

- Division of Molecular Psychiatry, Translational Research Center, University Hospital of Psychiatry and Psychotherapy, University of Bern, Bern, Switzerland
Correspondence Address:
Christian Saleh
Division of Molecular Psychiatry, Translational Research Center, University Hospital of Psychiatry and Psychotherapy, University of Bern, Bern, Switzerland
DOI:10.4103/sni.sni_15_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Christian Saleh, Gregor Hasler. Deep brain stimulation for psychiatric disorders: Is there an impact on social functioning?. 07-Jul-2017;8:134
How to cite this URL: Christian Saleh, Gregor Hasler. Deep brain stimulation for psychiatric disorders: Is there an impact on social functioning?. 07-Jul-2017;8:134. Available from: http://surgicalneurologyint.com/surgicalint-articles/deep-brain-stimulation-for-psychiatric-disorders-is-there-an-impact-on-social-functioning/
Date of Submission
09-Jan-2017
Date of Acceptance
06-May-2017
Date of Web Publication
07-Jul-2017
Abstract
Background:Deep brain stimulation (DBS) for refractory psychiatric disorders shows promising effects on symptom-reduction, however, little is known regarding the effects of DBS on social outcome.
Methods:A PubMed search based on original studies of DBS for psychiatric disorders [treatment resistant depression (TRD), Gilles de la Tourette's syndrome (GTS), and obsessive compulsive disorder (OCD)] was conducted. Data on social outcome following surgery were extracted and analyzed.
Results:Social functioning was not a primary outcome measure in the reviewed article. The literature is incomplete and inconclusive on this variable, however from the reported data, there is some evidence that DBS has the potential to improve social functioning.
Conclusions:More systematic and detailed data gathering and reporting on social outcome with longer follow-ups are needed to evaluate more exhaustively the role of DBS in refractory psychiatric disorders.
Keywords: Deep brain stimulation, Gilles de la Tourette's syndrome, obsessive compulsive disorder, refractory psychiatric disorders, social outcome, treatment resistant depression
INTRODUCTION
Deep brain stimulation (DBS) is considered a safe and established treatment option with the advantages of being nondestructive, reversible, and adjustable. The renaissance of DBS dates to 1987, when the French group led by Benabid applied DBS for refractory motor disease,[
MATERIALS AND METHODS
A PubMed search based on original studies of DBS for psychiatric disorders was conducted without any time limit. Only articles in English language were selected. The search was based on the current three main DBS indications for refractory psychiatric disorders, treatment resistant depression (TRD), GTS, and OCD. Key words used were “deep brain stimulation” in combined fashion with “Gilles de la Tourette's syndrome,” “obsessive compulsive disorder,” and “depression.” Only original studies, case reports/case series were included. Reviews, commentaries and basic research studies were excluded. Further articles were identified via an analysis of relevant papers obtained from the first literature search. From the initial search, we considered 87 papers for the first analysis. All papers on DBS for psychiatric disorders were reviewed at this stage for the outcome measure of social functioning; only articles reporting on this variable were considered for final analysis. Thirty two articles were included for our study: 11 GTS studies, 13 OCD studies, and 8 TRD studies. For each psychiatric indication, the data on demographics, the clinical results of DBS and the effect on social behavior were extracted, tabulated, and analyzed [Tables
RESULTS
The studies included in our analysis included 236 patients: 70 GTS patients, 88 OCD patients, and 78 TRD patients [Tables
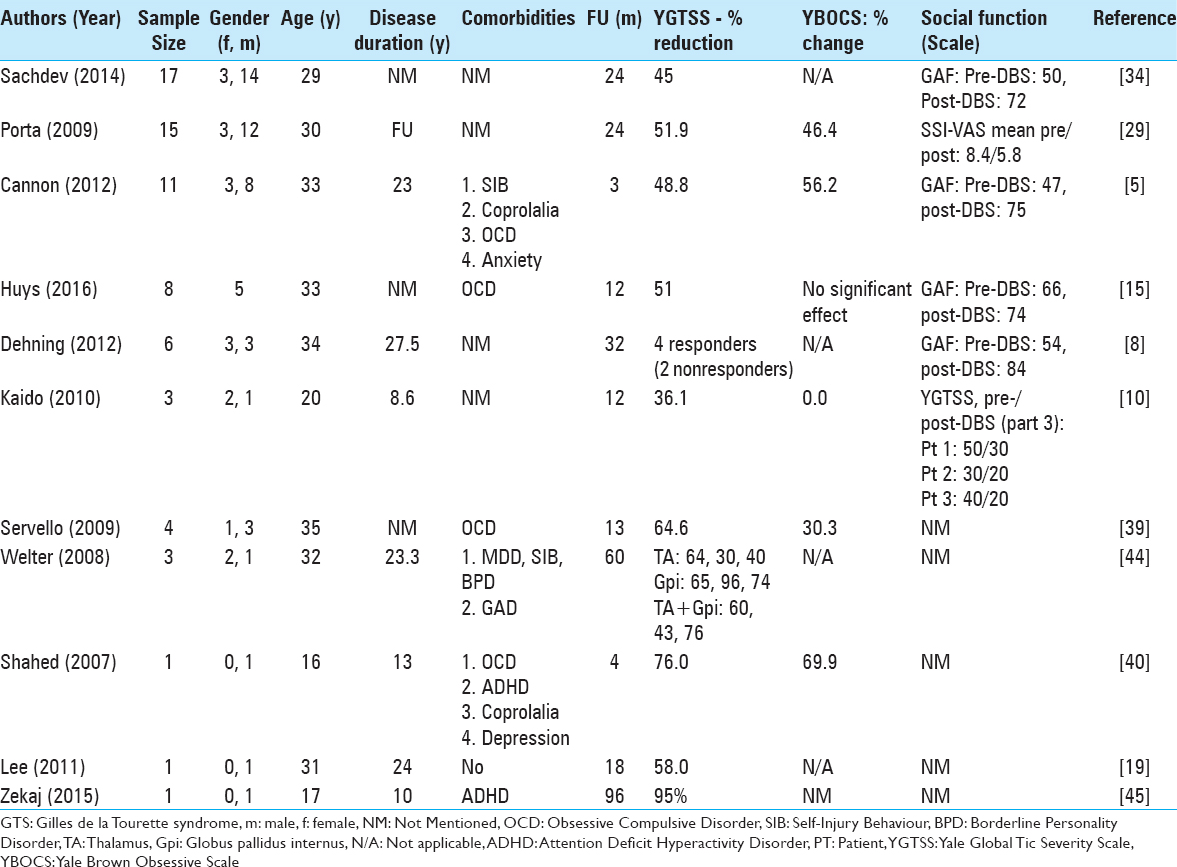
Gilles de la Tourette
Eleven GTS studies were included [
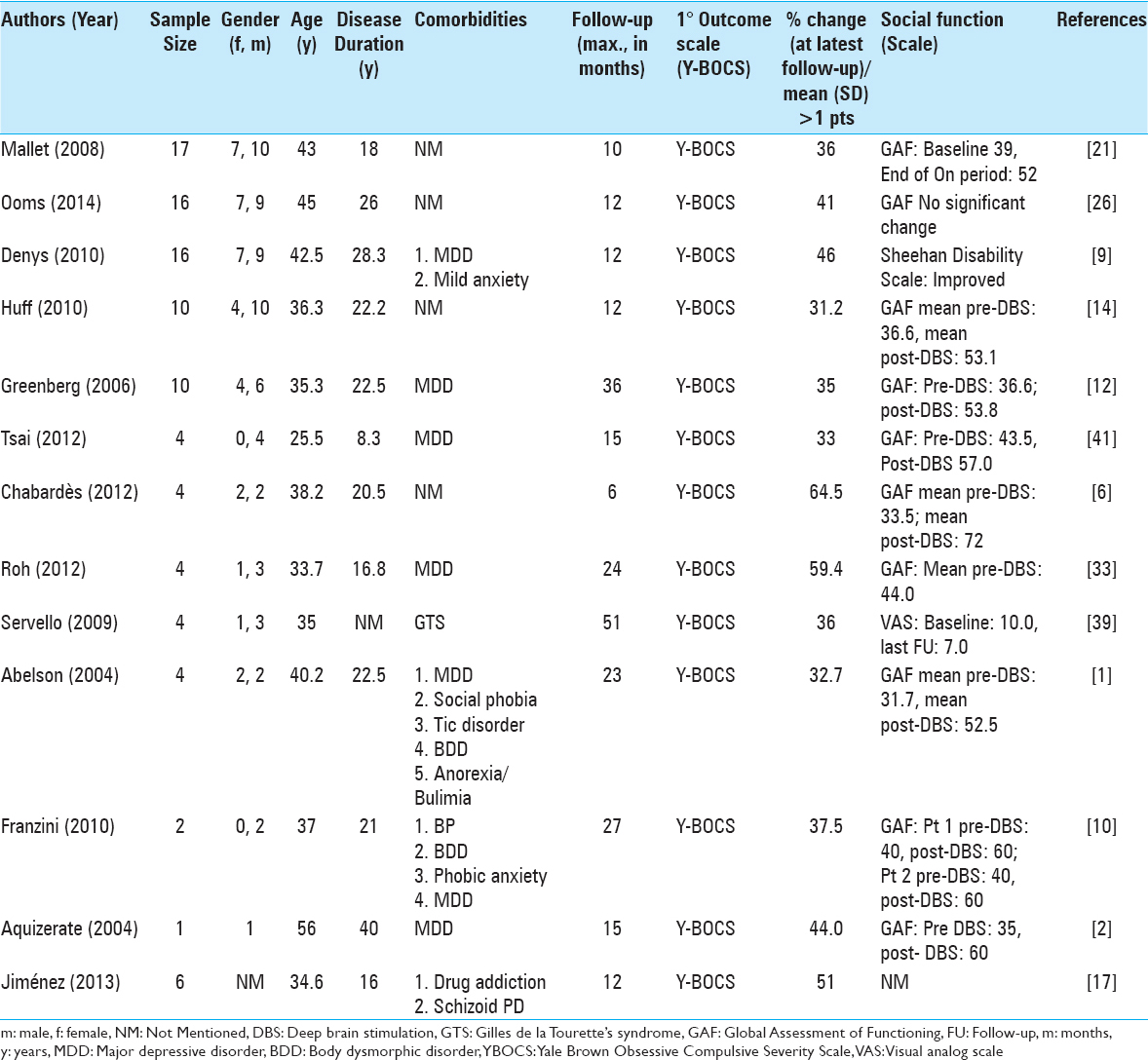
Obsessive compulsive disorder
13 OCD studies were included [
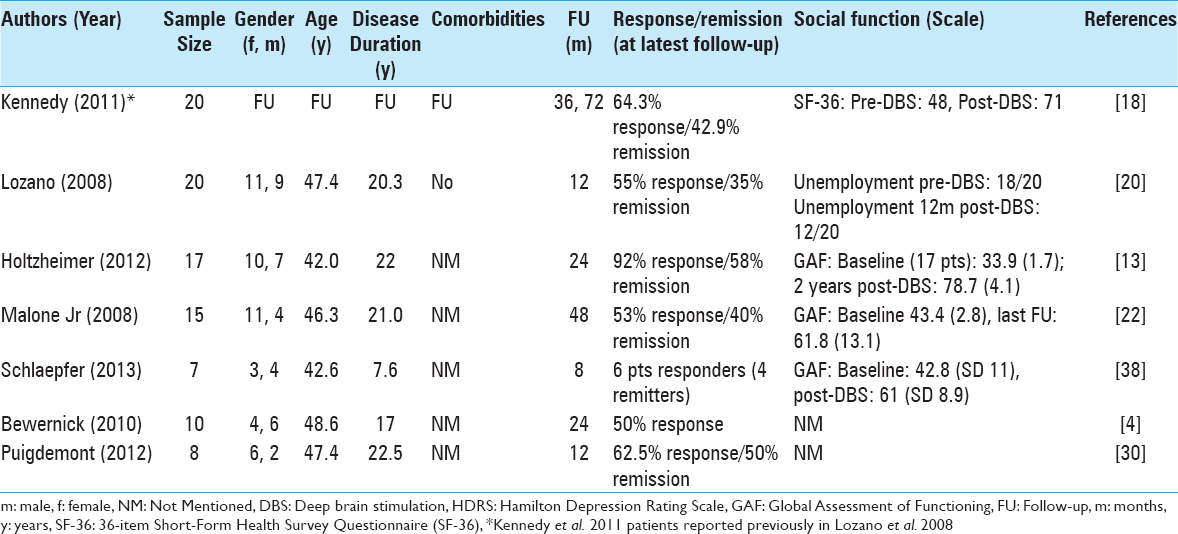
Treatment resistant depression
Eight TRD studies were included [
Deep brain stimulation and social functioning
Deep brain stimulation and social functioning in Gilles de la Tourette's syndrome
In a cohort of 17 patients Sachdev et al.[
Dehning et al.[
The results of a 2-year follow-up on 15 patients were published by Porta et al. in 2009.[
In 2009, this same group from Milan used nucleus accumbens DBS in four patients, who had failed to respond to thalamic or pallidal DBS.[
Welter et al.[
A 76% tic reduction on the YGTSS and to a circa 70% change on the YBOCS in a 16-year-old male patient was recorded by Shahed et al.[
Lee et al.[
Zekaj et al.[
Deep brain stimulation and social functioning in obsessive compulsive disorder
Greenberg et al.[
Jiménez et al.[
Chabardès et al.[
Roh et al.[
Abelson et al.[
Deep brain stimulation and social functioning in treatment resistant depression
Kennedy et al.[
Lozano et al.[
Holtzheimer et al.[
Bewernick et al.[
Puigdemont et al.[
DISCUSSION
The reviewed literature showed a significant variability in many factors including number of patients, mean age, comorbidities, disease duration, follow-up periods, and evaluating scales. Analyzing in a systematic and organized manner the available data allowed, however, despite the aforementioned encountered limitations, to appreciate certain patterns of the impact of DBS on social functioning.
Based on the available literature, DBS in refractory psychiatric disorders seems to have the potential to improve social functioning.
The modern era of DBS has made significant advances in treating refractory psychiatric respect the beginnings of psychosurgery.[
However, we cannot make definitive conclusions on the effects of DBS on social functioning based on the current data. The positive results have to be interpreted with great caution. We had to exclude a large number of patients treated with DBS for psychiatric disorders, approximately 250, from our study since no data on social functioning were available. Within this context, one has to be bear in mind that authors may have avoided to report negative or neutral social outcomes, potentially leading to a selection bias in our considerations. In addition, sample sizes were too small (mean 8.3 participants per study, SD 3.2) to generalize findings. Studies focused more on symptom severity reduction than on social functioning. Data gathering on social impact was based on qualitative as quantitative approaches rendering a meaningful comparison of results between studies difficult. The social functioning showed also heterogeneity within the same study not allowing an analysis of different outcomes within the same study.
The data on GTS patients may be particularly difficult to interpret. Contrary to DBS for motor diseases in DBS for psychiatric disorders, targets are multiple. In GTS, the target choice is particularly complicated and heterogeneous given the great phenotypic variability of GTS.[
To fully evaluate the risks and benefits, including social functioning, of DBS in psychiatric disorders, several factors have to be systematically assessed: Severity of the treated patients refractory to any conventional psychiatric treatment, the natural disease course, the severe side effects of conventional treatment, the symptomatic improvement, and the social impact of DBS.
Social outcomes are particularly important in the assessment of therapeutic intervention in psychiatry. The World Health Organization (1948) defines health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.”[
The assessment of social outcomes is not trivial. Unfortunately, there is no standard assessment. Social functioning includes multiple roles of an individual such as personal, social and professional interactions; it relates consequently directly to the quality of life of a participant.[
To evaluate more exhaustively the social outcomes of DBS, we recommend the use of the GAF and the Social Adjustment Scale.[
CONCLUSION
The current data on the social effects of DBS in psychiatric conditions is incomplete and inconclusive. However, from the available data DBS seems to have the potential to improve social functioning. Larger, multicentered trials are needed to increase statistical power, with systematic assessment of social outcomes along with longer follow-ups and closer postoperative surveillance, to evaluate more accurately the impact of DBS on social functioning.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Abelson JL, Curtis GC, Sagher O, Albucher RC, Harrigan M, Taylor SF. Deep brain stimulation for refractory obsessive-compulsive disorder. Biol Psychiatry. 2005. 57: 510-6
2. Aouizerate B, Cuny E, Martin-Guehl C, Guehl D, Amieva H, Benazzouz A. Deep brain stimulation of the ventral caudate nucleus in the treatment of obsessive-compulsive disorder and major depression. Case report. J Neurosurg. 2004. 101: 682-6
3. Benabid AL, Pollak P, Gervason C, Hoffmann D, Gao DM, Hommel M. Long-term suppression of tremor by chronic stimulation of the ventral intermediate thalamic nucleus. Lancet. 1991. 337: 403-6
4. Bewernick BH, Hurlemann R, Matusch A, Kayser S, Grubert C, Hadrysiewicz B. Nucleus accumbens deep brain stimulation decreases ratings of depression and anxiety in treatment-resistant depression. Biol Psychiatry. 2010. 67: 110-6
5. Cannon E, Silburn P, Coyne T, O’Maley K, Crawford JD, Sachdev PS. Deep brain stimulation of anteromedial globus pallidus interna for severe Tourette's syndrome. Am J Psychiatry. 2012. 169: 860-6
6. Chabardes S, Polosan M, Krack P, Bastin J, Krainik A, David O. Deep brain stimulation for obsessive-compulsive disorder: Subthalamic nucleus target. World Neurosurg. 2013. 80: S31 e1-8
7. De Silva MJ, Cooper S, Li HL, Lund C, Patel V. Effect of psychosocial interventions on social functioning in depression and schizophrenia: Meta-analysis. Br J Psychiatry. 2013. 202: 253-60
8. Dehning S, Leitner B, Schennach R, Muller N, Botzel K, Obermeier M. Functional outcome and quality of life in Tourette's syndrome after deep brain stimulation of the posteroventrolateral globus pallidus internus: Long-term follow-up. World J Biol Psychiatry. 2014. 15: 66-75
9. Denys D, Mantione M, Figee M, van den Munckhof P, Koerselman F, Westenberg H. Deep brain stimulation of the nucleus accumbens for treatment-refractory obsessive-compulsive disorder. Arch Gen Psychiatry. 2010. 67: 1061-8
10. Franzini A, Messina G, Gambini O, Muffatti R, Scarone S, Cordella R. Deep-brain stimulation of the nucleus accumbens in obsessive compulsive disorder: Clinical, surgical and electrophysiological considerations in two consecutive patients. Neurol Sci. 2010. 31: 353-9
11. Grad FP. The Preamble of the Constitution of the World Health Organization. Bull World Health Organ. 2002. 80: 981-4
12. Greenberg BD, Malone DA, Friehs GM, Rezai AR, Kubu CS, Malloy PF. Three-year outcomes in deep brain stimulation for highly resistant obsessive-compulsive disorder. Neuropsychopharmacology. 2006. 31: 2384-93
13. Holtzheimer PE, Meeks TW, Kelley ME, Mufti M, Young R, McWhorter K. A double blind, placebo-controlled pilot study of galantamine augmentation of antidepressant treatment in older adults with major depression. Int J Geriatr Psychiatry. 2008. 23: 625-31
14. Huff W, Lenartz D, Schormann M, Lee SH, Kuhn J, Koulousakis A. Unilateral deep brain stimulation of the nucleus accumbens in patients with treatment-resistant obsessive-compulsive disorder: Outcomes after one year. Clin Neurol Neurosurg. 2010. 112: 137-43
15. Huys D, Bartsch C, Koester P, Lenartz D, Maarouf M, Daumann J. Motor Improvement and Emotional Stabilization in Patients With Tourette Syndrome After Deep Brain Stimulation of the Ventral Anterior and Ventrolateral Motor Part of the Thalamus. Biol Psychiatry. 2016. 79: 392-401
16. Jiménez F, Nicolini H, Lozano AM, Piedimonte F, Salin R, Velasco F. Electrical stimulation of the inferior thalamic peduncle in the treatment of major depression and obsessive compulsive disorders. World Neurosurg. 2013. 80: S30 e17-25
17. Kaido T, Otsuki T, Kaneko Y, Takahashi A, Omori M, Okamoto T. Deep brain stimulation for Tourette syndrome: A prospective pilot study in Japan. Neuromodulation. 2011. 14: 123-8
18. Kennedy SH, Giacobbe P, Rizvi SJ, Placenza FM, Nishikawa Y, Mayberg HS. Deep brain stimulation for treatment-resistant depression: Follow-up after 3 to 6 years. Am J Psychiatry. 2011. 168: 502-10
19. Lee MW, Au-Yeung MM, Hung KN, Wong CK. Deep brain stimulation in a Chinese Tourette's syndrome patient. Hong Kong Med J. 2011. 17: 147-50
20. Lozano AM, Mayberg HS, Giacobbe P, Hamani C, Craddock RC, Kennedy SH. Subcallosal cingulate gyrus deep brain stimulation for treatment-resistant depression. Biol Psychiatry. 2008. 64: 461-7
21. Mallet L, Polosan M, Jaafari N, Baup N, Welter ML, Fontaine D. Subthalamic nucleus stimulation in severe obsessive-compulsive disorder. N Engl J Med. 2008. 359: 2121-34
22. Malone DA, Dougherty DD, Rezai AR, Carpenter LL, Friehs GM, Eskandar EN. Deep brain stimulation of the ventral capsule/ventral striatum for treatment-resistant depression. Biol Psychiatry. 2009. 65: 267-75
23. Mayberg HS, Lozano AM, Voon V, McNeely HE, Seminowicz D, Hamani C. Deep brain stimulation for treatment-resistant depression. Neuron. 2005. 45: 651-60
24. Nuttin B, Cosyns P, Demeulemeester H, Gybels J, Meyerson B. Electrical stimulation in anterior limbs of internal capsules in patients with obsessive-compulsive disorder. Lancet. 1999. 354: 1526-
25. Ogren K, Sandlund M. Lobotomy at a state mental hospital in Sweden. A survey of patients operated on during the period 1947-1958. Nord J Psychiatry. 2007. 61: 355-62
26. Ooms P, Mantione M, Figee M, Schuurman PR, van den Munckhof P, Denys D. Deep brain stimulation for obsessive-compulsive disorders: Long-term analysis of quality of life. J Neurol Neurosurg Psychiatry. 2014. 85: 153-8
27. Patel V, Simon G, Chowdhary N, Kaaya S, Araya R. Packages of care for depression in low- and middle-income countries. PLoS Med. 2009. 6: e1000159-
28. Porta M, Saleh C, Zekaj E, Zanaboni Dina C, Bona AR, Servello D. Why so many deep brain stimulation targets in Tourette's syndrome? Toward a broadening of the definition of the syndrome. J Neural Transm (Vienna). 2016. 123: 785-90
29. Porta M, Sassi M, Ali F, Cavanna AE, Servello D. Neurosurgical treatment for Gilles de la Tourette syndrome: The Italian perspective. J Psychosom Res. 2009. 67: 585-90
30. Puigdemont D, Perez-Egea R, Portella MJ, Molet J, de Diego-Adelino J, Gironell A. Deep brain stimulation of the subcallosal cingulate gyrus: Further evidence in treatment-resistant major depression. Int J Neuropsychopharmacol. 2012. 15: 121-33
31. Ramirez A, Ekselius L, Ramklint M. Axis V - Global Assessment of Functioning scale (GAF), further evaluation of the self-report version. Eur Psychiatry. 2008. 23: 575-9
32. Renner F, Cuijpers P, Huibers MJ. The effect of psychotherapy for depression on improvements in social functioning: A meta-analysis. Psychol Med. 2014. 44: 2913-26
33. Roh D, Chang WS, Chang JW, Kim CH. Long-term follow-up of deep brain stimulation for refractory obsessive-compulsive disorder. Psychiatry Res. 2012. 200: 1067-70
34. Sachdev PS, Mohan A, Cannon E, Crawford JD, Silberstein P, Cook R. Deep brain stimulation of the antero-medial globus pallidus interna for Tourette syndrome. PLoS One. 2014. 9: e104926-
35. Saleh C, Fontaine D. Deep brain stimulation for psychiatric diseases: What are the risks?. Curr Psychiatry Rep. 2015. 17: 33-
36. Saleh C, Gale JT, Eskandar E. The need for a multifactorial approach to raise the standard in deep brain stimulation reporting. Neuromodulation. 2011. 14: 183-4
37. Schaub D, Brune M, Jaspen E, Pajonk FG, Bierhoff HW, Juckel G. The illness and everyday living: Close interplay of psychopathological syndromes and psychosocial functioning in chronic schizophrenia. Eur Arch Psychiatry Clin Neurosci. 2011. 261: 85-93
38. Schlaepfer TE, Bewernick BH, Kayser S, Madler B, Coenen VA. Rapid effects of deep brain stimulation for treatment-resistant major depression. Biol Psychiatry. 2013. 73: 1204-12
39. Servello D, Sassi M, Brambilla A, Porta M, Haq I, Foote KD. De novo and rescue DBS leads for refractory Tourette syndrome patients with severe comorbid OCD: A multiple case report. J Neurol. 2009. 256: 1533-9
40. Shahed J, Poysky J, Kenney C, Simpson R, Jankovic J. GPi deep brain stimulation for Tourette syndrome improves tics and psychiatric comorbidities. Neurology. 2007. 68: 159-60
41. Tsai HC, Chang CH, Pan JI, Hsieh HJ, Tsai ST, Hung HY. Pilot study of deep brain stimulation in refractory obsessive-compulsive disorder ethnic Chinese patients. Psychiatry Clin Neurosci. 2012. 66: 303-12
42. Vandewalle V, van der Linden C, Groenewegen HJ, Caemaert J. Stereotactic treatment of Gilles de la Tourette syndrome by high frequency stimulation of thalamus. Lancet. 1999. 353: 724-
43. Weissman MM, Prusoff BA, Thompson WD, Harding PS, Myers JK. Social adjustment by self-report in a community sample and in psychiatric outpatients. J Nerv Ment Dis. 1978. 166: 317-26
44. Welter ML, Mallet L, Houeto JL, Karachi C, Czernecki V, Cornu P. Internal pallidal and thalamic stimulation in patients with Tourette syndrome. Arch Neurol. 2008. 65: 952-7
45. Zekaj E, Saleh C, Porta M, Servello D. Temporary deep brain stimulation in Gilles de la Tourette syndrome: A feasible approach?. Surg Neurol Int. 2015. 6: 122-
Commentary
Antonio A.F. De Salles- Professor Emeritus of Neurosurgery - UCLA, Departments of Neurosurgery and Radiation Oncology. Head, HCor Neuroscience E-mail:
a.desalles@yahoo.com
We recommend our readers to pay attention to this excellent and organized review of the literature on the social impact of deep brain stimulation (DBS) for diverse applications in psychiatric disorders. The importance of this article is immense, as it criticizes the literature on the most important role of any therapy. Does DBS really impact on patients’ quality of life?
DBS will only be valuable as a therapy if it is scientifically shown that it impacts on the patients’ quality of life, mostly bring the psychiatric patients to the main flow of society as productive citizens, or at least less dependent as possible. Although quantitative data are scarce, the positivity of the comments observed by the majority of the authors make DBS a valuable therapy for the scientific community to spend time sorting its real value. Those interested on behavior surgery, the discredit in the past psychosurgery, have to take the task of evaluating with critical scales reflecting adjustment of patients in their social environment in a strict scientific fashion.

