
Abstract
People with mental illness around the world continue to suffer from stigmatization and limited care. Previous studies utilizing self-report questionnaires indicate that many medical students regard clinical work with psychiatric patients as unappealing, while the professionalism literature has documented a general decline in students’ capacity for empathy over the course of medical school. Through in-depth interviews, this study attempts to better understand the formation of medical students’ perceptions of psychiatry and the implications of that process for a more general understanding of the impact of emotionally-laden experiences on medical students’ capacity for empathy. Forty-seven fourth-year medical students who had expressed interest or performed well in psychiatry were asked a series of questions to elicit their perceptions of the field of psychiatry. Interview transcripts were systematically coded using content analysis and principles of grounded theory. Stigma, stereotypes, and stressfully intense emotional reactions seemed to adversely affect the students’ expected satisfaction from and willingness to care for the mentally ill, despite enjoying psychiatry’s intellectual content and the opportunity to develop in-depth relationships with patients. Teaching faculty need to directly address the stigma and stereotypes that surround mental illness and actively help medical students cope with the stress that they report experiencing during their psychiatry clerkship in order to improve the recognition and treatment of psychiatric illness by newly graduating physicians. More generally, the relationships that we identify among stress, stigmatization, and stereotyping along an empathic spectrum suggest that increased attention should be paid to the stress that empathy can entail. This perspective may allow for the creation of similarly targeted interventions throughout the medical school curriculum to counteract the decline in empathy, the so-called “hardening of the heart,” associated with physician-training worldwide.
Similar content being viewed by others

Introduction
Stigma towards psychiatric patients continues to plague the field of medicine, and misinformation about mental illness remains a barrier to appropriate treatment worldwide. Many patients suffer in silence, reluctant to come forward with a psychiatric complaint (US DHHS 2003). Many physicians fail to recognize or appropriately address mental illness in their patients (Ormel et al. 1990; Rubinow 2006). As a result, extraordinarily common and debilitating conditions such as depression remain untreated, presenting an enormous public health challenge of international dimensions (Wang et al. 2005a, b; World Health Organization 2006; Grace et al. 2005).
Entering medical students oftentimes share their own society’s negative and stereotyped views of psychiatric patients (Feifel et al. 1999; Chew-Graham et al. 2003) and psychiatrists (Fink 1983; Walter 1989; Furnham 1986). While enrolled medical students in the United States find the field intellectually interesting (Cutler et al. 2006), many regard clinical work with psychiatric patients as unappealing (Galka et al. 2005; Martin et al. 2005; Singh et al. 1998; Balon et al. 1999; Sierles et al. 1995; Nielsen et al. 1981) and even stressful (Cutler et al. 2006). Similar observations have been made in many countries around the world (Brockington and Mumford 2002; Malhi et al. 2002; Fischel et al. 2008; Ndetei et al. 2008; Syed et al. 2008; Ay et al. 2006).
These medical student perceptions are important as they relate to the care of psychiatric patients for two reasons. First, most physicians, regardless of specialty, treat many patients with co-existing mental illness. Students who finish medical school without changing their pre-existing views of psychiatry will become practicing physicians who feel unprepared or unwilling to address psychiatric illnesses, thus further perpetuating stigmatization, misinformation, and the resultant limited care. Second, despite a recent stabilization in previous downward trends, the recruitment of medical school graduates into psychiatry remains a concern not only in the U.S. (Rao 2003; Sierles et al. 2003; United States National Resident Matching Program 2006), but also around the world (World Health Organization 2005). Whether or not the field seeks an increase in recruitment, avoidance of a further decline is necessary to maintain talented, well-trained psychiatrists to treat wide-spread mental illness.
Psychiatric educators over the years have offered hypotheses and recommendations to address these ongoing medical student perceptions (Feldmann 2006). The evidence supporting those recommendations has been limited, however, because most previous studies have relied upon self-report questionnaires that provide thought-provoking but unelaborated data. For example, Niedermier et al. (2006) found that students who were initially neutral regarding a psychiatric career became firmly rejecting of it after their psychiatry clerkship despite reporting a positive experience. Cutler et al. (2006) noted that students rated working with psychiatric patients as low in “satisfaction” and high in “stress,” but were unable to specify what those ratings reflected. The design of well-informed educational interventions requires a better understanding of the issues underlying such findings.
Medical student perceptions of psychiatry may also have implications for the broader community of medical educators. Increasing attention has been paid in recent years to professionalism and barriers to the development of empathy among medical students (Newton et al. 2008; Coulehan and Williams 2001). It has been recognized that students are influenced by many experiences beyond the formal medical school curriculum (Hafferty 1998; Hundert 1996), and that attention should be paid to factors underlying students’ outward behavior, such as their attitudes and self-reflective capacities (Hoifodt et al. 2007; Hafferty 2006). Students’ concern that working with psychiatric patients is unsatisfying and stressful could represent an opportunity to shed light on a more general phenomenon: the impact of emotionally-laden experiences on medical students’ developing professionalism, including their capacity for empathy, which has been repeatedly noted to decline over the course of medical school (Newton et al. 2008).
The purpose of this study was to determine: (1) a more detailed and nuanced account of medical students’ perceptions of psychiatry, particularly as those perceptions relate to the perceived stress and satisfaction inherent in working with psychiatric patients; (2) the basis of those perceptions (including formal and informal educational exposures as well as personal experiences) (3) the impact those perceptions have on students’ career decisions and their anticipated future practices; and (4) the implications of the formation of those perceptions for students’ professional development. To that end we conducted and systematically analyzed in-depth interviews of senior medical students.
Methods
Participants
After receiving Institutional Review Board (IRB) approval, we solicited participants from fourth-year students at one large private urban northeastern medical school. Students were invited to participate only if they met one or more of the following criteria: they expressed an interest in psychiatry on a self-report questionnaire from a previous study (Cutler et al. 2006); they expressed interest in psychiatry during their medical school experience by attending a psychiatry club meeting; or they demonstrated an aptitude for psychiatry by performing well during their psychiatry clerkship (i.e., receiving Honors).
One hundred and six eligible students were invited to participate with the incentive of $25 compensation. Written informed consent was obtained from the 47 students who volunteered. Twenty-one participants were female and 26 were male. The median age was 26 years with a range from 22 to 41. Participants’ undergraduate majors were mostly from the natural sciences (n = 31), with some from the humanities (n = 10) and the social sciences (n = 6). Twenty-five students matched in medical fields (e.g., pediatrics, internal medicine, neurology), while the other 22 matched in surgical fields (general surgery, a surgical subspecialty, obstetrics-gynecology). All of these characteristics are representative of the medical school’s overall student population.
Materials and procedure
The principal investigator constructed the interview questions (see Table 1) from previous medical student self-report questionnaire findings (Cutler et al. 2006), as well as from a general review of existing psychiatric education literature (Feifel et al. 1999; Chew-Graham et al. 2003; Fink 1983; Walter 1989; Furnham 1986; Cutler et al. 2006; Galka et al. 2005; Martin et al. 2005; Singh et al. 1998; Balon et al. 1999; Sierles and Taylor 1995; Nielsen and Eaton 1981). Two faculty members in the department of psychiatry conducted the interviews shortly after students received notification of their residency matches. The interview format was semi-structured, allowing interviewers to clarify student responses. Interviews lasted approximately sixty minutes. Each interviewer took detailed hand-written notes. The interviewers’ extensive psychotherapy process note-taking experience allowed the creation of accurate, frequently verbatim transcripts from these notes (Wolfson and Sampson 1976; Bailey 2000). In close collaboration with the faculty interviewers, three research team members transcribed the notes.
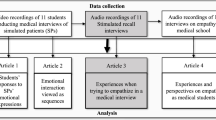
Analysis
We adhered to the established qualitative methodology of grounded theory to identify the salient themes as they emerged from our data (Strauss and Corbin 1998; Glaser 1992). This methodology has been widely used in social science and public health research, and has more recently been applied in the medical education setting (Ginsburg et al. 2002). First, two randomly chosen transcripts were reviewed in order to begin to identify emergent themes. During this initial review and throughout the process, the research team (one attending psychiatrist, two senior psychiatry residents, and one research assistant) worked both individually and as a group; disagreements were resolved by discussion.
Several initial versions of the coding structure were developed, applied to a few additional transcripts, and then rejected because of excessive complexity or over-simplification. The team agreed upon an initial coding structure that was successfully applied to five additional transcripts, such that each idea or “coherent unit” could be placed into one of the thematic categories. A “coherent unit” was defined as a section of text ranging from one to multiple sentences that expressed a single idea. While it was agreed that transcript sections could be “double-coded”—or even occasionally “triple-coded”—if more than one category was applicable, in practice most of the duplicate coding became unnecessary as the coding structure was refined.
As additional transcripts in sets of three to five were analyzed, categories evolved and the coding structure was further revised, subdividing the main categories to define more succinctly the emerging themes. Figure 1 illustrates an example of this process. A saturation point was reached when no new thematic categories appeared (after 23 transcripts had been coded). In other words, the categories comprising the coding structure were exhaustive and, for the most part, mutually exclusive.

Evolution of coding structure. An initial coding structure based on analysis of several transcripts placed the coded statement “psychiatry is too open-ended for me” in the category “attitudes” (stage I). After more transcripts were analyzed, the concept of “attitudes” became too non-specific. Statements coded under “attitudes” were moved to already existing categories in the coding structure or to newly created or refined categories. In this example,“personality” was refined to “preferences” and the statement “psychiatry is too open-ended for me” was coded as “diagnostic subjectivity,” better reflecting the sentiment evident in this and other statements about students’ perceptions of the nature of psychiatric diagnosis
The final coding structure (Table 2) was then systematically applied to each of the forty-seven transcripts. The coding results were entered into NVivo qualitative-data-analysis software (Kelle 1995) by one of the team members. The output of the NVivo analysis provides grouping of the coded elements, permitting an integration of themes across all respondents. Upon review of the NVivo analysis output, the research team decided on one further step in the coding process: assignment of a ‘positive,’ ‘negative,’ or ‘indeterminate’ valence to reflect the emotional tone of each unit of coded text. For example, statements reflecting respect, satisfaction, and interest received positive valences, whereas statements that were critical, frustrated, and dissatisfied were assigned negative valences. The indeterminate valence was specifically assigned to statements of ambiguous emotional meaning. The valence assignments were made section by section of the NVivo output, referring back to the original interview transcripts as necessary. Finally, we tallied the comments for each section of the coding outline to provide a quantitative assessment of the students’ perceptions.
Results
The frequency of occurrence of coded comments is summarized in Table 3. Multiple discussions with the entire research team in accordance with the guidelines of grounded theory resulted in a synthesis of the main themes that emerged from this data. Figure 2 illustrates a conceptual framework for describing these results: Medical School Experience; Psychiatric Practice; and Relevance of Psychiatry to Future Practice.

Conceptual framework derived from the coding structure. The results are best organized and described within the 3 over-arching components of this conceptual framework as illustrated on the right-side of the figure. The framework was developed by the entire research team as a result of analyzing the final data set, which consisted of the coded and grouped themes with their associated valences and frequency counts. * These thematic categories had relatively fewer coded comments (see Table 3) and are not specifically described in the section ‘Results’
Medical school experience
Students made generally positive comments regarding the pre-clinical psychiatry curriculum. They stated that the courses were “great” and expressed enthusiasm for learning the “very interesting” material, which they “loved.” Negative comments focused on the structure of the courses, rather than the material itself: for example, the preceptor wasn’t “very active” or “interesting,” or the discussion group was “too big.”
In contrast, the clinical curriculum and—more specifically—the students’ interactions with psychiatric patients, elicited many more negative comments. In fact, 12 out of the total sample of 47 students (26%) reported that an initially positive response to psychiatry became negative after their clinical clerkships. The following comment exemplifies this shift in attitude: “First and second year I thought maybe psychiatry, really interested, able to think the way psychiatrists do…[during the clerkship] uncomfortable with the patients…didn’t enjoy interacting with patients, felt like a chore to see them.”
While only 7 students (15%) made general comments associating the field of psychiatry with high levels of stress, many respondents described their actual clinical psychiatric experiences to be stressful. In particular, 15 students (32%) described patient interactions as “disturbing” and 9 students (19%) expressed concerns about the personal impact that working with psychiatric patients entailed, using such descriptive terms as “emotionally draining,” “overwhelming,” and “overly identified.” The following comment, made by a student who “brought experiences home” during the psychiatry clerkship and was left with “mentally disturbing images,” captures what seemed to be a prevalent concern: “Working with ‘crazies’ will make you ‘crazy’.” In addition, 24 students (51%) complained that psychiatric patients are treatment-refractory and “frustrating,” eliciting feelings of helplessness in the respondents.
Students also seemed to have mixed feelings with regard to their psychiatry clerkship in general: many students made both positive and negative comments (concurrently) regarding the clinical curriculum and, furthermore, the number of comments in the indeterminate category was substantial (see Table 1). The following comments seem to capture this ambivalence: “… the most formative and distressing rotation was psychiatry. Other rotations were more business as usual.” “[Psychiatry provided] a lot of patient contact; what fascinated me most seemed like [what I would have] the least impact on.” These students echo a common theme: psychiatric patients are fascinating, but also stressful and frustrating.
Positive comments regarding students’ experiences with psychiatric patients tended to focus on the work being interesting and fun, and the relationships that students forged with their patients on the psychiatry service were viewed as a draw to the field. Respondents noted the opportunity to have longer-term, more in-depth relationships, and to spend more time with patients. Clinical experiences with “appreciable” and even “impressive” treatment results were “very rewarding.”
Sixteen students (34%) reported positive experiences with the psychiatrists with whom they came into contact in medical school, describing them as effective role models who were generally easy to get along with, “caring,” “self-reflecting, very cerebral, patient,” “friendly, approachable, without seeming stressed,” and particularly satisfied as compared with physicians in other fields. One student went so far as to say “[I] never talked to a psychiatrist with regrets!”
Ten students (21%) made negative comments about faculty and residents; these tended to be overly generalized and seemed to reflect stereotyping of psychiatrists. “A lot of people go into psychiatry with a lot of their own psychopathology.” “They are concerned about their own selves, being broken in their head.” In addition, the perceived status of psychiatry in the medical community was described as a uniformly negative characteristic of the field. Respondents cited a “lack of respect among the medical community” and “disparaging comments about psychiatry” made by residents and faculty in other fields, and even being ridiculed when suggesting the usefulness of a psychiatric consultation.
Psychiatric practice
Many respondents described their families as having negative, stigmatizing attitudes toward the field (coded as the category values), although most of those students denied that their families’ views had a significant impact on their career choices. Some students reported that their families regarded becoming a psychiatrist as “wasted time” or signifying that they were “not a real doctor”; others’ friends expressed the opinion that “everyone in psychiatry is crazy themselves.”
The lifestyle of psychiatrists was regarded as advantageous by 13 students (28%) who indicated that the logistics of the clinical work (hours, workload) appeared manageable, offering flexibility and “a lot of freedom” with less time spent in the hospital and more control over work hours. In addition, they perceived “a niche for everybody” in which one could “work with sick patients or have an eastside [i.e., upper middle class] practice.” Several students observed that the field was particularly good for women with regard to having a family. Negative comments tended to focus on the limitations that health insurance imposes on the practice of psychiatry. Specifically, students believed that psychiatrists would have to focus more on medication management than on psychotherapy. In addition, a number of students admitted that they regarded the earning power of psychiatrists as being limited, but they denied the impact of this financial issue on their career choices.
Many respondents described two characteristics of the day-to-day work of psychiatry that were felt to be incompatible with their personal preferences. First, 10 students (21%) reported that they liked to work with their hands and noted that they would be unable to do so in psychiatry. “[There is] something about touching a patient, listening with a stethoscope, looking at a throat—an intimacy that strengthens the relationship with the doctor.” “In high school I was artistic and liked working with my hands. I decided that I wanted to be a surgeon. Otherwise, I wouldn’t have wanted to be a doctor.” Second, 12 students (26%) felt that psychiatry’s lack of immediate gratification would be problematic. “I’m impatient, I like tangible and immediate gratification and psychiatry does not offer this.” “Psychiatry was drawn out. I like to finish a book in one weekend.”
Relevance of psychiatry to future practice
Finally, nearly all participants felt that their experiences in psychiatry would be relevant to their future practices, regardless of specialty. They specifically appreciated their ability to recognize psychiatric disorders in their patients and to be aware of indications for psychiatric consultation and referral. Students described valuable attitudinal lessons learned from their psychiatric education, including the realization that mental illness is common and is “real pathology” accompanied by genuine suffering; increased optimism regarding the effectiveness of treatment; and legitimization of the profession.
Discussion
Our data present us with some sobering observations: stress, stigma, and stereotypes appear to adversely affect medical students’ expected satisfaction from and willingness to work with psychiatric patients. This impact occurred despite students finding (1) their pre-clinical exposure to psychiatry appealing, (2) the in-depth relationships that they developed with psychiatric patients engaging, and (3) the opportunity to observe psychiatric patients’ status improve impressive. Our results do not indicate that students observed psychiatric faculty and residents with whom they worked as “stressed” (Cutler et al. 2006), which was one of our initial hypotheses. Instead, the students reported that they themselves experienced stress during their psychiatry clerkship. This particular explanation regarding students’ perceptions of psychiatry as a stressful field has not before been cogently identified. While Kris (1986) reported 20 years ago that nearly one quarter of medical students seeking mental health service consultations with her did so during their psychiatry clerkship, stress specific to students’ clinical psychiatric exposure has been neglected in the subsequent literature.
Our finding of students’ experience of working with psychiatric patients as stressful is of interest to the medical and health science education community at large in light of the observation that medical students tend to experience a dramatic decline in empathy during their clinical exposure (Newton et al. 2008). Our data highlight stress as it relates to empathizing with hospitalized psychiatric patients. While empathizing with severely disorganized and emotionally labile patients may be particularly stressful for students, the conflicts and stress inherent in empathic identification with ill patients in any specialty may play a crucial role in the overall decline in empathy during medical training. Furthermore, this stress may be an important factor more broadly in the development of negative attitudes toward certain patient types (Griffith and Wilson 2001). Interestingly, educators’ lack of attention to this barrier to empathy may reflect in parallel their own empathic failure, in order to protect themselves from re-experiencing the anxiety and discomfort of their trainees. This self-protective response has been described by Hundert (1996) with regard to more senior trainees’ apparent lack of empathy for their more junior colleagues’ stressful experiences.
While it has been recognized that students struggle to reconcile their empathic feelings with the demands of patient care (Branch et al. 1993), much of the medical professionalism literature tends to focus on the medical culture (Stern and Papadakis 2006) and behavioral recommendations that fail to fully recognize the stress that empathy can entail (Miller and Schmidt 1999; Larson and Yao 2005). The concept of “compassion fatigue” (Figley 1995; Huggard 2003) comes closest to such recognition, but it has been reserved mainly for describing the stress that health professionals experience when empathizing with trauma victims. More broadly, the stigmatization and stereotyping of certain types of patients may be related to the particular stress that empathizing with them involves. While stigmatization and stereotyping may be regarded as barriers to empathy, it may be more accurate to regard them as lying at one end of an empathic spectrum. This empathic spectrum can be conceptualized as placing over-identification at one extreme, in which the physician moves painfully too close to the patient’s experience, and disengaged lack of empathy at the other extreme. Thus, when confronted with a suffering patient, a physician might choose to distance him or herself by categorizing the patient in a stigmatized and stereotyped manner, rather than risking the stress of over-identification that lies at the other end of the empathic spectrum.
Our data indicate that stigmatization and stereotyping of psychiatric patients by medical students arise in part from the influence of others: family members and friends, who reflect the views held by society at large; and non-psychiatric physicians, who, in reflecting those societal views as well as their own medical training, represent the impact of the “hidden” curriculum on our student subjects. Furthermore, stigmatization and stereotyping persist not just with regard to psychiatric patients, but also with regard to psychiatrists. We found that psychiatry’s perceived low status among students’ families, as well as among the medical school faculty and housestaff, were notable and could be considerable impediments to all students’ attitudes towards patients with psychiatric illness as well as for those considering specializing in psychiatry.
Implications
We believe that it is essential to discredit the persistent notion that ‘working with crazies will make you crazy:’ while working with psychotic and depressed patients entails real stress, students should be educated in a setting where they feel empathically supported—not overwhelmed—so that the stress is not magnified. Psychiatric educators should actively help students cope with the stress that they experience during their psychiatry clerkship and directly address the stigma and stereotypes that surround psychiatry. For example, in our own curriculum, during a case-based discussion of depression we now highlight students’ reluctance to recommend prescribing anti-depressants in comparison with treatments for less stigmatized conditions such as hypertension. The class discussion illustrates the subtle ways in which stigma affects perceptions and practice. Interventions such as these could have beneficial effects on future non-psychiatric physicians’ recognition and care of their patients’ psychiatric issues, as well as on students considering pursuit of a psychiatric career.
We believe that our proposed understanding of stress and empathy has wide-ranging curricular implications beyond the confines of psychiatry. In considering how to enhance medical students’ professional development in general and empathic skills in particular, we recommend that increased attention be paid to the forces contributing to a decline in empathy not just over medical students’ training, but for all physicians. Simply attributing the decline in empathy observed during medical school to the pressures of the medical culture, the presence of unempathic role models, and other interpersonal issues (Haidet and Stein 2006), overlooks the underlying question as to why faculty and housestaff have become less empathic. Perhaps it is time for health professionals and educators to acknowledge that empathizing with extremely ill patients, whether psychiatric or not, can frequently be stressful. All health professionals, not just trainees, might then acknowledge the on-going struggle to keep our equilibrium and function at our best in caring for our patients and in taking care of ourselves. Faculty and residents might then model a professional stance that balances empathic identification with appropriate professional distance by providing not only their patients but also their students with empathy and emotional support.
Interestingly, the processes limiting health care professionals’ ability to be empathic may be even more basic to human behavior than we, as medical and health profession educators, recognize. For example, as part of normal social functioning, it has been observed that adults regularly and automatically mimic other people’s emotional facial expressions (McIntosh et al. 2006). Furthermore, current research into the basic neuroscience of empathy suggests that brain cells, known as mirror neurons, respond similarly when we experience an emotion, such as ‘disgust,’ and when we witness someone else looking ‘disgusted’ (Wicker et al. 2003). Finally, empathy is not ‘all-or-none’ and is not static; an individual’s capacity for empathy is recognized to be influenced by cognitive processing (Lamm et al. 2007) and imitation (Iacoboni 2005). Thus, for physician-educators and medical students alike, these basic human processes may unknowingly contribute to not only the ‘stress’ of working with severely ill patients but also to the underlying power of the informal (Hundert 1996) or so-called “hidden”curriculum (Hafferty 2006). We propose that preceptors and supervisors throughout medical and health science education play a key role mediating medical students’ abilities to process strong emotional reactions to difficult situations that otherwise can result in stigmatizing statements like “Working with crazies will make you crazy.” Recognition of the unconscious nature of these types of reactions—whether student- or instructor-initiated—is necessary to begin to address them.
Limitations
We acknowledge the boundaries of our methodology and interpretations. First, the presence of faculty interviewers may have made the students reluctant to be fully open and honest in their responses. Even when grades are not at stake, students may have been unwilling to share specific comments about faculty with whom they rotated. On the other hand, the interviews were conducted when the students had completed nearly all of their academic requirements, certainly all within the department of psychiatry; they were within a month or two of graduation; and they did seem comfortable in discussing many negative opinions relating to psychiatry. Second, the timing of the interviews soon before the students’ first year of residency training may not have been most conducive to introspective observations since graduating students tend to be filled with anticipatory anxiety: that is, our respondents may have felt inclined to convince themselves that their career choices were clearly best for them. At a less anxiety-provoking time, students’ views might be characterized by more ambivalence. Third, this study is confined to one medical school, and thus its results may not generalize across institutions. To address this issue, a more focused self-report questionnaire that builds from the richness of the themes identified in this analysis could be developed and distributed to medical schools with a range of student populations and educational experiences to insure validity and reliability. Finally, there is a lack of empirical research supporting the relationships that we have drawn between the neuroscience of empathy and medical education. Further research is needed to address these conjectures in a rigorous fashion.
Conclusion
The relationships that we have described among stress, stigmatization, and stereotyping along an empathic spectrum suggest that increased attention should be paid to the stress that empathy can entail. Our data indicate that medical students associate mental illness with stress, stigma, and stereotypes even after four years of medical education. This finding is likely to exist to some extent across medical curriculums worldwide. If medical students are not given the tools to metabolize their reactions to psychiatric patients, then it seems reasonable to presume that in the future as practicing physicians they will experience reactions similar to those reported by our participants, thus perpetuating the stress, stigmatization, and stereotyping associated with psychiatry and mental illness. Therefore, within the field of psychiatric education, faculty should actively help students identify and cope with the stress that they report experiencing as they work with psychiatric patients. Such interventions will hopefully improve the recognition and care of patients with mental illness by all newly graduating physicians. More generally, our finding that students experience working with psychiatric patients as stressful is of interest to all medical educators in light of the dramatic decline in empathy that has been observed over the course of medical school. The conflicts and stress inherent in empathic identification with ill patients in any specialty may play a crucial role in this overall decline in empathy. This perspective may allow for the creation of similarly targeted interventions throughout the medical school curriculum to address and perhaps begin to soften the “hardening of the heart” observed in medical education worldwide.
References
Ay, P., Save, D., & Fidanoglu, O. (2006). Does stigma concerning mental disorders differ through medical education? A survey among medical students in Istanbul. Social Psychiatry and Psychiatric Epidemiology, 41, 63–67. doi:10.1007/s00127-005-0994-y.
Bailey, K. E. (2000). Comparison of verbatim transcripts and psychoanalytic process notes for emotion tone, abstraction, and referential activity using computerized text analysis methods. Dissertation Abstracts International, Section B, The Sciences and Engineering, 61, 3269.
Balon, R., Franchini, G. R., Freeman, P. S., Hassenfeld, I. N., Keshavan, M. S., & Yoder, E. (1999). Medical students’ attitudes and views of psychiatry: 15 Years later. Academic Psychiatry, 23, 30–36.
Branch, W., Pels, R. J., Lawrence, R. S., & Arky, R. (1993). Becoming a doctor–critical-incident reports from third-year medical students. The New England Journal of Medicine, 329, 1130–1132. doi:10.1056/NEJM199310073291518.
Brockington, I., & Mumford, D. (2002). Recruitment into psychiatry. British Journal of Psychiatry, 180, 307–312. doi:10.1192/bjp.180.4.307.
Chew-Graham, C. A., Rogers, A., & Yassin, N. (2003). “I wouldn’t want it on my CV or their records”: Medical students’ experiences of help-seeking for mental health problems. Medical Education, 37, 873–880. doi:10.1046/j.1365-2923.2003.01627.x.
Coulehan, J., & Williams, P. C. (2001). Vanquishing virtue: The impact of medical education. Academic Medicine, 76, 598–605.
Cutler, J. L., Alspector, S. L., Harding, K. J., Wright, L. A., & Graham, M. J. (2006). Medical students’ perceptions of psychiatry as a career choice. Academic Psychiatry, 30, 144–149. doi:10.1176/appi.ap.30.2.144.
Feifel, D., Moutier, C. Y., & Swerdlow, N. R. (1999). Attitudes toward psychiatry as a prospective career among students entering medical school. American Journal of Psychiatry, 156, 1397–1402.
Feldmann, T. B. (2006). Medical students’ attitudes toward psychiatry and mental disorders. Academic Psychiatry, 29, 354–356. doi:10.1176/appi.ap.29.4.354.
Figley, C. R. (1995). Compassion fatigue. New York: Brunner/Mazel.
Fink, P. J. (1983). The enigma of stigma and its relation to psychiatric education. Psychiatric Annals, 13, 669–690.
Fischel, T., Manna, H., Krivoy, A., Lewis, M., & Weizman, A. (2008). Does a clerkship in psychiatry contribute to changing medical students’ attitudes towards psychiatry? Academic Psychiatry, 32, 147–153. doi:10.1176/appi.ap.32.2.147.
Furnham, A. F. (1986). Medical students’ beliefs about nine different specialties. British Medical Journal, 293, 1607–1610.
Galka, S. W., Perkins, D. V., Butler, N., Griffith, D. A., Schmetzer, A. D., Avirrappattu, G., et al. (2005). Medical students’ attitudes toward mental disorders before and after a psychiatric rotation. Academic Psychiatry, 29, 357–361. doi:10.1176/appi.ap.29.4.357.
Ginsburg, S., Regehr, G., Stern, D., & Lingard, L. (2002). The anatomy of the professional lapse: Bridging the gap between traditional frameworks and students’ perceptions. Academic Medicine, 77, 516–522. doi:10.1097/00001888-200206000-00007.
Glaser, B. G. (1992). Basics of grounded theory analysis. Mill Valley, CA: Sociology Press.
Grace, S. L., Abbey, S. E., Kapral, M. K., Fang, J., Nolan, R. P., & Steward, D. E. (2005). Effect of depression on five-year mortality after an acute coronary syndrome. American Journal of Cardiology, 96, 1179–1185. doi:10.1016/j.amjcard.2005.06.052.
Griffith, C. H., & Wilson, J. F. (2001). The loss of student idealism in the 3rd-year clinical clerkships. Evaluation and the Health Professions, 24, 61–71. doi:10.1177/01632780122034795.
Hafferty, F. W. (1998). Beyond curriculum reform: Confronting medicine’s hidden curriculum. Academic Medicine, 73, 403–407. doi:10.1097/00001888-199804000-00013.
Hafferty, F. W. (2006). Professionalism–the next wave. The New England Journal of Medicine, 355, 2151–2152. doi:10.1056/NEJMe068217.
Haidet, P., & Stein, H. F. (2006). The role of the student-teacher relationship in the formation of physicians: The hidden curriculum as process. Journal of General Internal Medicine, 21(supplement 1), S16–S20. doi:10.1111/j.1525-1497.2006.00304.x.
Hoifodt, T. S., Olstad, R., & Sexton, H. (2007). Developing psychiatric competence during medical education and internship: Contributing factors. Advances in Health Sciences Education, 12, 457–473. doi:10.1007/s10459-006-9010-x.
Huggard, P. (2003). Compassion fatigue: How much can I give? Medical Education, 37, 163–164. doi:10.1046/j.1365-2923.2003.01414.x.
Hundert, E. M. (1996). Characteristics of the informal curriculum and trainees’ ethical choices. Academic Medicine, 71, 624–633. doi:10.1097/00001888-199606000-00014.
Iacoboni, M. (2005). Understanding others: Imitation, language, empathy. In S. Hurley & N. Chater (Eds.), Perspectives on imitation: From neuroscience to social science (Vol. 1). Cambridge, MA: MIT Press.
Kelle, U. (1995). Computer-aided qualitative data analysis: Theory, methods, and practice. Thousand Oaks, CA: Sage Publications.
Kris, K. (1986). Distress precipitated by psychiatric training among medical students. American Journal of Psychiatry, 143, 1432–1435.
Lamm, C., Nusbaum, H. C., Meltzoff, A. N., & Decety, J. (2007). What are you feeling? Using functional magnetic resonance imaging to assess the modulation of sensory and affective responses during empathy for pain. PLoS One, 2(12), e1292. doi:10.1371/journal.pone.0001292.
Larson, E. B., & Yao, X. (2005). Clinical empathy as emotional labor in the patient-physician relationship. Journal of the American Medical Association, 293, 1100–1106. doi:10.1001/jama.293.9.1100.
Malhi, G. S., Parker, G. B., Parker, K., Kirby, D. C., Boyce, P., Yellowlees, P., et al. (2002). Shrinking away from psychiatry? A survey of Australian medical students’ interest in psychiatry. Australian and New Zealand Journal of Psychiatry, 36, 416–423. doi:10.1046/j.1440-1614.2001.00991.x.
Martin, V. L., Bennett, D. S., & Pitale, M. (2005). Medical students’ perceptions of child psychiatry pre- and post-psychiatry clerkship. Academic Psychiatry, 29, 362–366. doi:10.1176/appi.ap.29.4.362.
McIntosh, D. N., Reichmann-Decker, A., Winkielman, P., & Wilbarger, J. L. (2006). When the social mirror breaks: Deficits in automatic, but not voluntary, mimicry of emotional facial expressions in autism. Developmental Science, 3, 295–302. doi:10.1111/j.1467-7687.2006.00492.x.
Miller, S. Z., & Schmidt, H. J. (1999). The habit of humanism: A framework for making humanistic care a reflexive clinical skill. Academic Medicine, 74, 800–803.
Ndetei, D. M., Khasakhala, L., Ongecha-Owuor, F., Kuria, M., Mutiso, V., Syanda, J., et al. (2008). Attitudes toward psychiatry: A survey of medical students at the University of Nairobi, Kenya. Academic Psychiatry, 32, 154–159. doi:10.1176/appi.ap.32.2.154.
Newton, B. W., Barber, L., Clardy, J., Cleveland, E., & O’Sullivan, P. (2008). Is there hardening of the heart during medical school? Academic Medicine, 30, 136–143.
Niedermier, J. A., Bornstein, R., & Brandemihl, A. (2006). The junior medical student psychiatry clerkship: Curriculum, attitudes, and test performance. Academic Psychiatry, 30, 136–143. doi:10.1176/appi.ap.30.2.136.
Nielsen, A. C., & Eaton, J. S. (1981). Medical students’ attitudes about psychiatry: Implication for psychiatric recruitment. Archives of General Psychiatry, 38, 1144–1154.
Ormel, J., Van Den Brink, W., Koeter, M. W., Giel, R., Van Der Meer, K., Van De Willige, G., et al. (1990). Recognition, management and outcome of psychological disorders in primary care: A naturalistic follow-up study. Psychological Medicine, 20, 909–923.
Rao, N. R. (2003). Psychiatric workforce: Past legacies, current dilemmas, and future prospects. Academic Psychiatry, 27, 238–240. doi:10.1176/appi.ap.27.4.238.
Rubinow, D. R. (2006). Treatment strategies after SSRI failure–Good news and bad news. New England Journal of Medicine, 354, 1305–1307. doi:10.1056/NEJMe068029.
Sierles, F. S., & Taylor, M. A. (1995). Decline of U.S. medical student career choice of psychiatry and what to do about it. American Journal of Psychiatry, 152, 1416–1425.
Sierles, F. S., Yager, J., & Weissman, S. H. (2003). Recruitment of U.S. graduates into psychiatry: Reasons for optimism, sources of concern. Academic Psychiatry, 27, 252–259. doi:10.1176/appi.ap.27.4.252.
Singh, S. P., Baxter, H., Standen, P., & Duggan, C. (1998). Changing the attitudes of “tomorrow’s doctors” towards mental illness and psychiatry: A comparison of two teaching methods. Medical Education, 32, 115–120. doi:10.1046/j.1365-2923.1998.00162.x.
Stern, D. T., & Papadakis, M. (2006). The developing physician–becoming a professional. The New England Journal of Medicine, 355, 1794–1799. doi:10.1056/NEJMra054783.
Strauss, A. L., & Corbin, J. (1998). Basics of qualitative research: Techniques and procedures for developing grounded theory (2nd ed.). Thousand Oaks, CA: Sage Publications.
Syed, W. U., Siddiqui, M. N., Dogar, I., Hamrani, M. M., Yousafzai, A. W., & Zuberi, S. (2008). Attitudes of Pakistani medical students towards psychiatry as a prospective career: A survey. Academic Psychiatry, 32, 160–164. doi:10.1176/appi.ap.32.2.160.
United States Department of Health and Human Services. (2003). President’s new freedom commission on mental health, achieving the promise: Transforming mental health care in America. Final Report. Pub. No. SMA-03-3832. Rockville, MD. Retrieved from http://www.mentalhealthcommission.gov/reports/FinalReport/FullReport.htm. Accessed August 2007.
United States National Resident Matching Program. (2006). National resident matching program results and data. Washington, DC.
Walter, G. (1989). The stereotype of the mad psychiatrist. Australian and New Zealand Journal of Psychiatry, 23, 547–554. doi:10.3109/00048678909062624.
Wang, P. S., Berglund, P., Olfson, M., Pincus, H. A., Wells, K. B., & Kessler, R. C. (2005a). Failure and delay in initial treatment contact after first onset of mental disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62, 603–613. doi:10.1001/archpsyc.62.6.603.
Wang, P. S., Lane, M., Olfson, M., Pincus, H. A., Wells, K. B., & Kessler, R. C. (2005b). Twelve-month use of mental health services in the United States: Results from the National Comorbidity Survey Replication. Archives of General Psychiatry, 62, 629–640. doi:10.1001/archpsyc.62.6.629.
Wicker, B., Keysers, C., Plailly, J., Royet, J. P., Gallese, V., & Rizzolatti, G. (2003). Both of us disgusted in my insula: The common neural basis of seeing and feeling disgust. Neuron, 40, 655–664. doi:10.1016/S0896-6273(03)00679-2.
Wolfson, A., & Sampson, H. (1976). A comparison of process notes and tape recordings: Implications for therapy research. Archives of General Psychiatry, 33, 558–563.
World Health Organization. (2005). Mental health atlas 2005. Available at http://www.who.int/mental_health/evidence/atlas/. Accessed April 2008.
World Health Organization. (2006). Depression. Geneva, Switzerland. Retrieved from http://www.who.int/mental_health/management/depression/definition/en. Accessed August 2007.
Acknowledgements
The authors would like to acknowledge the assistance of Drs. Ronald Rieder and Eric Marcus with study design and Dr. Lucy Epstein with conceptualizing the discussion and implications. They thank Drs. Lisa Mellman and Reed Perron for their careful readings of earlier versions of the manuscript. They acknowledge the insightful comments of the anonymous reviewers, which improved the manuscript significantly. This work was supported by a grant from the Frontier Fund.
Author information
Authors and Affiliations
Corresponding author
Additional information
Previous presentation: The contents of this paper have been presented in part at the Annual Meeting of the Association of Directors of Medical Student Education in Psychiatry in Santa Fe, New Mexico, June 15–17, 2000; the Research in Medical Education (RIME) Conference, part of the Association of American Medical Colleges (AAMC) Annual Meeting in Washington, D.C., November 4–9, 2005; the Annual Meeting of the Association of Directors of Medical Student Education in Psychiatry in Annapolis, Maryland, June 22–24, 2006; and the AAMC Northeast Group on Educational Affairs Meeting in Stony Brook, NY, June 8–9, 2007.
Rights and permissions
About this article
Cite this article
Cutler, J.L., Harding, K.J., Mozian, S.A. et al. Discrediting the notion “working with ‘crazies’ will make you ‘crazy’”: addressing stigma and enhancing empathy in medical student education. Adv in Health Sci Educ 14, 487–502 (2009). https://doi.org/10.1007/s10459-008-9132-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10459-008-9132-4