

Abstract
Objective. Systemic lupus erythematosus (SLE) is associated with high cardiovascular morbidity and mortality. Cardiovascular involvement is frequently underestimated by routine imaging techniques. Our aim was to determine if new echocardiographic imaging modalities like tissue Doppler (TDI), strain rate (SRR), and strain (SRI) imaging detect abnormalities in left ventricular (LV) function in asymptomatic patients with SLE.
Methods. Sixty-seven young patients with SLE (mean age 42 ± 10 yrs) without typical symptoms or signs of heart failure or angina, and a matched healthy control group (n = 40), underwent standard transthoracic echocardiography, TDI, SRR, and SRI imaging of the LV as well as assessment of disease characteristics.
Results. Despite findings within the normal range on routine standard 2-dimensional echocardiography, SLE was associated with significantly impaired systolic and diastolic myocardial velocities of the LV measured by TDI [mean global TDI: systolic (s): 2.9 ± 0.9 vs 3.9 ± 0.7 cm/s, p < 0.05; early (e): 4.3 ± 1.5 vs 6.3 ± 1.3 cm/s, p < 0.05; late (a): 2.9 ± 0.8 vs 3.4 ± 0.8 cm/s, p < 0.05; values ± SD); SRR (s: −0.8 ± 0.1 vs −1.1 ± 0.1 s−1; e: 1.1 ± 0.2 vs 1.6 ± 0.3 s−1; a: 0.7 ± 0.1 vs 1.0 ± 0.2 s−1; all p < 0.05); and SR (−15.11 ± 2.2% vs −19.7 ± 1.9%; p < 0.05) compared to the control group. Further, elevated disease activity, measured with the ECLAM and the SLEDAI score, resulted in significantly lower values for LV longitudinal function measured by SRR and SR, but not by TDI.
Conclusion. SLE is associated with a significant impairment of systolic and diastolic LV longitudinal function in patients without cardiac symptoms. New imaging modalities provide earlier insight into cardiovascular involvement in SLE and seem to be superior to standard echocardiography to detect subclinical myocardial disease.
Systemic lupus erythematosus (SLE) is a multiorgan autoimmune disease associated with high cardiovascular morbidity and mortality that primarily affects young women1–4. Myocardial involvement occurs in 8%–14% of patients, and all cardiac structures may be involved. However, the detection of myocardial involvement in patients with SLE is difficult since clinical signs and symptoms are nonspecific, and myocardial involvement may be present in completely asymptomatic patients5. In this regard, standard methods for evaluating cardiac function used in clinical practice often lack the sensitivity to detect myocardial abnormalities in SLE6–9. Thus, the prevalence of myocardial involvement in patients with SLE may be significantly underestimated and may be an important contributor to cardiovascular morbidity and mortality.
Because myocardial architecture is intricate, global left ventricular (LV) function is more complex, with radial, longitudinal, and torsional components10–13. In patients with heart failure, longitudinal LV function represents an independent prognostic variable of survival14–19, and atrioventricular displacement during the cardiac cycle constitutes an important component of global function of the heart20 and is thought to be reduced early in the progression of several pathologic conditions21–23.
Tissue Doppler imaging (TDI) is a relatively new ultrasonographic technique that measures regional systolic and diastolic myocardial velocities24,25 and has been used for quantitative analysis of global and regional myocardial function26,27. TDI can assess impairment of myocardial function in left ventricular hypertrophy and stress-induced ischemia, providing important prognostic information15,16,28. Strain imaging (SRI) is a new technique derived from TDI that allows the determination of velocity gradients between 2 points in space29. The resulting contraction variable is independent of passive tethering effects or drawing motion from other regions and therefore appears promising for quantification of regional myocardial function30.
To date there is relatively limited evidence that SLE may be accompanied by a decrease in the systolic and diastolic function of the LV31–34. Further, to our knowledge there is no published report on the incremental value of strain imaging techniques for the early detection of cardiac involvement in adults with SLE. We sought to determine whether new echocardiographic methods are sensitive enough to assess subclinical myocardial involvement in SLE and whether such involvement is related to aspects of this complex disease (disease activity, serological markers, disease duration).
MATERIALS AND METHODS
Patient selection and enrolment
Sixty-seven young patients with SLE treated at our outpatient clinic and 40 age and sex matched healthy controls were enrolled into the study. Diagnosis of SLE was based on criteria defined by the American College of Rheumatology35. The consecutive patients were visited by 2 rheumatologists (RM, HML) and were included after informed consent. The study was approved by the institutional review board. The presence of cardiovascular risk factors (hypertension, hyperlipidemia, diabetes mellitus, and cigarette smoking) and clinical disease activity based on European Consensus Lupus Activity Measurement (ECLAM) and the SLE Disease Activity Index (SLEDAI) score were obtained. An ECLAM score > 236 and a SLEDAI score > 1018,19 were considered indicative of a more active disease. Blood samples were investigated determining renal function, C-reactive protein (CRP), anti-dsDNA antibodies, antinuclear antibodies, and erythrocyte sedimentation rate (ESR) as biochemical marker for disease activity.
All patients were in stable clinical condition and under optimized therapy. To avoid potential confounding effects of non-SLE related myocardial complications we excluded patients with typical symptoms or signs of heart failure, significant valvular disease, dilated cardiomyopathy, reduced ejection fraction of < 55%, obvious wall motion abnormalities, severe diastolic dysfunction, pericardial abnormalities, history or symptoms of coronary artery disease (CAD), myocardial infarction, evidence of ischemic heart disease by any stress test or coronary angiography, bundle branch block, atrial fibrillation, serum creatinine > 1.5 mg/dl, or inadequate performance on echocardiograms.
Standard ultrasound examination
Two-dimensional (2D) transthoracic echocardiographic examinations were performed with a commercial ultrasound machine (iE33, Philips Medical Systems, Bothell, WA, USA). Three consecutive cardiac cycles of each view were acquired during breath-hold and stored digitally. The heart rate and blood pressure were measured in supine position prior to the echocardiographic examination.
Great care was taken to obtain an optimal visualization, e.g., to avoid apical foreshortening and to maximize the length from base to apex. The LV dimensions were measured according to recently published recommendations of the American Society of Echocardiography37. End-diastolic and end-systolic LV volumes and ejection fraction were determined by manual tracing of end-systolic (smallest LV shape) and end-diastolic endocardial borders (largest LV shape) using apical 4-chamber and 2-chamber views, employing the modified Simpson’s method for biplane assessment. Pulsed Doppler echocardiography of transmitral flow velocities was performed, positioning a sample volume at the level of the mitral tips to measure the peak velocities of early (E) and late (A) filling waves and deceleration time (DT) of E. Cardiac output and cardiac index were calculated from the stroke volume estimated using the modified Simpson’s method. The LV mass was indexed either for the body surface area or its growth relation with height (height2.7)38,39.
Tissue Doppler and strain imaging data acquisition
2D color tissue Doppler recordings with second harmonic imaging were collected with high frame rates (100–170 frames/s) during brief breath-hold, from the apical 4-chamber, 2-chamber, and long-axis views. Pulsed-wave tissue Doppler imaging (PW-TDI) was performed, the sample volume was placed on the lateral mitral annulus in the apical 4-chamber view, and the systolic (s), early (e), and late (a) peak diastolic velocities were measured. Three consecutive beats were measured and averaged for each measurement. The cardiac cycles were recorded as 2D color video loops, and the acquired raw data were saved for offline analysis (Xcelera and QLab, Philips Medical Systems). The inferoseptal, anterolateral, inferior, anterior, and inferolateral (posterior) walls were investigated for longitudinal systolic peak values for TDI, strain (SR), and strain rate (SRR) imaging. Diastolic peak early (e) and late (a) diastolic values for SRR and TDI were also measured.
The region of interest was evaluated using “M-Line” sample volumes (7.5 mm wide), which were placed reaching from the basal over the middle segments towards the apex, in the apical transthoracic views of the LV, excluding the apical regions of the LV, to avoid angle-dependent underestimation (at least < 30°). The “M-Line” was then tracked manually and adjusted frame by frame. We considered the sample volume position to be acceptable when the SR waveforms were reproducible over 3 consecutive cardiac cycles. The analysis of the raw data images allows determination of TDI, SR, and SRR curves from the same sample volume at the same time in the same position of the images. A mean value for each wall was determined, as well as a value for the TDI in the basal segments. The analyses of the echocardiographic examinations were performed by the investigators in a blinded manner.
Intra- and interobserver variability
To examine intraobserver variability, a sample of 20 representative echocardiographic examinations for the estimation of TDI and strain parameters were randomly selected for masked review by the same investigator. To examine interobserver variability a coinvestigator blinded to the clinical information and the results of the first investigator examined 20 randomly selected echocardiographic studies for the estimation of TDI and strain parameters.
Statistics
Differences among the groups were assessed with the chi-square test for categoric variables. Comparisons among groups were made using Student’s t-test with a Bonferroni correction and one-way factorial ANOVA, with post-hoc testing for multiple comparisons where appropriate. The differences were considered significant after applying the conservative Bonferroni-Holm procedure, to adjust the nominal alpha niveau of p < 0.05. Additionally throughout the t-test a Satterthwaite correction was used. Linear regression analyses and a correlation test (either Pearson’s or Spearman’s method) were performed to assess univariate relations. Data are expressed as mean values ± SD. Statistical significance was accepted at the p < 0.05 level.
RESULTS
Clinical findings
The clinical characteristics are shown in Table 1. The composition of patients in the study and control groups was comparable with respect to age, sex, blood pressure, and heart rate. Among subjects with SLE 21% had arterial hypertension. The median ECLAM score was 3. Current or former use of prednisone was present in 90% of patients, whereas other immunosuppressive therapy was less common (azathioprine in 11%, cyclosporine 10%, mycophenolic acid 10%, cyclophosphamide 8%, and methotrexate 10%). Hydroxychloroquine had been used by 60% of patients.
Characteristics of patients with SLE and the control group.
2D echocardiography
LV wall thicknesses, chamber dimensions, and myocardial mass were higher in patients with SLE than in the reference group (Table 2), resulting in a higher relative LV mass and prevalence of LV hypertrophy (p < 0.05). In agreement with others40, in our study even SLE patients who were normotensive had greater LV mass than controls (161 ± 36 g vs 138 ± 23 g, respectively; p < 0.05; Table 2); moreover, the presence of both SLE and hypertension resulted in a further increase of LV mass (187 ± 38 g; p < 0.05).
Comparison of myocardial structure and function in patients with SLE and the control group with 2-dimensional echocardiography.
Biplane estimation of LV ejection fraction revealed a slightly reduced—albeit within the normal range—ejection fraction in the SLE group compared to healthy controls (Table 2). Patients with SLE had greater LV end-diastolic dimension (EDD), greater LV end-systolic dimension (ESD), and a reduced fractional shortening compared to controls. Left atrial dimensions were significantly larger in SLE patients (Table 2). Interestingly, 2 classical characteristics for longitudinal function, MAPSE (mitral annular plane systolic excursion) and TAPSE (tricuspid annular plane systolic excursion), of LV and RV, were already significantly reduced in patients with SLE compared to controls (Table 2).
Indices of transmitral flow are shown in Table 2. Similar to most of the 2D echocardiographic features, no standard Doppler flow measurement differentiated the 2 groups. As anticipated, SLE patients showed a significant reduction in PW-TDI measurements of the lateral mitral annulus. PW-TDI revealed a reduction in the systolic as well as in the diastolic (e, a) LV function (Table 2 and Figure 1A). The ratio of E/e was elevated in the SLE group compared to controls, but the level was still near the normal range (Table 2 and Figure 1B), so no firm conclusion can be drawn. Estimated systolic pulmonary artery pressure (sPA), derived from the tricuspid regurgitation signal, was still within the normal range but was significantly elevated in the SLE group compared to healthy controls (Table 2).

Comparison of myocardial structure and function in SLE patients and controls with 2-dimensional echocardiography and strain imaging. A. PW-TDI-s, peak systolic myocardial velocity derived by pulsed wave Doppler tissue, is impaired in SLE. B. Reduced diastolic function in SLE determined by E/e ratio. Peak systolic strain rate (C, SRR) and strain (D, SR) is reduced in SLE compared to controls. Values are mean ± SD. **p < 0.05
Tissue Doppler and strain imaging
To render the data less complex, to present them more clearly, and because of similar findings in different wall regions, mean values of TDI derived from all regions were calculated and are presented in Table 3. Peak systolic TDI differed between SLE patients and controls at any site (p < 0.05). Also, peak early and late diastolic TDI values were statistically different among the groups (p < 0.05). SRI and SRR clearly documented that SLE was associated with a decrease in systolic function and diastolic function in asymptomatic patients with SLE (Figure 1C and 1D).
Comparison of LV function with tissue Doppler and strain imaging in SLE patients and in controls.
SRI and TDI measurements were significantly reduced in all subjects with SLE. There was no significant difference in SRI in the group of patients with SLE and hypertension compared to those with SLE and without hypertension (−15.2 ± 2.2% vs −14.7 ± 2.5%; p = 0.43). Also, subjects receiving hydroxychloroquine showed no significant differences (−15.2 ± 2.1% vs −15.1 ± 2.5%; p = 0.9).
Analysis of disease activity
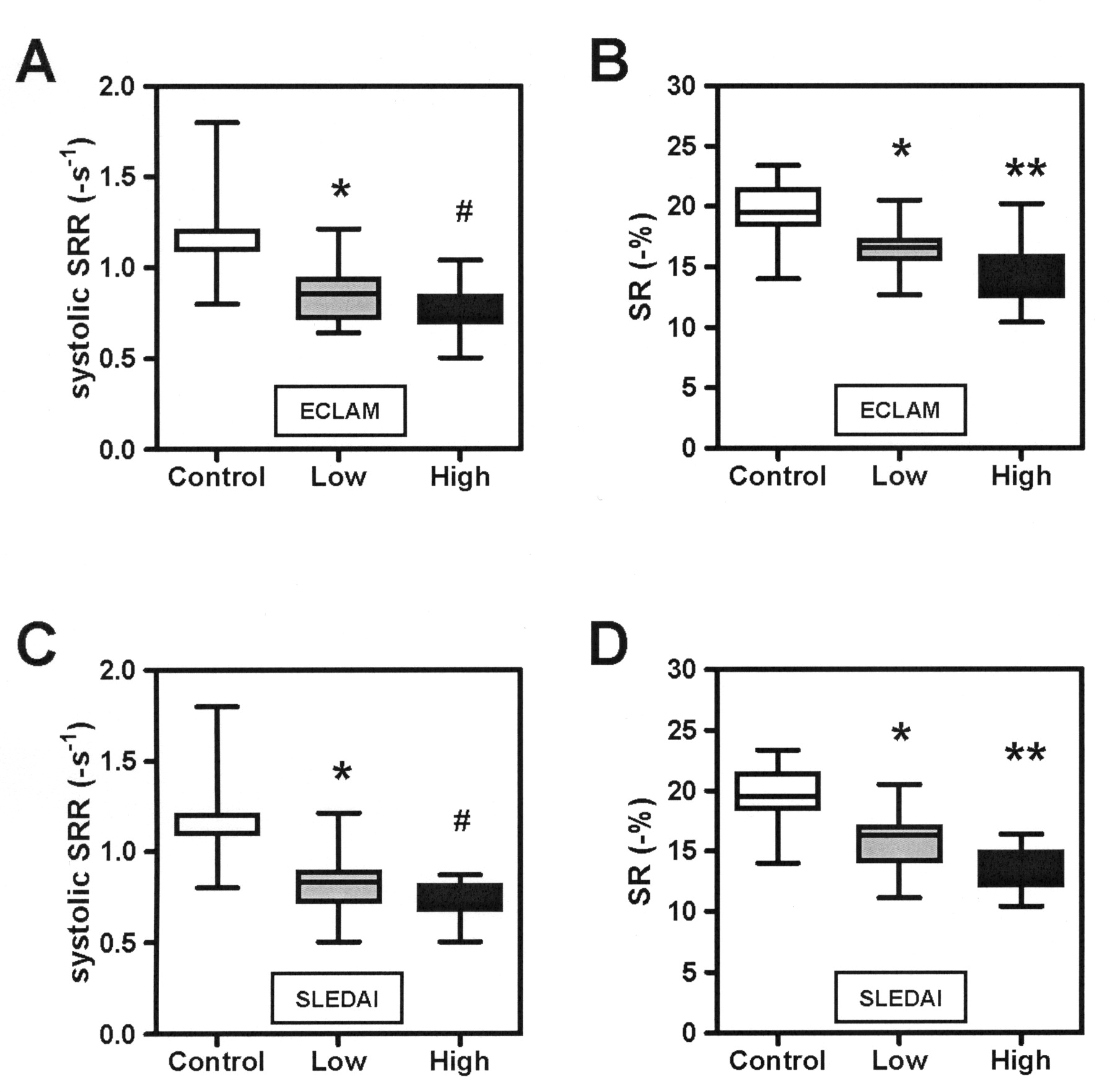
SLE patients were divided into 2 groups according to higher and lower disease activity. Interestingly, those with a higher ECLAM and SLEDAI activity score presented a significantly reduced longitudinal function, when measured with SRR and SRI (Figure 2). This difference was still clearly detectable for SRI without the patients with SLE plus hypertension (p < 0.05). Of note, there was still a significant difference between subjects with low disease activity and control subjects (Figure 2). The measurements of TDI and PW-TDI could not differentiate between subjects with higher versus lower disease activity (p = 0.83 and p = 0.49). LV mass indices also did not show an association with disease activity (data not shown). Measurements of CRP, ESR, and dsDNA antibodies did not correlate significantly with longitudinal function (p = 0.4, p = 0.07, and p = 0.9, respectively). Thus SRI performed better than TDI in detecting differences of longitudinal systolic function in SLE regarding disease activity.

Evaluation of left ventricular longitudinal function in SLE patients with lower and higher disease activity using the ECLAM (A and B) and the SLEDAI score (C and D). A, C: peak systolic strain rate (SRR); B, D: peak systolic strain (SR). *p < 0.05 vs control, **p < 0.05 vs Low, #p < 0.05 vs Low.
Observer variabilities
The intraobserver variabilities were 6.5% for TDI, 8.0% for SRR, and 5.9% for SR. The interobserver variabilities were 7.5% for TDI, 8.3% for SRR, and 6.3% for SR.
Strain parameters showed good reproducibility (intra- and interobserver variability) for SRR (r = 0.85 and 0.80, respectively) and SR (r = 0.85 and 0.79).
DISCUSSION
Our study shows that young patients with SLE, even in the absence of specific clinical complaints of heart disease, demonstrate abnormal systolic and diastolic LV longitudinal function. Tissue Doppler and strain imaging are accurate means to determine myocardial dysfunction, providing incremental findings in stages of the disease, where 2D echocardiography shows normal findings.
TDI and SRI are noninvasive techniques, widely used to detect subtle, asymptomatic myocardial functional abnormalities. They are useful and early indicators of LV dysfunction and allow a reliable screening for subclinical cardiac manifestations in patients with increased risk for cardiovascular diseases21,41. Our study suggests that these methods may be used in patients with SLE and can provide important further information.
Patients with SLE have an increased prevalence of subclinical LV dysfunction, which may be a prognostic indicator of cardiac morbidity and mortality. Mechanisms by which SLE might directly induce changes in LV structure and function are manifold and include underlying inflammatory processes leading to subclinical vasculitis, myocarditis or vascular stiffening, and preclinical CAD in SLE patients7,8,42.
Myocarditis is a characteristic feature of myocardial involvement in SLE43. However, since the advent of corticosteroid therapy, vasculitis and myocarditis have been rare findings in SLE patients who undergo autopsy44. Currently, myocarditis is reported in 7%–10% of cases. However, subclinical involvement for other cardiac manifestations is probably more frequent. Echocardiography findings, while not specific and sensitive, are suggestive of myocardial inflammation: observations include global or regional wall motion abnormalities, decreased ejection fraction, increased chamber size, and prolonged isovolumic relaxation time45. Cardiac magnetic resonance imaging (MRI) demonstrated that T2 relaxation times were significantly longer in patients with active SLE compared to healthy controls; such abnormalities are a sensitive indicator of myocardial disease even in the absence of myocardial involvement by clinical criteria46. Scintigraphy and MRI may be useful in the diagnosis of myocardial inflammation and myocarditis but are usually not used as a screening method in clinical routine.
Myocardial dysfunction in SLE may also be the consequence of other features, particularly CAD due to premature atherosclerosis, hypertension, renal failure, valvular disease, and toxicity from medications such as chloroquine7,8,47. But little is known about the prevalence of preclinical disease and associated factors. Previous evidence from autopsies and clinical studies has suggested that the prevalence of subclinical atherosclerosis is increased in patients with SLE47. Ventricular remodeling and subsequent LV functional changes may therefore result from premature development of atherosclerosis48,49. In SLE, reported CAD prevalence ranges from 6% to 10%7,50; and in young women, risk of myocardial infarction is increased 50-fold. These results are concordant with those of a retrospective study in which risk of adverse cardiovascular outcomes was observed to be increased by a factor of 7 to 17 in patients with SLE as compared with the Framingham cohort51. Different mechanisms play a role in the development of CAD. These include atherosclerosis of epimyocardial coronary arteries, coronary arteritis, thrombotic events, or vasospasm. Attempts to address the extent and severity of CAD in patients with SLE more directly have used single-photon-emission computed tomography (SPECT), detecting myocardial perfusion abnormalities in 35% of patients52. In previous studies, Tc-99m sestamibi myocardial perfusion SPECT showed high incidence of myocardial perfusion abnormalities in asymptomatic lupus patients without any clinical signs of cardiac involvement53. Whether SRI is valuable for the diagnosis or prognosis of CAD in SLE patients should be evaluated in further comparative prospective studies.
Alterations in LV structure and function have also been reported as cardiac manifestations of SLE, including echocardiographic evidence of increased LV wall thicknesses and LV mass, a decrease in LV ejection fraction, and impaired diastolic filling5,32,40,45. Although no SLE patients in our study had clinical signs of ischemic heart disease, decreased longitudinal LV function in SLE patients might be a reflection of preclinical ischemic myocardial disease. The use of tissue Doppler and strain imaging has shown a significant reduction of systolic and diastolic function of the LV, despite normal ejection fraction and cardiac output. Gradation was not noticeable for DT but was observed for E/e ratio, the prime parameter reflecting diastolic dysfunction. Our results are in agreement with the findings of Lee, et al, Sasson, et al, and Fujimoto, et al, who demonstrated a high incidence of LV diastolic dysfunction in patients with SLE32,33,48. Gin, et al34 used TDI to evaluate heart function in patients with SLE. A trend towards LV dysfunction was also observed in the SLE group. LV ejection fraction and peak systolic TDI of the mitral annulus was lower in SLE; however, this trend was not statistically significant. In a more detailed study by Crozier, et al5, greater LV wall thicknesses and mass and lower ejection fraction were found in 50 SLE patients compared with controls. In accord with our results, Yip and colleagues54 recently reported that patients with SLE had subclinical long and short-axis dysfunctions, using TDI of the basal segments of the LV. As described above, SR and SRR were reduced in our study, indicative of a form of heart failure with preserved ejection fraction. Also, Chow, et al recently showed significantly reduced longitudinal function detected by SRI values in young adolescents with pediatric-onset SLE31. In contrast to that study, we investigated young adults without pediatric-onset SLE. In addition to the significant findings, we focused further on LV longitudinal dysfunction in SLE. Of note, we observed that reduction of longitudinal myocardial dysfunction was associated with higher disease activity scores. SLE, in addition to traditional stimuli, augments LV dysfunction, possibly by a direct disease-related effect of SLE on LV structure and function.
In conclusion, asymptomatic patients with SLE already have reduced systolic and diastolic LV longitudinal function. Longitudinal LV function is significantly associated with enhanced disease activity. Damage of the LV seems to have multiple causes and thus implies a careful clinical evaluation of these patients. The clinical significance of this dysfunction needs to be established in longterm studies to determine whether detection of such abnormalities in otherwise asymptomatic subjects should affect their therapeutic management. Moreover, use of modern imaging techniques could advance our understanding of the prevalence and mechanisms of heart involvement in patients with SLE.
Footnotes
- Accepted for publication August 25, 2009.








{kind=link}
{kind=link}