillation risk prediction. Eur. Heart J. 2013, 34, 2243–2251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aronson, D.; Shalev, V.; Katz, R.; Chodick, G.; Mutlak, D. Risk Score for Prediction of 10-Year Atrial Fibrillation: A Community-Based Study. Thromb. Haemost. 2018, 118, 1556–1563. [Google Scholar] [CrossRef] [Green Version]
- Hamada, R.; Muto, S. Simple risk model and score for predicting of incident atrial fibrillation in Japanese. J. Cardiol. 2019, 73, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.-G.; Miyazawa, K.; Pastori, D.; Szekely, O.; Shahid, F.; Lip, G.Y. Atrial high-rate episodes and thromboembolism in patients without atrial fibrillation: The West Birmingham Atrial Fibrillation Project. Int. J. Cardiol. 2019, 292, 126–130. [Google Scholar] [CrossRef]
- Li, Y.G.; Pastori, D.; Farcomeni, A.; Yang, P.S.; Jang, E.; Joung, B.; Wang, Y.T.; Guo, Y.T.; Lip, G.Y.H. A simple clinical risk score (C2HEST) for predicting incident atrial fibrillation in Asian subjects: Derivation in 471,446 Chinese subjects, with internal validation and external application in 451,199 Korean subjects. Chest 2019, 155, 510–518. [Google Scholar] [CrossRef]
- Ding, L.; Li, J.; Wang, C.; Li, X.; Su, Q.; Zhang, G.; Xue, F. Incidence of atrial fibrillation and its risk prediction model based on a prospective urban Han Chinese cohort. J. Hum. Hypertens. 2017, 31, 574–579. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Whole Population | No AF (AF−) | AF+ | SAF | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | p (AF− vs. AF) | N | % | p (AF− vs. SAF) | |
| Age (years, mean ± SD) | 77.5 | 7.9 | 76.8 | 7.9 | 80.0 | 7.4 | <0.001 | 80.9 | 7.4 | <0.001 |
| Male gender | 1535 | 50.9% | 1122 | 48.1% | 413 | 60.7% | <0.001 | 191 | 68.5% | <0.001 |
| MI | 446 | 14.8% | 321 | 13.8% | 125 | 18.4% | 0.003 | 45 | 16.1% | 0.294 |
| CHD | 666 | 22.1% | 444 | 19.0% | 222 | 32.6% | <0.001 | 84 | 30.1% | <0.001 |
| Thyroid diseases | 418 | 13.9% | 301 | 12.9% | 117 | 17.2% | 0.005 | 42 | 15.1% | 0.337 |
| Pulmonary diseases | 361 | 12.0% | 264 | 11.3% | 97 | 14.3% | 0.040 | 32 | 11.5% | 0.974 |
| Thromboembolism | 241 | 8.0% | 166 | 7.1% | 75 | 11.0% | 0.001 | 23 | 8.2% | 0.513 |
| LEAD | 415 | 13.8% | 286 | 12.3% | 129 | 19.0% | <0.001 | 51 | 18.3% | 0.005 |
| ICS/TIA | 366 | 12.1% | 246 | 10.5% | 120 | 17.6% | <0.001 | 53 | 19.0% | <0.001 |
| PCI/CABG | 368 | 12.2% | 270 | 11.6% | 98 | 14.4% | 0.043 | 44 | 15.8% | 0.040 |
| DM | 881 | 29.2% | 628 | 26.9% | 253 | 37.2% | <0.001 | 98 | 35.1% | 0.004 |
| Heart failure | 673 | 22.3% | 396 | 17.0% | 277 | 40.7% | <0.001 | 96 | 34.4% | <0.001 |
| HA | 2433 | 80.7% | 1856 | 79.5% | 577 | 84.9% | 0.001 | 223 | 79.9% | 0.821 |
| CKD | 1005 | 33.3% | 695 | 29.8% | 310 | 45.6% | <0.001 | 144 | 51.6% | <0.001 |
| Physical activity | 1294 | 42.9% | 1039 | 44.5% | 255 | 37.5% | 0.001 | 103 | 36.9% | 0.017 |
| BMI ≥ 30 | 923 | 30.6% | 686 | 29.4% | 237 | 34.9% | 0.005 | 88 | 31.5% | 0.419 |
| hs CRP > 5 mg/L | 565 | 18.7% | 434 | 18.6% | 131 | 19.3% | 0.659 | 56 | 20.1% | 0.603 |
| NT pro-BNP > 125 pg/mL | 2288 | 75.9% | 1690 | 72.4% | 598 | 87.9% | <0.001 | 247 | 88.5% | <0.001 |
| AF Overall | SAF | |||||
|---|---|---|---|---|---|---|
| Parameter | OR | 95% CI | p | OR | 95% CI | p |
| Age (every 5 years) | 1.26 | 1.17–1.35 | <0.001 | 1.36 | 1.24–1.49 | <0.001 |
| Male gender | 2.05 | 1.67–2.51 | <0.001 | 2.58 | 1.94–3.44 | <0.001 |
| MI | 0.96 | 0.70–1.30 | 0.776 | 0.68 | 0.41–1.12 | 0.131 |
| CHD | 1.30 | 1.01–1.66 | 0.043 | 1.10 | 0.77–1.57 | 0.592 |
| Thyroid diseases | 1.44 | 1.09–1.90 | 0.010 | 1.41 | 0.98–2.03 | 0.066 |
| Pulmonary diseases | 0.87 | 0.65–1.17 | 0.353 | 0.67 | 0.43–1.04 | 0.073 |
| Thromboembolism | 1.28 | 0.91–1.81 | 0.157 | 1.41 | 0.83–2.41 | 0.204 |
| LEAD | 0.96 | 0.73–1.26 | 0.761 | 1.11 | 0.76–1.62 | 0.593 |
| ICS/TIA | 1.28 | 1.00–1.64 | 0.051 | 1.59 | 1.16–2.18 | 0.004 |
| PCI/CABG | 0.43 | 0.30–0.61 | <0.001 | 0.64 | 0.39–1.06 | 0.084 |
| DM | 1.39 | 1.12–1.72 | 0.003 | 1.48 | 1.10–1.98 | 0.009 |
| Heart failure | 2.98 | 2.33–3.80 | <0.001 | 2.06 | 1.46–2.90 | <0.001 |
| HA | 1.29 | 0.97–1.72 | 0.077 | 0.85 | 0.60–1.19 | 0.344 |
| CKD | 1.25 | 1.00–1.56 | 0.045 | 1.39 | 1.06–1.84 | 0.019 |
| Physical activity | 1.03 | 0.82–1.29 | 0.813 | 1.02 | 0.78–1.34 | 0.860 |
| BMI ≥ 30 | 1.43 | 1.14–1.78 | 0.002 | 1.21 | 0.92–1.59 | 0.175 |
| hs CRP >5 mg/L | 0.89 | 0.67–1.19 | 0.438 | 0.83 | 0.59–1.15 | 0.260 |
| NT pro-BNP > 125 pg/mL | 1.95 | 1.44–2.64 | <0.001 | 2.37 | 1.493.76 | <0.001 |
| Factor | Male Gender | CKD | DM | Age ≥ 75 | ICS/TIA | Heart Failure | |
|---|---|---|---|---|---|---|---|
| Sample/Draw 1 | OR | 2.39 | 1.78 | 1.34 | 2.66 | 1.70 | 1.63 |
| 95% CI | 1.68–3.38 | 1.24–2.55 | 0.93–1.92 | 1.83–3.87 | 1.07–2.71 | 1.09–2.43 | |
| P | 0.020 | 0.002 | 0.115 | <0.001 | 0.025 | 0.016 | |
| Sample/Draw 2 | OR | 1.54 | 1.39 | 1.39 | 3.30 | 1.57 | 2.02 |
| 95% CI | 1.07–2.21 | 0.95–2.05 | 0.95–2.04 | 2.21–4.92 | 0.96–2.57 | 1.34–3.05 | |
| P | <0.001 | 0.092 | 0.093 | <0.001 | 0.073 | 0.001 | |
| Sample/Draw 3 | OR | 2.13 | 1.31 | 1.29 | 3.10 | 1.94 | 2.10 |
| 95% CI | 1.48–3.06 | 0.89–1.93 | 0.88–1.89 | 2.10–4.57 | 1.22–3.09 | 1.40–3.15 | |
| P | <0.001 | 0.171 | 0.197 | <0.001 | 0.005 | <0.001 | |
| Sample/Draw 4 | OR | 1.99 | 1.88 | 1.37 | 2.34 | 1.98 | 1.85 |
| 95% CI | 1.41–2.81 | 1.31–2.69 | 0.96–1.96 | 1.62–3.38 | 1.27–3.10 | 1.26–2.72 | |
| P | <0.001 | 0.001 | 0.086 | <0.001 | 0.003 | 0.002 | |
| Sample/Draw 5 | OR | 2.50 | 1.43 | 1.51 | 2.83 | 1.76 | 1.88 |
| 95% CI | 1.75–3.59 | 0.98–2.08 | 1.04–2.20 | 1.93–4.15 | 1.09–2.84 | 1.25–2.83 | |
| P | <0.001 | 0.066 | 0.030 | <0.001 | 0.021 | 0.002 | |
| Abbreviation | M Male gender | R Renal failure | D Diabetes | A Age | S Stroke | H Heart failure | |
| Score | 2 | 1 | 1 | 3 | 2 | 1 | |
| Sample/Draw 1 | Sample/Draw 2 | Sample/Draw 3 | Sample/Draw 4 | Sample/Draw 5 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Derivation Cohort | Validation Cohort | Derivation Cohort | Validation Cohort | Derivation Cohort | Validation Cohort | Derivation Cohort | Validation Cohort | Derivation Cohort | Validation Cohort | |
| Sensitivity (%) | 52.2 | 60.9 | 59.9 | 53.8 | 62.7 | 48.0 | 58.3 | 54.1 | 57.9 | 56.9 |
| Specificity (%) | 74.0 | 77.2 | 74.9 | 75.3 | 75.9 | 73.2 | 735.7 | 77.4 | 75.7 | 73.7 |
| Positive predictive value (%) | 17.2 | 18.1 | 16.9 | 18.9 | 19.0 | 143.7 | 18.2 | 15.4 | 18.3 | 16.1 |
| Negative predictive value (%) | 94.6 | 96.0 | 95.6 | 93.8 | 95.8 | 93.6 | 94.6 | 95.7 | 95.0 | 95.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitrega, K.; Lip, G.Y.H.; Sredniawa, B.; Sokal, A.; Streb, W.; Przyludzki, K.; Zdrojewski, T.; Wierucki, L.; Rutkowski, M.; Bandosz, P.; et al. Predicting Silent Atrial Fibrillation in the Elderly: A Report from the NOMED-AF Cross-Sectional Study. J. Clin. Med. 2021, 10, 2321. https://doi.org/10.3390/jcm10112321
Mitrega K, Lip GYH, Sredniawa B, Sokal A, Streb W, Przyludzki K, Zdrojewski T, Wierucki L, Rutkowski M, Bandosz P, et al. Predicting Silent Atrial Fibrillation in the Elderly: A Report from the NOMED-AF Cross-Sectional Study. Journal of Clinical Medicine. 2021; 10(11):2321. https://doi.org/10.3390/jcm10112321
Chicago/Turabian StyleMitrega, Katarzyna, Gregory Y. H. Lip, Beata Sredniawa, Adam Sokal, Witold Streb, Karol Przyludzki, Tomasz Zdrojewski, Lukasz Wierucki, Marcin Rutkowski, Piotr Bandosz, and et al. 2021. "Predicting Silent Atrial Fibrillation in the Elderly: A Report from the NOMED-AF Cross-Sectional Study" Journal of Clinical Medicine 10, no. 11: 2321. https://doi.org/10.3390/jcm10112321