Relationship between Citizens’ Health Engagement and Intention to Take the COVID-19 Vaccine in Italy: A Mediation Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.3. Statistical Analyses
- Configural invariance: is the model’s structure equal across groups?
- Weak invariance: are regressions between variables equal across groups?
- Strong invariance: are intercepts equal across groups?
- Strict invariance: are residuals equal across groups?
2.4. Ethics
3. Results
3.1. Sample Characteristics
3.2. Descriptive Statistics and Reliability
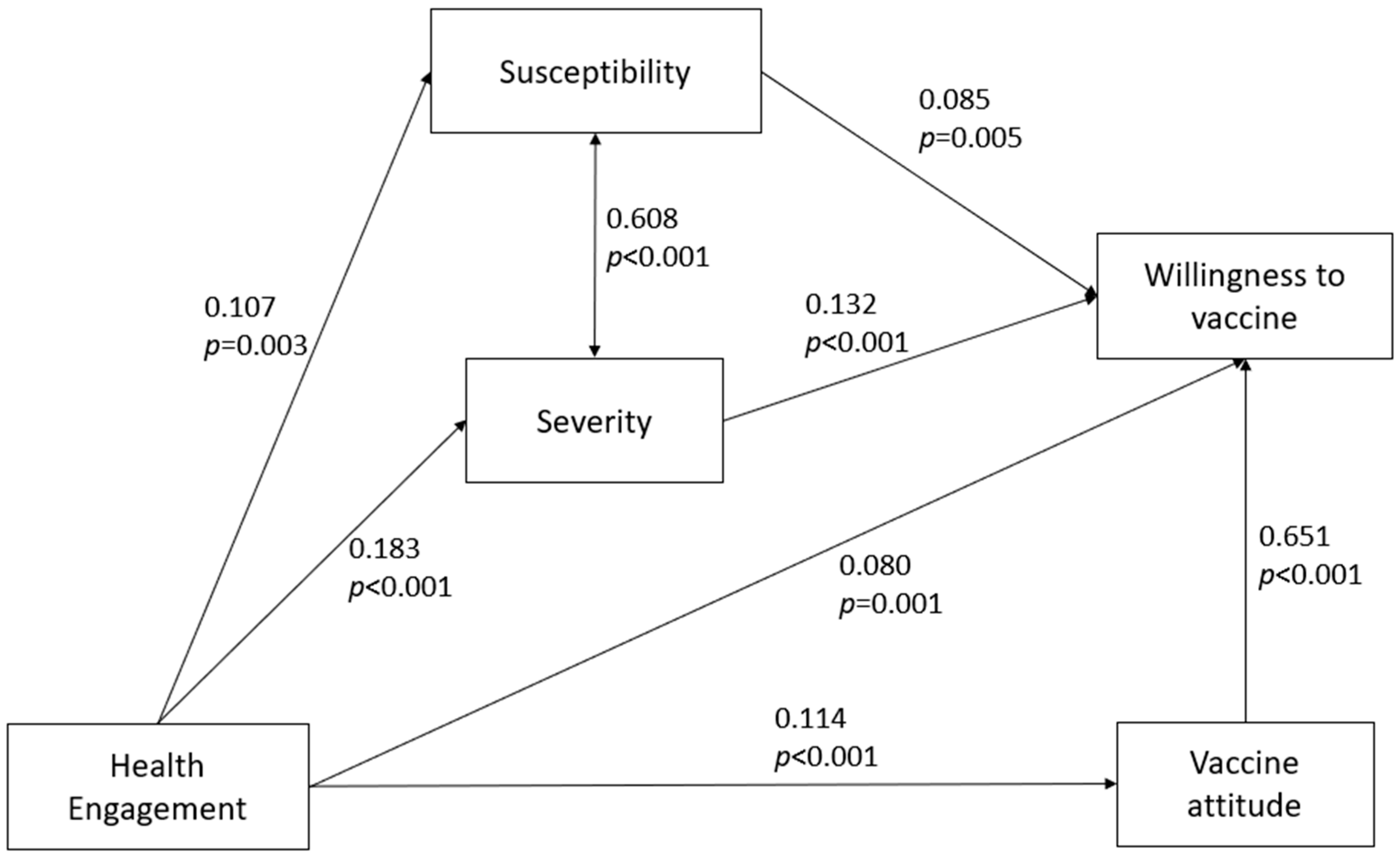
3.3. Path Analysis
3.4. Invariance Analysis
4. Discussion
5. Conclusion and Limitations
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization Ten Threats to Global Health in 2019. Available online: https://www.who.int/vietnam/news/feature-stories/detail/ten-threats-to-global-health-in-2019 (accessed on 23 September 2020).
- Eastwood, K.; Durrheim, D.N.; Jones, A.; Butler, M. Acceptance of pandemic (H1N1) 2009 influenza vaccination by the Australian public. Med. J. Aust. 2010. [Google Scholar] [CrossRef]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020. [Google Scholar] [CrossRef]
- Barello, S.; Nania, T.; Dellafiore, F.; Graffigna, G.; Caruso, R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur. J. Epidemiol. 2020. [Google Scholar] [CrossRef]
- Harrison, E.A.; Wu, J.W. Vaccine confidence in the time of COVID-19. Eur. J. Epidemiol. 2020, 35, 325–330. [Google Scholar] [CrossRef] [Green Version]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020. [Google Scholar] [CrossRef]
- Guidry, J.P.D.; Carlyle, K.E.; Perrin, P.B.; LaRose, J.G.; Ryan, M.; Messner, M. A path model of psychosocial constructs predicting future Zika vaccine uptake intent. Vaccine 2019, 37, 5233–5241. [Google Scholar] [CrossRef]
- Looijmans-van den Akker, I.; Hulscher, M.E.; Verheij, T.J.; Riphagen-Dalhuisen, J.; van Delden, J.J.; Hak, E. How to develop a program to increase influenza vaccine uptake among workers in health care settings? Implement. Sci. 2011, 6, 47. [Google Scholar] [CrossRef] [Green Version]
- Ng, T.W.Y.; Cowling, B.J.; So, H.C.; Ip, D.K.M.; Liao, Q. Testing an integrative theory of health behavioural change for predicting seasonal influenza vaccination uptake among healthcare workers. Vaccine 2020, 38, 690–698. [Google Scholar] [CrossRef]
- Halvorsen, K.; Dihle, A.; Hansen, C.; Nordhaug, M.; Jerpseth, H.; Tveiten, S.; Joranger, P.; Ruud Knutsen, I. Empowerment in healthcare: A thematic synthesis and critical discussion of concept analyses of empowerment. Patient Educ. Couns. 2020, 103, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Babazadeh, T.; Nadrian, H.; Ranjbaran, S.; Rezakhani-Moghaddam, H.; Aghemiri, M. Cognitive factors associated with brucellosis preventive behaviours among diagnosed patients: An application of empowerment model. East. Mediterr. Health J. 2019. [Google Scholar] [CrossRef] [PubMed]
- Castellini, G.; Savarese, M.; Leone, S.; Previtali, E.; Armuzzi, A.; Graffigna, G. Italian IBD Patients coping with Covid-19 emergency: The mitigating role of psychological readiness to engage in self-care. Inflamm. Bowel Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Nania, T.; Dellafiore, F.; Caruso, R.; Barello, S. Risk and protective factors for psychological distress among Italian university students during the COVID-19 pandemic: The beneficial role of health engagement. Int. J. Soc. Psychiatr. 2020. [Google Scholar] [CrossRef]
- Graffigna, G.; Barello, S.; Savarese, M.; Palamenghi, L.; Castellini, G.; Bonanomi, A.; Lozza, E. Measuring Italian citizens’ engagement in the first wave of the COVID-19 pandemic containment measures: A cross-sectional study. PLoS ONE 2020, 15, e0238613. [Google Scholar] [CrossRef]
- Politi, M.C.; Jones, K.M.; Philpott, S.E. The role of patient engagement in addressing parents’ perceptions about immunizations. JAMA-J. Am. Med. Assoc. 2017. [Google Scholar] [CrossRef]
- Rosseel, Y. Lavaan: An R package for structural equation modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Schumacker, R.E.; Lomax, R.G. A Beginner’s Guide to Structural Equation Modeling, 2nd ed.; Lawrence Erlbaum Associates: Mahwan, India, 2004. [Google Scholar]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural equation modelling: Guidelines for determining model fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Lavaan Tutorial. Available online: https://lavaan.ugent.be/tutorial/est.html (accessed on 18 July 2020).
- Vandenberg, R.J.; Lance, C.E. A review and synthesis of the measurement invariance literature: Suggestions, practices, and recommendations for organizational research. Organ. Res. Methods 2000, 3, 4–70. [Google Scholar] [CrossRef]
- Widaman, K.F.; Early, D.R.; Conger, R.D. Special populations. In The Oxford Handbook of Quantitative Methods: Foundations; Little, T.D., Ed.; Oxford University Press: Oxford, MS, USA, 2014; Volume 1. [Google Scholar]
- Bollen, K.A. A new incremental fit index for general structural equation models. Sociol. Methods Res. 1989, 17, 303–316. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct. Equ. Model. Multidiscip. J. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Chen, F.F. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct. Equ. Model. Multidiscip. J. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Kenny, D.A.; Kaniskan, B.; McCoach, D.B. The performance of RMSEA in models with small degrees of freedom. Sociol. Methods Res. 2015, 44, 486–507. [Google Scholar] [CrossRef]
- Peretti-Watel, P.; Seror, V.; Cortaredona, S.; Launay, O.; Raude, J.; Verger, P.; Fressard, L.; Beck, F.; Legleye, S.; L’Haridon, O.; et al. A future vaccination campaign against COVID-19 at risk of vaccine hesitancy and politicisation. Lancet Infect. Dis. 2020, 20, 769–770. [Google Scholar] [CrossRef]
- Thunstrom, L.; Ashworth, M.; Finnoff, D.; Newbold, S. Hesitancy towards a COVID-19 Vaccine and prospects for herd immunity. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Feleszko, W.; Lewulis, P.; Czarnecki, A.; Waszkiewicz, P. Flattening the curve of COVID-19 vaccine rejection—A global overview. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Hibbard, J.H.; Greene, J. What the evidence shows about patient activation: Better health outcomes and care experiences; fewer data on costs. Health Aff. 2013. [Google Scholar] [CrossRef]
- Skrine Jeffers, K.; Castellon-Lopez, Y.; Grotts, J.; Mangione, C.M.; Moin, T.; Tseng, C.H.; Turk, N.; Frosch, D.L.; Norris, K.C.; Duke, C.C.; et al. Diabetes prevention program attendance is associated with improved patient activation: Results from the prediabetes informed decisions and education (PRIDE) study. Prev. Med. Rep. 2019. [Google Scholar] [CrossRef]
- Katz, M.L.; Fisher, J.L.; Fleming, K.; Paskett, E.D. Patient activation increases colorectal cancer screening rates: A randomized trial among low-income minority patients. Cancer Epidemiol. Biomark. Prev. 2012. [Google Scholar] [CrossRef] [Green Version]
- Glanz, J.M.; Kraus, C.R.; Daley, M.F. Addressing parental vaccine concerns: Engagement, balance, and timing. PLoS Biol. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, S. The Psychology of Pandemics: Preparing for the Next Global Outbreak of Infectious Disease; Cambridge Scholars Publishing: Newcastle upon Tyne, UK, 2019. [Google Scholar]
- Dubé, E.; Gagnon, D.; MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; et al. Strategies intended to address vaccine hesitancy: Review of published reviews. Vaccine 2015, 33, 4191–4203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weissberg, R.P.; Elias, M.J. Enhancing young people’s social competence and health behavior: An important challenge for educators, scientists, policymakers, and funders. Appl. Prev. Psychol. 1993. [Google Scholar] [CrossRef]
- MacPhail, C. Challenging dominant norms of masculinity for HIV prevention. Afr. J. AIDS Res. 2003. [Google Scholar] [CrossRef]
- WHO. Key Messages and Actions for COVID-19 Prevention and Control in Schools; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Sardu, C.; D’Onofrio, N.; Balestrieri, M.L.; Barbieri, M.; Rizzo, M.R.; Messina, V.; Maggi, P.; Coppola, N.; Paolisso, G.; Marfella, R. Outcomes in patients with hyperglycemia affected by COVID-19: Can we do more on glycemic control? Diabetes Care 2020, 43, 1408–1415. [Google Scholar] [CrossRef]
- Sardu, C.; Maggi, P.; Messina, V.; Iuliano, P.; Sardu, A.; Iovinella, V.; Paolisso, G.; Marfella, R. Could anti-hypertensive drug therapy affect the clinical prognosis of hypertensive patients with COVID-19 infection? Data from centers of Southern Italy. J. Am. Heart Assoc. 2020, 9. [Google Scholar] [CrossRef]
- Dubé, E.; Gagnon, D.; Nickels, E.; Jeram, S.; Schuster, M. Mapping vaccine hesitancy-Country-specific characteristics of a global phenomenon. Vaccine 2014. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable Sub Variable | (n)% |
|---|---|
| Gender | |
| Male | 49.1 (n = 493) |
| Female | 50.9 (n = 511) |
| Age group | |
| 18–38 | 34.4 (n = 345) |
| 39–52 | 33.6 (n = 337) |
| >52 | 32.1 (n = 322) |
| Geographical region | |
| North-west | 26.3 (n = 264) |
| North-east | 18.6 (n = 187) |
| Center | 19.7 (n = 198) |
| South and islands | 35.4 (n = 355) |
| Education | |
| No high school | 12.5 (n = 126) |
| High school | 60.0 (n = 602) |
| University or higher | 27.5 (n = 276) |
| Willingness to vaccinate | |
| Not likely at all | 8.6 (n = 86) |
| Unlikely | 6.7 (n = 67) |
| Not likely or unlikely | 26.2 (n = 263) |
| Very likely | 33.3 (n = 334) |
| Absolutely likely | 25.3 (n = 254) |
| Variable Name | Mean | Standard Deviation | Skewness | Kurtosis |
|---|---|---|---|---|
| Health Engagement | 3.62 | 0.59 | −0.031 | 0.221 |
| Vaccine attitude | 3.37 | 0.89 | −0.220 | 0.218 |
| Perceived Severity | 7.51 | 2.06 | −1.076 | 1.173 |
| Perceived Susceptibility | 3.08 | 0.96 | −0.174 | −0.230 |
| Willingness to vaccinate | 3.60 | 1.18 | −0.684 | −0.229 |
| Path | Std. Estimate | p-Value |
|---|---|---|
| Health engagement -> Willingness to vaccinate | 0.080 | <0.001 |
| Health engagement -> Susceptibility -> Willingness to vaccinate | 0.009 | 0.039 |
| Health engagement -> Severity -> Willingness to vaccinate | 0.024 | 0.001 |
| Health engagement -> Attitude towards vaccine -> Willingness to vaccinate | 0.074 | <0.001 |
| Total health engagement effect (indirect effect + direct effect) | 0.188 | <0.001 |
| Gender | Age | ||||
|---|---|---|---|---|---|
| Parameters | Configural | Weak | Configural | Weak | Weak Partial 2 |
| Robust χ2(df) | 10.533(4) | 18.854(12) | 12.015(6) | 41.365(22) | 28.875(21) |
| p-value | 0.032 | 0.092 | 0.062 | 0.007 | 0.177 |
| RMSEA (90% C.I.) | 0.072 (0.035–0.114) | 0.044 (0.016–0.070) | 0.071 (0.031–0.114) | 0.062 (0.039–0.085) | 0.045 (0.015–0.070) |
| CFI | 0.991 | 0.991 | 0.992 | 0.977 | 0.989 |
| SRMR | 0.026 | 0.038 | 0.03 | 0.058 | 0.047 |
| Δχ2(Δdf) 1 | 7.607(8) | 29.232(16) | 16.204(15) | ||
| p-value | 0.47 | 0.022 | 0.368 | ||
| ΔCFI | −0.015 | −0.003 | |||
| ΔRMSEA | −0.028 | −0.009 | −0.026 | ||
| ΔSRMR | 0.012 | 0.028 | 0.017 | ||
| Path | Younger | Middle Aged | Elderly | |||
|---|---|---|---|---|---|---|
| Std. Estimate | p-Value | Std. Estimate | p-Value | Std. Estimate | p-Value | |
| Susceptibility <-> Severity | 0.583 | <0.001 | 0.644 | <0.001 | 0.595 | <0.001 |
| Health Engagement -> Susceptibility | 0.127 | 0.028 | 0.108 | 0.101 | 0.081 | 0.137 |
| Health Engagement -> Severity | 0.194 | 0.003 | 0.170 | 0.009 | 0.161 | 0.003 |
| Health Engagement -> Attitude towards vaccine | 0.114 | 0.042 | 0.067 | 0.242 | 0.190 | 0.002 |
| Susceptibility -> Willingness to vaccinate | 0.010 | 0.844 | 0.201 | <0.001 | 0.029 | 0.586 |
| Severity -> Willingness to vaccinate | 0.096 | 0.075 | 0.140 | 0.016 | 0.196 | <0.001 |
| Attitude towards vaccine -> Willingness to vaccinate | 0.621 | <0.001 | 0.608 | <0.001 | 0.703 | <0.001 |
| Health Engagement -> Willingness to vaccinate | 0.134 | 0.002 | 0.072 | 0.073 | 0.032 | 0.369 |
| Health Engagement -> Susceptibility -> Willingness to vaccinate | 0.001 | 0.845 | 0.022 | 0.133 | 0.002 | 0.601 |
| Health Engagement -> Severity -> Willingness to vaccinate | 0.019 | 0.108 | 0.024 | 0.057 | 0.013 | 0.032 |
| Health Engagement -> Attitude towards vaccine -> Willingness to vaccinate | 0.071 | 0.044 | 0.041 | 0.240 | 0.134 | 0.002 |
| Total effect of Health Engagement on Willingness to vaccinate | 0.244 | <0.001 | 0.158 | 0.010 | 0.200 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Graffigna, G.; Palamenghi, L.; Boccia, S.; Barello, S. Relationship between Citizens’ Health Engagement and Intention to Take the COVID-19 Vaccine in Italy: A Mediation Analysis. Vaccines 2020, 8, 576. https://doi.org/10.3390/vaccines8040576
Graffigna G, Palamenghi L, Boccia S, Barello S. Relationship between Citizens’ Health Engagement and Intention to Take the COVID-19 Vaccine in Italy: A Mediation Analysis. Vaccines. 2020; 8(4):576. https://doi.org/10.3390/vaccines8040576
Chicago/Turabian StyleGraffigna, Guendalina, Lorenzo Palamenghi, Stefania Boccia, and Serena Barello. 2020. "Relationship between Citizens’ Health Engagement and Intention to Take the COVID-19 Vaccine in Italy: A Mediation Analysis" Vaccines 8, no. 4: 576. https://doi.org/10.3390/vaccines8040576