

Serology Assays Used in SARS-CoV-2 Seroprevalence Surveys Worldwide: A Systematic Review and Meta-Analysis of Assay Features, Testing Algorithms, and Performance
 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Serological Assay Data Extraction
2.4. Analysis
2.5. Modeling Analysis
3. Results
3.1. Included Studies
3.2. Assay Use in Seroprevalence Studies
3.3. Characteristics of Identified Assays
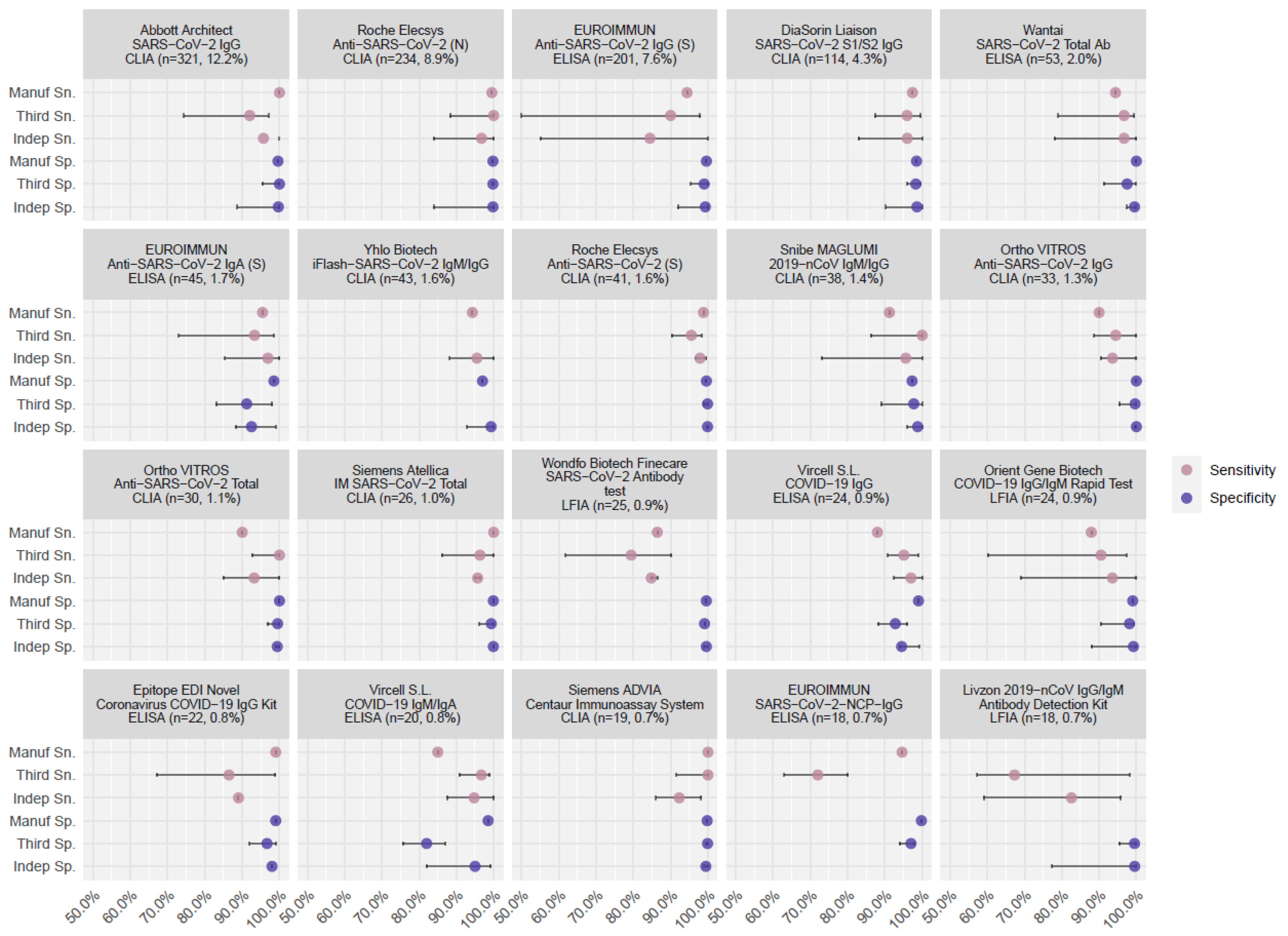
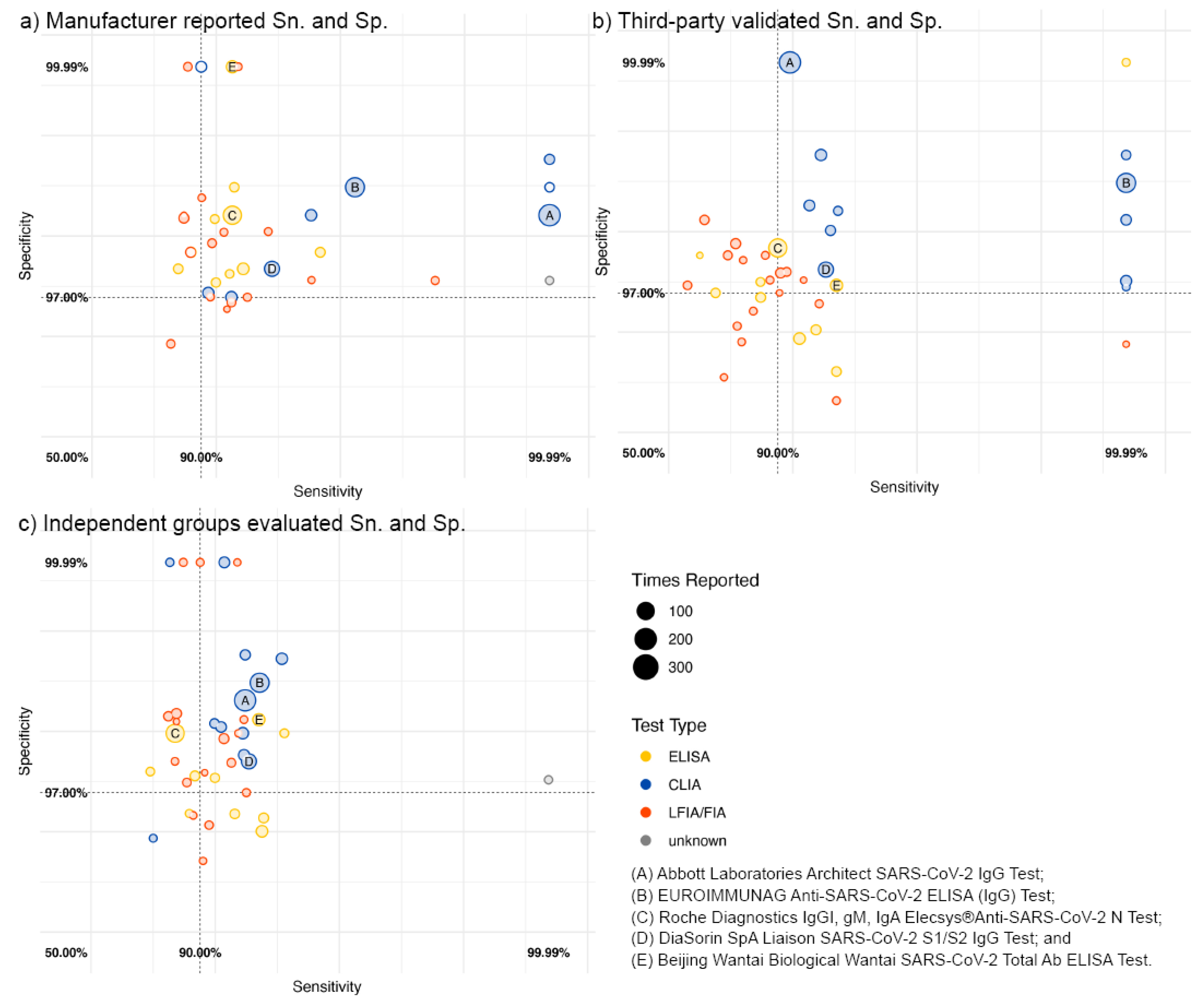
3.4. Reporting of Assay Performance
3.5. Multiple Test Combinations
4. Discussion
4.1. Third-Party Evaluation Validates Manufacturer Data
4.2. Independent Evaluation Reflects Regional Population Characteristics
4.3. Correct Seroprevalence Estimate for Assay Performance
4.4. Multiple Testing
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peeling, R.W.; Wedderburn, C.J.; Garcia, P.J.; Boeras, D.; Fongwen, N.; Nkengasong, J.; Sall, A.; Tanuri, A.; Heymann, D.L. Serology Testing in the COVID-19 Pandemic Response. Lancet Infect. Dis. 2020, 20, e245–e249. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, A.; Meurant, R.; Ardakani, A. COVID-19 Serological Tests: How Well Do They Actually Perform? Diagnostics 2020, 10, 453. [Google Scholar] [CrossRef] [PubMed]
- Makoah, N.A.; Tipih, T.; Litabe, M.M.; Brink, M.; Sempa, J.B.; Goedhals, D.; Burt, F.J. A Systematic Review and Meta-Analysis of the Sensitivity of Antibody Tests for the Laboratory Confirmation of COVID-19. Future Virol. 2021, 17, 119–139. [Google Scholar] [CrossRef] [PubMed]
- NRL Science of Quality. WHO SARS-CoV-2 Test Kit Comparative Study; NRL Science of Quality: Melbourne, Australia, 2020; Available online: https://www.nrlquality.org.au/who-covid-evaluations-summary-of-results (accessed on 20 November 2022).
- U.S. Food and Drug Administration. Independent Evaluations of COVID-19 Serological Tests. Available online: https://open.fda.gov/apis/device/covid19serology/ (accessed on 20 November 2022).
- Van den Beld, M.J.C.; Murk, J.-L.; Kluytmans, J.; Koopmans, M.P.G.; Reimerink, J.; van Loo, I.H.M.; Wegdam-Blans, M.C.A.; Zaaijer, H.; Serology Workgroup for SARS-CoV-2; GeurtsvanKessel, C.; et al. Increasing the Efficiency of a National Laboratory Response to COVID-19: A Nationwide Multicenter Evaluation of 47 Commercial SARS-CoV-2 Immunoassays by 41 Laboratories. J. Clin. Microbiol. 2021, 59, e0076721. [Google Scholar] [CrossRef] [PubMed]
- Australian Government Department of Health Therapeutic Goods Administration. Post-Market Evaluation of Serology-Based Point of Care Tests. Available online: https://www.tga.gov.au/post-market-evaluation-serology-based-point-care-tests (accessed on 20 November 2022).
- FIND Diagnostics for All. SARS-CoV-2 Test Performance; FIND Diagnostics: Geneva, Switzerland, 2020; Available online: https://www.finddx.org/covid-19/ab-test-perf/ (accessed on 20 November 2022).
- UK Health Security Agency. Validating COVID-19 Tests in the Private Market; UK Health Security Agency: London, UK, 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1053516/Validating_COVID_19_tests_in_the_private_market.pdf (accessed on 20 November 2022).
- Peluso, M.J.; Takahashi, S.; Hakim, J.; Kelly, J.D.; Torres, L.; Iyer, N.S.; Turcios, K.; Janson, O.; Munter, S.E.; Thanh, C.; et al. SARS-CoV-2 Antibody Magnitude and Detectability Are Driven by Disease Severity, Timing, and Assay. Sci. Adv. 2021, 7, eabh3409. [Google Scholar] [CrossRef]
- Einhauser, S.; Peterhoff, D.; Niller, H.H.; Beileke, S.; Günther, F.; Steininger, P.; Burkhardt, R.; Heid, I.M.; Pfahlberg, A.B.; Überla, K.; et al. Spectrum Bias and Individual Strengths of SARS-CoV-2 Serological Tests—A Population-Based Evaluation. Diagnostics 2021, 11, 1843. [Google Scholar] [CrossRef]
- Bobrovitz, N.; Arora, R.K.; Boucher, E.; Yan, T.; Rahim, H.; Van Wyk, J.; Duarte, N.; Atmaja, A.; Rocco, S.; Joseph, a.; et al. A Systematic Review and Meta-Analysis of SARS-CoV-2 Seroprevalence Studies Aligned with the WHO Population-Based Sero-Epidemiological ‘Unity’ Protocol; PROSPERO International Prospective Register of Systematic Reviews: York, UK, 2021; Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=183634 (accessed on 20 November 2022).
- Arora, R.K.; Joseph, A.; Van Wyk, J.; Rocco, S.; Atmaja, A.; May, E.; Yan, T.; Bobrovitz, N.; Chevrier, J.; Cheng, M.P.; et al. SeroTracker: A Global SARS-CoV-2 Seroprevalence Dashboard. Lancet Infect. Dis. 2021, 21, e75–e76. [Google Scholar] [CrossRef]
- Bobrovitz, N.; Arora, R.K.; Cao, C.; Boucher, E.; Liu, M.; Donnici, C.; Yanes-Lane, M.; Whelan, M.; Perlman-Arrow, S.; Chen, J.; et al. Global Seroprevalence of SARS-CoV-2 Antibodies: A Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0252617. [Google Scholar] [CrossRef]
- Bergeri, I.; Whelan, M.; Ware, H.; Subissi, L.; Nardone, A.; Lewis, H.C.; Li, Z.; Ma, X.; Valenciano, M.; Cheng, B.; et al. Global Epidemiology of SARS-CoV-2 Infection: A Systematic Review and Meta-Analysis of Standardized Population-Based Seroprevalence Studies, Jan 2020-Dec 2021. medRxiv 2022. [Google Scholar] [CrossRef]
- Bobrovitz, N.; Noel, K.C.; Li, Z.; Cao, C.; Deveaux, G.; Selemon, A.; Clifton, D.A.; Yanes Lane, M.; Yan, T.; Arora, R.K. SeroTracker-RoB: An Approach to Automating Reproducible Risk of Bias Assessment of Seroprevalence Studies. Epidemiology 2021. preprint. [Google Scholar] [CrossRef]
- The Joanna Briggs Institute. Critical Appraisal Tools for Use in JBI Systematic Reviews Checklist for Prevalence Studies; The Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- World Health Organization. Target Product Profiles for Priority Diagnostics to Support Response to the COVID-19 Pandemic v.1.0; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2013. [Google Scholar]
- Sempos, C.T.; Tian, L. Adjusting Coronavirus Prevalence Estimates for Laboratory Test Kit Error. Am. J. Epidemiol. 2021, 190, 109–115. [Google Scholar] [CrossRef]
- Pourhoseingholi, M.A.; Vahedi, M.; Rahimzadeh, M. Sample Size Calculation in Medical Studies. Gastroenterol. Hepatol. Bed Bench 2013, 6, 14–17. [Google Scholar]
- Caini, S.; Bellerba, F.; Corso, F.; Díaz-Basabe, A.; Natoli, G.; Paget, J.; Facciotti, F.; De Angelis, S.P.; Raimondi, S.; Palli, D.; et al. Meta-Analysis of Diagnostic Performance of Serological Tests for SARS-CoV-2 Antibodies up to 25 April 2020 and Public Health Implications. Euro Surveill. Bull. Eur. Sur Mal. Transm. Eur. Commun. Dis. Bull. 2020, 25, 2000980. [Google Scholar] [CrossRef]
- Lisboa Bastos, M.; Tavaziva, G.; Abidi, S.K.; Campbell, J.R.; Haraoui, L.-P.; Johnston, J.C.; Lan, Z.; Law, S.; MacLean, E.; Trajman, A.; et al. Diagnostic Accuracy of Serological Tests for Covid-19: Systematic Review and Meta-Analysis. BMJ 2020, 370, m2516. [Google Scholar] [CrossRef]
- Whitman, J.D.; Hiatt, J.; Mowery, C.T.; Shy, B.R.; Yu, R.; Yamamoto, T.N.; Rathore, U.; Goldgof, G.M.; Whitty, C.; Woo, J.M.; et al. Evaluation of SARS-CoV-2 Serology Assays Reveals a Range of Test Performance. Nat. Biotechnol. 2020, 38, 1174–1183. [Google Scholar] [CrossRef]
- Vengesai, A.; Midzi, H.; Kasambala, M.; Mutandadzi, H.; Mduluza-Jokonya, T.L.; Rusakaniko, S.; Mutapi, F.; Naicker, T.; Mduluza, T. A Systematic and Meta-Analysis Review on the Diagnostic Accuracy of Antibodies in the Serological Diagnosis of COVID-19. Syst. Rev. 2021, 10, 155. [Google Scholar] [CrossRef]
- Theel, E.S. Performance Characteristics of High-Throughput Serologic Assays for Severe Acute Respiratory Syndrome Coronavirus 2 with Food and Drug Administration Emergency Use Authorization: A Review. Clin. Lab. Med. 2022, 42, 15–29. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration. EUA Authorized Serology Test Performance. Available online: https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergency-use-authorizations-medical-devices/eua-authorized-serology-test-performance (accessed on 20 November 2022).
- Stein, D.R.; Osiowy, C.; Gretchen, A.; Thorlacius, L.; Fudge, D.; Lang, A.; Sekirov, I.; Morshed, M.; Levett, P.N.; Tran, V.; et al. Evaluation of Commercial SARS-CoV-2 Serological Assays in Canadian Public Health Laboratories. Diagn. Microbiol. Infect. Dis. 2021, 101, 115412. [Google Scholar] [CrossRef]
- Takahashi, S.; Greenhouse, B.; Rodríguez-Barraquer, I. Are Seroprevalence Estimates for Severe Acute Respiratory Syndrome Coronavirus 2 Biased? J. Infect. Dis. 2020, 222, 1772–1775. [Google Scholar] [CrossRef]
- Lippi, G.; Adeli, K.; Plebani, M. Commercial Immunoassays for Detection of Anti-SARS-CoV-2 Spike and RBD Antibodies: Urgent Call for Validation against New and Highly Mutated Variants. Clin. Chem. Lab. Med. 2021, 60, 338–342. [Google Scholar] [CrossRef]
- Tso, F.Y.; Lidenge, S.J.; Peña, P.B.; Clegg, A.A.; Ngowi, J.R.; Mwaiselage, J.; Ngalamika, O.; Julius, P.; West, J.T.; Wood, C. High Prevalence of Pre-Existing Serological Cross-Reactivity against Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) in Sub-Saharan Africa. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2021, 102, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Emmerich, P.; Murawski, C.; Ehmen, C.; von Possel, R.; Pekarek, N.; Oestereich, L.; Duraffour, S.; Pahlmann, M.; Struck, N.; Eibach, D.; et al. Limited Specificity of Commercially Available SARS-CoV-2 IgG ELISAs in Serum Samples of African Origin. Trop. Med. Int. Health TMIH 2021, 26, 621–631. [Google Scholar] [CrossRef] [PubMed]
- Bottomley, C.; Otiende, M.; Uyoga, S.; Gallagher, K.; Kagucia, E.W.; Etyang, A.O.; Mugo, D.; Gitonga, J.; Karanja, H.; Nyagwange, J.; et al. Quantifying Previous SARS-CoV-2 Infection through Mixture Modelling of Antibody Levels. Nat. Commun. 2021, 12, 6196. [Google Scholar] [CrossRef] [PubMed]
- Irwin, N.; Murray, L.; Ozynski, B.; Richards, G.A.; Paget, G.; Venturas, J.; Kalla, I.; Diana, N.; Mahomed, A.; Zamparini, J. Age Significantly Influences the Sensitivity of SARS-CoV-2 Rapid Antibody Assays. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2021, 109, 304–309. [Google Scholar] [CrossRef]
- Vogel, G.; Couzin-Frankel, J. Grade: Incomplete. Science 2020, 370, 1023–1027. [Google Scholar] [CrossRef]
- Mead, R. Statistical Games 2—Medical Diagnosis. Teach. Stat. 1992, 14, 12–16. [Google Scholar] [CrossRef]
- Veyrenche, N.; Bolloré, K.; Pisoni, A.; Bedin, A.; Mondain, A.; Ducos, J.; Segondy, M.; Montes, B.; Pastor, P.; Morquin, D.; et al. Diagnosis Value of SARS-CoV-2 Antigen/Antibody Combined Testing Using Rapid Diagnostic Tests at Hospital Admission. J. Med. Virol. 2021, 93, 3069–3076. [Google Scholar] [CrossRef]
- Luijkx, T.; Morgan, M. Sensitivity and Specificity of Multiple Tests. In Radiopaedia.org. 2015. Available online: https://radiopaedia.org/articles/sensitivity-and-specificity-of-multiple-tests?lang=us (accessed on 20 November 2022). [CrossRef]
- Weinstein, S.; Obuchowski, N.A.; Lieber, M.L. Clinical Evaluation of Diagnostic Tests. Am. J. Roentgenol. 2005, 184, 14–19. [Google Scholar] [CrossRef]
- Comparative Evaluation of Lateral Flow Assay (LFA) and ELISA Tests That Detect Human Antibodies Specific to SARS-CoV-2 to Suppor. FIND Diagnostics. (Version 27 APR 2020). Available online: https://www.finddx.org/wp-content/uploads/2020/04/20200427-COVID-19-IA-Evaluation-Synopsis.pdf (accessed on 22 March 2022).
- Overview of FIND Methodology for Antibody Evaluations Introduction: Overview of the Studies. FIND Diagnostics. Last Updated on 26 April. Available online: https://www.finddx.org/wp-content/uploads/2021/04/Overview-of-FIND-Methodology-for-Antibody-Evaluations-2021April29.pdf (accessed on 22 March 2022).
- Post-Market Validation of Serological Point-of-Care Tests for COVID-19. Australian Government Department of Health. Available online: https://www.health.gov.au/resources/collections/post-market-validation-of-serological-point-of-care-tests-for-covid-19 (accessed on 22 March 2022).
- SARS-CoV-2 Antibody Detection Test Kit Performance Evaluation Protocol. Available online: https://www.nrlquality.org.au/_files/ugd/188553_d050808aa3374506968498af59ed5ebc.pdf (accessed on 22 March 2022).




{kind=link}
{kind=link}
{kind=link}
| Assay Characteristics | Commercially Assays | Self-Developed Assays | ||
|---|---|---|---|---|
| (N = 192) | (N = 380) | |||
| n | % | n | % | |
| Developed by | ||||
| Manufacturer | 162 | - | ||
| Lab groups | - | 275 | ||
| Type of Assays | ||||
| ELISA | 60 | 31.3 | 261 | 68.7 |
| LFIA | 75 | 39.1 | 0 | 0.0 |
| IFA | 5 | 2.6 | 17 | 4.5 |
| CLIA (Including CGIA, CMIA) | 30 | 15.6 | 3 | 0.8 |
| Neutralization Assay | 0 | 0.0 | 52 | 13.7 |
| Others/Not specified | 22 | 11.5 | 47 | 12.4 |
| WHO regions of development | ||||
| Africa | 0 | 0.0 | 12 | 3.2 |
| America | 49 | 25.5 | 152 | 40.0 |
| Eastern Mediterranean | 5 | 2.6 | 15 | 3.9 |
| Europe | 75 | 39.1 | 163 | 42.9 |
| South East Asia | 4 | 2.1 | 6 | 1.6 |
| Western Pacific | 58 | 30.2 | 32 | 8.4 |
| Not Reported | 1 | 0.5 | 0 | 0.0 |
| Feature of Assays | ||||
| RDT | 103 | 53.6 | 17 | 4.5 |
| Non-RDT | 89 | 46.4 | 363 | 95.5 |
| Antibody Targets | ||||
| Spike | 55 | 28.6 | 48 | 12.6 |
| Nucleocapsid | 37 | 19.3 | 37 | 9.7 |
| Multiplex Targetsa | 38 | 19.8 | 171 | 45.0 |
| Unknown | 62 | 32.3 | 124 | 32.6 |
| Isotypes | ||||
| IgG-only | 52 | 27.1 | 149 | 39.2 |
| IgG and IgM | 103 | 53.6 | 31 | 8.2 |
| Total Antibody (IgG, IgM, IgA) | 22 | 11.5 | 38 | 10.0 |
| Other Combinationsb/ Not Reported | 15 | 7.8 | 162 | 42.6 |
| Assay Sn. and Sp. | ||||
| Manufacturer/developer reported | 91 | 47.4 | 124 | 32.6 |
| Third-party validated | 118 | 61.5 | - | - |
| Australia NRL | 16 | 8.3 | - | - |
| Australia Doherty | 18 | 9.4 | - | - |
| US FDA | 57 | 29.7 | - | - |
| FIND Diagnostic | 30 | 15.6 | - | - |
| Netherland CIDC | 26 | 13.5 | - | - |
| Other groups | 94 | 49.0 | - | - |
| Emergency Use c | ||||
| Yes | 57 | 29.7 | - | - |
| No | 135 | 70.3 | - | - |
| Fixed Effects | Sensitivity | Specificity | ||||||
|---|---|---|---|---|---|---|---|---|
| Difference in Performance against Manufacturer Value a | Absolute Performance Value b | pc | Difference in Performance against Manufacturer Value b | Absolute Performance Value a | p c | |||
| [95% CI] | [95% CI] | [95% CI] | [95% CI] | |||||
| Source of Evaluation | ||||||||
| Manufacturer | ref. | 93.6% | <0.001 | * | ref. | 98.5% | <0.001 | * |
| [90.6, 95.7%] | [97.8, 99.0%] | |||||||
| Independent | 3.3% | 90.3% | 0.001 | * | 0.2% | 98.3% | 0.247 | |
| [2.7, 3.4%] | [87.8, 92.3%] | [−0.1, 0.4%] | [97.8, 98.7%] | |||||
| Third Party’s Lab | 1.0% | 92.6% | 0.289 | 0.9% | 97.6% | <0.001 | * | |
| [0.1, 1.4%] | [90.5, 94.3%] | [0.9, 0.9%] | [96.9, 98.2%] | |||||
| NRL | −2.2% | 95.8% | 0.207 | * | 4.2% | 94.4% | <0.001 | * |
| [−2.3, −1.8%] | [92.9, 97.5%] | [2.7, 6.4%] | [91.3, 96.4%] | |||||
| US FDA | −2.2% | 95.8% | 0.038 | * | 0.4% | 98.1% | 0.047 | * |
| [−3.6, −1.3%] | [94.2, 97.0%] | [0.4, 0.4%] | [97.3, 98.6%] | |||||
| FIND Diagnostic | 18.6% | 75.0% | <0.001 | * | 0.9% | 97.6% | 0.008 | * |
| [14.6, 22.8%] | [67.8, 81.1%] | [0.6, 1.3%] | [96.4, 98.4%] | |||||
| Netherland CIDC | −0.2% | 93.8% | 0.825 | 0.5% | 98.0% | 0.060 | ||
| [−0.3, 0.0%] | [90.5, 96.0%] | [0.4, 0.7%] | [97.0, 98.7%] | |||||
| Doherty | 2.7% | 90.9% | 0.055 | 0.8% | 97.7% | 0.037 | * | |
| [1.5, 4.5%] | [86.1, 94.1%] | [0.4, 1.5%] | [96.2, 98.6%] | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, X.; Li, Z.; Whelan, M.G.; Kim, D.; Cao, C.; Yanes-Lane, M.; Yan, T.; Jaenisch, T.; Chu, M.; Clifton, D.A.; et al. Serology Assays Used in SARS-CoV-2 Seroprevalence Surveys Worldwide: A Systematic Review and Meta-Analysis of Assay Features, Testing Algorithms, and Performance. Vaccines 2022, 10, 2000. https://doi.org/10.3390/vaccines10122000
Ma X, Li Z, Whelan MG, Kim D, Cao C, Yanes-Lane M, Yan T, Jaenisch T, Chu M, Clifton DA, et al. Serology Assays Used in SARS-CoV-2 Seroprevalence Surveys Worldwide: A Systematic Review and Meta-Analysis of Assay Features, Testing Algorithms, and Performance. Vaccines. 2022; 10(12):2000. https://doi.org/10.3390/vaccines10122000
Chicago/Turabian StyleMa, Xiaomeng, Zihan Li, Mairead G. Whelan, Dayoung Kim, Christian Cao, Mercedes Yanes-Lane, Tingting Yan, Thomas Jaenisch, May Chu, David A. Clifton, and et al. 2022. "Serology Assays Used in SARS-CoV-2 Seroprevalence Surveys Worldwide: A Systematic Review and Meta-Analysis of Assay Features, Testing Algorithms, and Performance" Vaccines 10, no. 12: 2000. https://doi.org/10.3390/vaccines10122000