
Serum α1-Proteinase Inhibitor, Calprotectin, and S100A12 Concentrations in the Characterization of Pancreatitis in Dogs
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mansfield, C. Pathophysiology of acute pancreatitis: Potential application from experimental models and human medicine to dogs. J. Vet. Intern. Med. 2012, 26, 875–887. [Google Scholar] [CrossRef]
- Cridge, H.; Sullivant, A.M.; Wills, R.W.; Lee, A.M. Association between abdominal ultrasound findings, the specific canine pancreatic lipase assay, clinical severity indices, and clinical diagnosis in dogs with pancreatitis. J. Vet. Intern. Med. 2020, 34, 636–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xenoulis, P.G. Diagnosis of pancreatitis in dogs and cats. J. Small Anim. Pract. 2015, 56, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Xenoulis, P.G.; Steiner, J.M. Canine and feline pancreatic lipase immunoreactivity. Vet. Clin. Pathol. 2012, 41, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Steiner, J.M.; Newman, S.; Xenoulis, P.G.; Woosley, K.; Suchodolski, J.; Williams, D.; Barton, L. Sensitivity of serum markers for pancreatitis in dogs with macroscopic evidence of pancreatitis. Vet. Ther. 2008, 9, 263–273. [Google Scholar]
- Trivedi, S.; Marks, S.L.; Kass, P.H.; Luff, J.A.; Keller, S.M.; Johnson, E.G.; Murphy, B. Sensitivity and specificity of canine pancreas-specific lipase (cPL) and other markers for pancreatitis in 70 dogs with and without histopathologic evidence of pancreatitis. J. Vet. Intern. Med. 2011, 25, 1241–1247. [Google Scholar] [CrossRef]
- Cridge, H.; Twedt, D.C.; Marolf, A.J.; Sharkey, L.C.; Steiner, J.M. Advances in the diagnosis of acute pancreatitis in dogs. J. Vet. Intern. Med. 2021, 35, 2572–2587. [Google Scholar] [CrossRef]
- Lim, S.Y.; Nakamura, K.; Morishita, K.; Sasaki, N.; Murakami, M.; Osuga, T.; Yokoyama, N.; Ohta, H.; Yamasaki, M.; Takiguchi, M. Quantitative contrast-enhanced ultrasonographic assessment of naturally occurring pancreatitis in dogs. J. Vet. Intern. Med. 2015, 29, 71–78. [Google Scholar] [CrossRef] [Green Version]
- French, J.M.; Twedt, D.C.; Rao, S.; Marolf, A.J. Computed tomographic angiography and ultrasonography in the diagnosis and evaluation of acute pancreatitis in dogs. J. Vet. Intern. Med. 2019, 33, 79–88. [Google Scholar] [CrossRef]
- Lidbury, J.A.; Suchodolski, J.S. New advances in the diagnosis of canine and feline liver and pancreatic disease. Vet. J. 2016, 215, 87–95. [Google Scholar] [CrossRef]
- Rhodes, B.; Fürnrohr, B.G.; Vyse, T.J. C-reactive protein in rheumatology: Biology and genetics. Nat. Rev. Rheumatol. 2011, 7, 282–289. [Google Scholar] [CrossRef]
- Mansfield, C.S.; James, F.E.; Robertson, I.D. Development of a clinical severity index for dogs with acute pancreatitis. J. Am. Vet. Med. Assoc. 2008, 233, 936–944. [Google Scholar] [CrossRef] [PubMed]
- Tvarijonaviciute, A.; García-Martínez, J.D.; Caldin, M.; Martínez-Subiela, S.; Tecles, F.; Pastor, J.; Ceron, J.J. Serum paraoxonase 1 (PON1) activity in acute pancreatitis of dogs. J. Small Anim. Pract. 2015, 56, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, H.J.; Kang, J.H.; Kang, B.T.; Yang, M.P. Evaluation of serum C-reactive protein and high mobility group box 1 concentrations in 22 dogs with acute pancreatitis: A pilot study. Vet. Q. 2019, 39, 122–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keany, K.; Fosgate, G.T.; Perry, S.M.; Stroup, S.T.; Steiner, J.M. Serum concentrations of canine pancreatic lipase immunoreactivity and C-reactive protein for monitoring disease progression in dogs with acute pancreatitis. J. Vet. Intern. Med. 2021, 35, 2187–2195. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Ohno, K.; Tamamoto, T.; Oishi, M.; Kanemoto, H.; Fukushima, K.; Goto-Koshino, Y.; Takahashi, M.; Tsujimoto, H. Assessment of severity and changes in C-reactive protein concentration and various biomarkers in dogs with pancreatitis. J. Vet. Med. Sci. 2017, 79, 35–40. [Google Scholar] [CrossRef] [Green Version]
- Gori, E.; Pierini, A.; Lippi, I.; Ceccherini, G.; Perondi, F.; Marchetti, V. Evaluation of C-reactive protein/albumin ratio and its relationship with survival in dogs with acute pancreatitis. N. Z. Vet. J. 2020, 68, 345–348. [Google Scholar] [CrossRef]
- Steiner, J.M. Canine pancreatic disease. In Textbook of Veterinary Internal Medicine, 7th ed.; Ettinger, S.J., Feldman, E.C., Eds.; Elsevier Saunders: St. Louis, MO, USA, 2010; pp. 1695–1704. [Google Scholar]
- Steiner, J.M.; Teague, S.R.; Williams, D.A. Development and analytic validation of an enzyme-linked immunosorbent assay for the measurement of canine pancreatic lipase immunoreactivity in serum. Can. J. Vet. Res. 2003, 67, 175–182. [Google Scholar]
- Xenoulis, P.G.; Suchodolski, J.S.; Ruaux, C.G.; Steiner, J.M. Association between serum triglyceride and canine pancreatic lipase immunoreactivity concentrations in Miniature Schnauzers. J. Am. Anim. Hosp. Assoc. 2010, 46, 229–234. [Google Scholar] [CrossRef]
- Xenoulis, P.G.; Levinski, M.D.; Suchodolski, J.S.; Steiner, J.M. Serum triglyceride concentrations in Miniature Schnauzers with and without a history of probable pancreatitis. J. Vet. Intern. Med. 2011, 25, 20–25. [Google Scholar] [CrossRef]
- Xenoulis, P.G.; Suchodolski, J.S.; Levinski, M.D.; Steiner, J.M. Investigation of hypertriglyceridemia in healthy Miniature Schnauzers. J. Vet. Intern. Med. 2007, 21, 1224–1230. [Google Scholar] [CrossRef] [PubMed]
- Bishop, M.A.; Steiner, J.M.; Moore, L.E.; Williams, D.A. Evaluation of the cationic trypsinogen gene for potential mutations in Miniature Schnauzers with pancreatitis. Can. J. Vet. Res. 2004, 68, 315–318. [Google Scholar]
- Bishop, M.A.; Xenoulis, P.G.; Levinski, M.D.; Suchodolski, J.S.; Steiner, J.M. Identifications of variants of the SPINK1 gene and their association with pancreatitis in Miniature Schnauzers. Am. J. Vet. Res. 2010, 71, 527–533. [Google Scholar] [CrossRef]
- Xenoulis, P.G.; Steiner, J.M. Canine hyperlipidemia. J. Small Anim. Pract. 2015, 56, 595–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hess, R.S.; Kass, P.H.; Shofer, F.S.; Van Winkle, T.J.; Washabau, R.J. Evaluation of risk factors for fatal acute pancreatitis in dogs. J. Am. Vet. Med. Assoc. 1999, 214, 46–51. [Google Scholar] [PubMed]
- Cook, A.K.; Breitschwerdt, E.B.; Levine, J.F.; Bunch, S.E.; Linn, L.O. Risk factors associated with acute pancreatitis in dogs: 101 cases (1985–1990). J. Am. Vet. Med. Assoc. 1993, 203, 673–679. [Google Scholar] [PubMed]
- Yadav, D.; Pitchumoni, C.S. Issues in hyperlipidemic pancreatitis. J. Clin. Gastroenterol. 2003, 36, 54–62. [Google Scholar] [CrossRef]
- Xenoulis, P.G.; Steiner, J.M. Lipid metabolism and hyperlipidemia in dogs. Vet. J. 2010, 183, 12–21. [Google Scholar] [CrossRef]
- Furrow, E.; Jaeger, J.Q.; Parker, V.J.; Hinchcliff, K.W.; Johnson, S.E.; Murdoch, S.J.; de Boer, I.H.; Sherding, R.G.; Brunzell, J.D. Proteinuria and lipoprotein lipase activity in Miniature Schnauzer dogs with and without hypertriglyceridemia. Vet. J. 2016, 212, 83–89. [Google Scholar] [CrossRef] [Green Version]
- Xenoulis, P.G.; Levinski, M.D.; Suchodolski, J.S.; Steiner, J.M. Association of hypertriglyceridemia with insulin resistance in healthy Miniature Schnauzers. J. Am. Vet. Med. Assoc. 2011, 238, 1011–1016. [Google Scholar] [CrossRef]
- Xenoulis, P.G.; Heilmann, R.M.; Stavroulaki, E.M.; Riggers, D.S.; Gneipel, L.J.; Suchodolski, J.S.; Steiner, J.M. Associations among serum insulin, calprotectin, and C-reactive protein concentrations in Miniature Schnauzers with idiopathic hyperlipidemia before and after feeding an ultra-low-fat diet. J. Vet. Intern. Med. 2022, 36, 910–918. [Google Scholar] [CrossRef] [PubMed]
- Heilmann, R.M.; Xenoulis, P.G.; Müller, K.; Stavroulaki, E.M.; Suchodolski, J.S.; Steiner, J.M. Association of serum calprotectin (S100A8/A9) concentrations and idiopathic hyperlipidemia in Miniature Schnauzers. J. Vet. Intern. Med. 2019, 33, 578–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xenoulis, P.G.; Cammarata, P.J.; Walzem, R.L.; Suchodolski, J.S.; Steiner, J.M. Effect of a low-fat diet on serum triglyceride and cholesterol concentrations and lipoprotein profiles in Miniature Schnauzers with hypertriglyceridemia. J. Vet. Intern. Med. 2020, 34, 2605–2616. [Google Scholar] [CrossRef] [PubMed]
- Grützner, N.; Heilmann, R.M.; Suchodolski, J.S.; Steiner, J.M. Serum concentrations of canine alpha1-proteinase inhibitor in Yorkshire Terriers with and without cobalamin deficiency. J. Vet. Diagn. Investig. 2012, 26, 376–385. [Google Scholar]
- Heilmann, R.M.; Ruaux, C.G.; Grützner, N.; Cranford, S.M.; Bridges, C.S.; Steiner, J.M. Biological variation of serum canine calprotectin concentrations as measured by ELISA in healthy dogs. Vet. J. 2019, 247, 61–64. [Google Scholar] [CrossRef]
- Heilmann, R.M.; Lanerie, D.J.; Ruaux, C.G.; Grützner, N.; Suchodolski, J.S.; Steiner, J.M. Development and analytic validation of an immunoassay for the quantification of canine S100A12 in serum and fecal samples and its biological variability in serum from healthy dogs. Vet. Immunol. Immunopathol. 2011, 144, 200–209. [Google Scholar] [CrossRef]
- Heilmann, R.M.; Ruaux, C.G.; Burgener, I.A.; Hern, J.D.; Suchodolski, J.S.; Steiner, J.M. Serum alpha1-proteinase inhibitor concentrations in healthy dogs—Method validation and determination of reference interval and intra-individual variation. Vet. Clin. Pathol. 2013, 42, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Ruaux, C.G. Diagnostic approaches to acute pancreatitis. Clin. Tech. Small Anim. Pract. 2003, 18, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Hedstrom, J.; Sainio, V.; Kemppainen, E.; Haapiainen, R.; Kivilaakso, E.; Schroder, T.; Leinonen, J.; Stenman, U.H. Serum complex of trypsin 2 and alpha 1 antitrypsin as diagnostic and prognostic marker of acute pancreatitis: Clinical study in consecutive patients. BMJ 1996, 313, 333–337. [Google Scholar] [CrossRef]
- Heilmann, R.M.; Grützner, N.; Thames, B.E.; Steiner, J.M.; Barr, J.W. Serum alpha1-proteinase inhibitor concentrations in dogs with systemic inflammatory response syndrome or sepsis. J. Vet. Emerg. Crit. Care 2017, 27, 674–683. [Google Scholar] [CrossRef]
- Kuzi, S.; Mazaki-Tovi, M.; Suchodolski, J.S.; Rimer, D.; Lidbury, J.A.; Steiner, J.M.; Buono, A.; Nivy, R.; Segev, G.; Aroch, I. Protease inhibitors, inflammatory markers, and their association with outcome in dogs with naturally occurring acute pancreatitis. J. Vet. Intern. Med. 2020, 34, 1801–1812. [Google Scholar] [CrossRef] [PubMed]
- Lasson, Å.; Ohlsson, K. Protease inhibitors in acute human pancreatitis correlation between biochemical changes and clinical course. Scand. J. Gastroenterol. 1984, 19, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Karşıdağ, T.; Tüzün, S.; Kemik, A.S.; Purisa, S.; Unlü, A. Alpha-1 protease inhibitor and antichymotrypsin levels in acute pancreatitis. Turk. J. Trauma Emerg. Surg. 2012, 18, 195–199. [Google Scholar] [CrossRef] [Green Version]
- Borgström, A.; Lasson, A. Trypsin-alpha1-protease inhibitor complexes in serum and clinical course of acute pancreatitis. Scand. J. Gastroenterol. 1984, 19, 1119–1122. [Google Scholar]
- Lorenz, E.; Muhlebach, M.S.; Tessier, P.A.; Alexis, N.E.; Hite, R.D.; Seeds, M.C.; Peden, D.B.; Meredith, W. Different expression ratio of S100A8/A9 and S100A12 in acute and chronic lung diseases. Respir. Med. 2008, 102, 567–573. [Google Scholar] [CrossRef] [Green Version]
- Heilmann, R.M.; Grützner, N.; Hokamp, J.A.; Lidbury, J.A.; Xenoulis, P.G.; Suchodolski, J.S.; Nabity, M.B.; Ciancolo, R.; Steiner, J.M. Serum alpha1-proteinase inhibitor concentrations in dogs with exocrine pancreatic disease, chronic hepatitis or proteinuric chronic kidney disease. Vet. J. 2018, 236, 68–71. [Google Scholar] [CrossRef]
- Ruaux, C.G.; Atwell, R.B. A severity score for spontaneous canine acute pancreatitis. Aust. Vet. J. 1998, 76, 804–808. [Google Scholar] [CrossRef]
- Fabrès, V.; Dossin, O.; Reif, C.; Campos, M.; Freiche, V.; Maurey, C.; Pilot-Storck, F.; Desquilbet, L.; Benchekroun, G. Development and validation of a novel clinical scoring system for short-term prediction of death in dogs with acute pancreatitis. J. Vet. Intern. Med. 2019, 33, 499–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Parameter | Typical Clinical Presentation (Group A) # | Atypical Clinical Presentation (Group B) | p-Value |
|---|---|---|---|
| Patient characteristics | |||
| Age (in years) | 8.9 (1.7–12.7) | 9.1 (3.3–14.6) | 0.4492 |
| Body weight (in kg) | 9.2 (6.2–13.3) | 8.6 (6.4–14.2) | 0.7031 |
| Sex (female/male) | 7/11 | 5/2 | 0.1394 |
| No. of clinical signs $ | 4 (0–5) | 3 (0–5) | 0.8194 |
| Vomiting | 13/17 (76%) | 4/7 (57%) | 0.3527 |
| Diarrhea | 5/17 (29%) | 3/7 (43%) | 0.5298 |
| Abdominal pain | 10/17 (59%) | 2/7 (29%) | 0.1726 |
| Anorexia | 7/17 (41%) | 5/7 (71%) | 0.1726 |
| Depression | 10/17 (59%) | 6/7 (86%) | 0.1826 |
| Hypertriglyceridemia † | 12/16 (75%) | 2/5 (40%) | 0.1564 |
| Medications associated with the risk of pancreatitis † | 0/15 (0%) | 1/6 (17%) | 0.1046 |
| Euthanasia | 1/18 (6%) | 0/7 (0%) | 0.412 |
| Serum biomarkers | |||
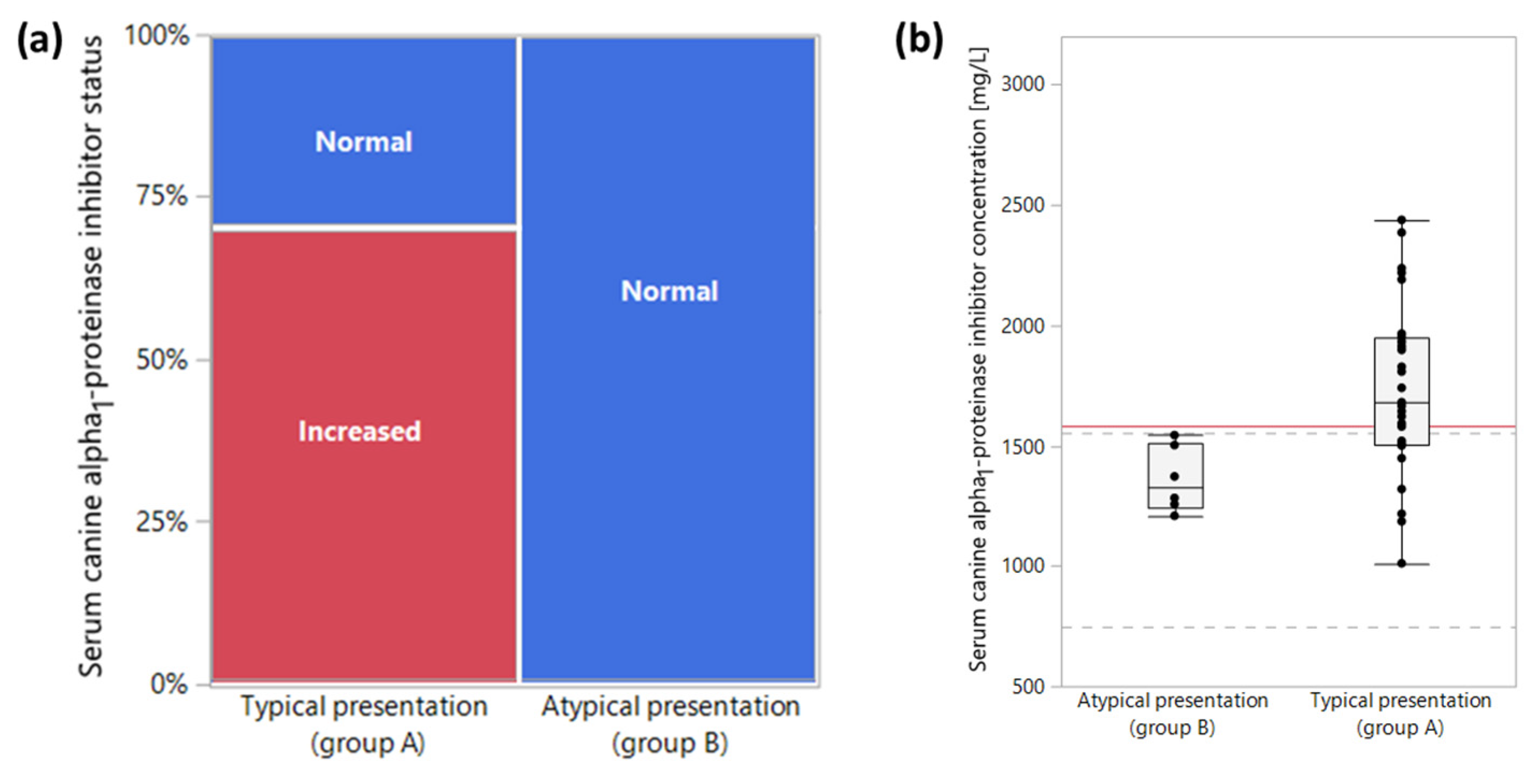
| Serum α1PI ‡ | 1680 (1011–2428) mg/L | 1327 (1208–1543) mg/L | 0.011 |
| Increased serum α1PI ‡ | 19/27 (70%) | 0/6 (0%) | 0.0005 |
| Serum calprotectin | 16.6 (1.2–269.7) mg/L | 7.2 (1.3–101.2) mg/L | 0.5227 |
| Hypercalprotectinemia | 11/28 (39%) | 4/7 (57%) | 0.3954 |
| Serum S100A12 | 266 (16 –6464) μg/L | 190 (77–2713) μg/L | 0.6952 |
| Increased serum S100A12 | 11/28 (39%) | 4/7 (57 %) | 0.3954 |
| Serum calprotectin-to-S100A12 ratio | 52.4 (20.8–84.8) | 38.1 (16.9–58.9) | 0.0606 |
| Parameter Correlated with | Serum α1PI | Serum Calprotectin | Serum S100A12 |
|---|---|---|---|
| Serum α1PI | 0.48 (0.0047) | 0.44 (0.0112) | |
| Serum calprotectin | 0.48 (0.0047) | 0.94 (<0.0001) | |
| Serum S100A12 | 0.44 (0.0112) | 0.94 (<0.0001) | |
| Age | −0.26 (0.2291) | 0.05 (0.8322) | 0.04 (0.8652) |
| Body weight | −0.24 (0.2784) | −0.31 (0.1363) | −0.39 (0.0586) |
| No. of clinical signs | −0.20 (0.3745) | −0.53 (0.0377) | −0.49 (0.0149) |
| Parameter | Serum α1PI | Serum Calprotectin | Serum S100A12 | Serum Calprotectin-to-S100A12 Ratio |
|---|---|---|---|---|
| No. of clinical signs $ | 0.3745 | 0.0377 a | 0.0149 a | 0.778 |
| Vomiting | 0.6953 | 0.0188 a | 0.0133 a | 0.6566 |
| Diarrhea | 0.8112 | 0.1046 | 0.1335 | 0.1046 |
| Abdominal pain | 0.4483 | 0.2366 | 0.0885 a | 0.4025 |
| Anorexia | 0.3933 | 0.6236 | 0.4357 | 0.665 |
| Lethargy | 0.2308 | 0.0708 a | 0.0537 a | 0.7363 |
| Hypertriglyceridemia † | 0.3139 | 0.4334 | 0.4334 | 0.351 |
| Medication(s) known to be associated with pancreatitis † | – | 0.2155 | 0.1167 | 0.8044 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jandel, A.N.; Heilmann, R.M.; Sander, H.; Steiner, J.M.; Grützner, N.; Xenoulis, P.G. Serum α1-Proteinase Inhibitor, Calprotectin, and S100A12 Concentrations in the Characterization of Pancreatitis in Dogs. Vet. Sci. 2023, 10, 428. https://doi.org/10.3390/vetsci10070428
Jandel AN, Heilmann RM, Sander H, Steiner JM, Grützner N, Xenoulis PG. Serum α1-Proteinase Inhibitor, Calprotectin, and S100A12 Concentrations in the Characterization of Pancreatitis in Dogs. Veterinary Sciences. 2023; 10(7):428. https://doi.org/10.3390/vetsci10070428
Chicago/Turabian StyleJandel, Annina N., Romy M. Heilmann, Henri Sander, Jörg M. Steiner, Niels Grützner, and Panagiotis G. Xenoulis. 2023. "Serum α1-Proteinase Inhibitor, Calprotectin, and S100A12 Concentrations in the Characterization of Pancreatitis in Dogs" Veterinary Sciences 10, no. 7: 428. https://doi.org/10.3390/vetsci10070428