
Acceptance of a Third Dose of COVID-19 Vaccine and Associated Factors in China Based on Health Belief Model: A National Cross-Sectional Study



Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Acceptance of a Third Dose of COVID-19 Vaccine
2.4. Health Beliefs on COVID-19 and COVID-19 Vaccine
2.5. Data Analysis
3. Results
3.1. Characteristics of the Participants
3.2. Acceptance of a Third Dose of COVID-19 Vaccine
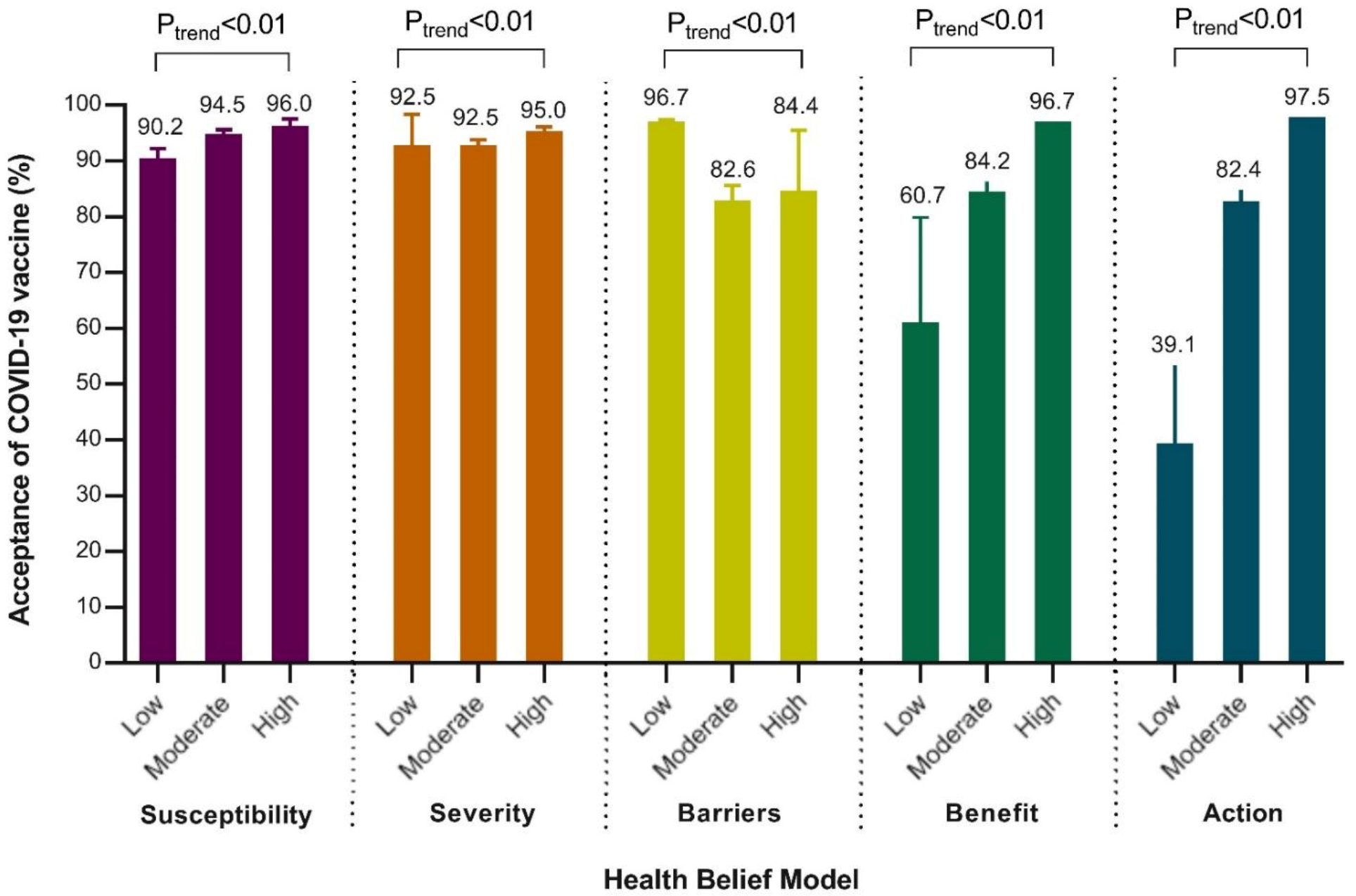
3.3. Comparison of the Acceptance of a Third Dose of COVID-19 Vaccine by Dimensions of Health Belief Model
3.4. Factors Related with a Third Dose of COVID-19 Vaccine Acceptance
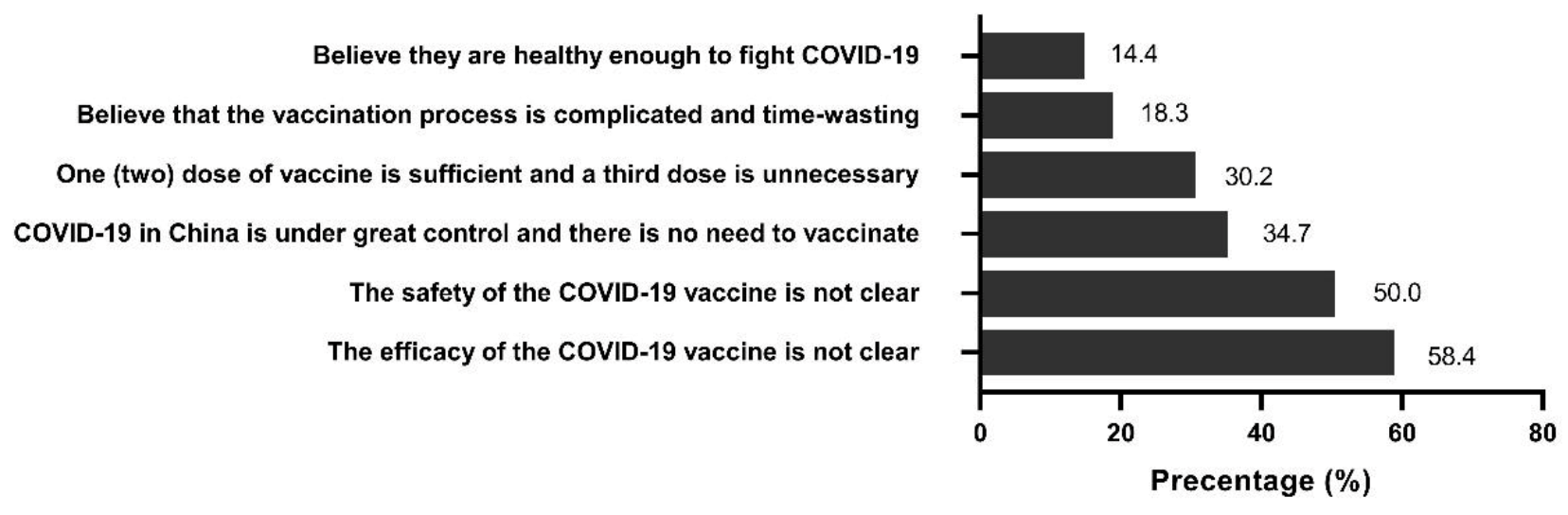
3.5. Reasons for Hesitation to Receive a Third Dose of COVID-19 Vaccine
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jin, Y.; Yang, H.; Ji, W.; Wu, W.; Chen, S.; Zhang, W.; Duan, G. Virology, Epidemiology, Pathogenesis, and Control of COVID-19. Viruses 2020, 12, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johns Hopkins University. COVID-19 Map. Available online: https://coronavirus.jhu.edu/map.html (accessed on 24 November 2021).
- London School of Hygiene & Tropical Medicine. COVID-19 Vaccine Tracker. Available online: https://vac-lshtm.shinyapps.io/ncov_vaccine_landscape/ (accessed on 24 December 2021).
- National Health Commission of People’s Republic of China. COVID-19 Vaccination Status. Available online: http://www.nhc.gov.cn/jkj/s7915/202112/690b96ef633640bbb0b090832eb27eda.shtml (accessed on 25 December 2021).
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Tang, P.; Hasan, M.R.; Coyle, P.; Al Kanaani, Z.; et al. Association of Prior SARS-CoV-2 Infection With Risk of Breakthrough Infection Following mRNA Vaccination in Qatar. JAMA J. Am. Med. Assoc. 2021, 326, 1930–1939. [Google Scholar] [CrossRef] [PubMed]
- Del Rio, C.; Malani, P.N.; Omer, S.B. Confronting the Delta Variant of SARS-CoV-2, Summer 2021. JAMA J. Am. Med. Assoc. 2021, 326, 1001–1002. [Google Scholar] [CrossRef] [PubMed]
- Mallapaty, S. China’s COVID vaccines have been crucial—Now immunity is waning. Nature 2021, 598, 398–399. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Cohen, C.; Hernán, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]
- WHO. Interim Statement On Booster Doses for COVID-19 Vaccination. Available online: https://www.who.int/news/item/04-10-2021-interim-statement-on-booster-doses-for-covid-19-vaccination (accessed on 24 November 2021).
- Our World in Data. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 25 December 2021).
- Salmon, D.A.; Dudley, M.Z.; Glanz, J.M.; Omer, S.B. Vaccine hesitancy: Causes, consequences, and a call to action. Vaccine 2015, 33 (Suppl. S4), D66–D71. [Google Scholar] [CrossRef]
- McAteer, J.; Yildirim, I.; Chahroudi, A. The VACCINES Act: Deciphering Vaccine Hesitancy in the Time of COVID-19. Clin. Infect. Dis. 2020, 71, 703–705. [Google Scholar] [CrossRef]
- Pal, S.; Shekhar, R.; Kottewar, S.; Upadhyay, S.; Singh, M.; Pathak, D.; Kapuria, D.; Barrett, E.; Sheikh, A.B. COVID-19 Vaccine Hesitancy and Attitude toward Booster Doses among US Healthcare Workers. Vaccines 2021, 9, 1358. [Google Scholar] [CrossRef]
- Klugar, M.; Riad, A.; Mohanan, L.; Pokorná, A. COVID-19 Vaccine Booster Hesitancy (VBH) of Healthcare Workers in Czechia: National Cross-Sectional Study. Vaccines 2021, 9, 1437. [Google Scholar] [CrossRef]
- Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef]
- Sugawara, N.; Yasui-Furukori, N.; Fukushima, A.; Shimoda, K. Attitudes of Medical Students toward COVID-19 Vaccination: Who Is Willing to Receive a Third Dose of the Vaccine? Vaccines 2021, 9, 1295. [Google Scholar] [CrossRef]
- Wang, R.; Tao, L.; Han, N.; Liu, J.; Yuan, C.; Deng, L.; Han, C.; Sun, F.; Chi, L.; Liu, M.; et al. Acceptance of seasonal influenza vaccination and associated factors among pregnant women in the context of COVID-19 pandemic in China: A multi-center cross-sectional study based on health belief model. BMC Pregnancy Childbirth 2021, 21, 745. [Google Scholar] [CrossRef]
- Tao, L.; Wang, R.; Han, N.; Liu, J.; Yuan, C.; Deng, L.; Han, C.; Sun, F.; Liu, M.; Liu, J. Acceptance of a COVID-19 vaccine and associated factors among pregnant women in China: A multi-center cross-sectional study based on health belief model. Hum. Vaccin Immunother. 2021, 17, 2378–2388. [Google Scholar] [CrossRef]
- Tao, L.; Wang, R.; Liu, J. Comparison of Vaccine Acceptance Between COVID-19 and Seasonal Influenza Among Women in China: A National Online Survey Based on Health Belief Model. Front. Med. 2021, 8, 679520. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social learning theory and the Health Belief Model. Health Educ. Q. 1988, 15, 175–183. [Google Scholar] [CrossRef]
- Baccolini, V.; Renzi, E.; Isonne, C.; Migliara, G.; Massimi, A.; De Vito, C.; Marzuillo, C.; Villari, P. COVID-19 Vaccine Hesitancy among Italian University Students: A Cross-Sectional Survey during the First Months of the Vaccination Campaign. Vaccines 2021, 9, 1292. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Abedin, M.; Islam, M.A.; Rahman, F.N.; Reza, H.M.; Hossain, M.Z.; Hossain, M.A.; Arefin, A.; Hossain, A. Willingness to vaccinate against COVID-19 among Bangladeshi adults: Understanding the strategies to optimize vaccination coverage. PLoS ONE 2021, 16, e0250495. [Google Scholar] [CrossRef]
- Liu, Q.; Qin, C.; Liu, M.; Liu, J. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: A systematic review and meta-analysis. Infect. Dis. Poverty 2021, 10, 132. [Google Scholar] [CrossRef]
- Wu, Q.; Dudley, M.Z.; Chen, X.; Bai, X.; Dong, K.; Zhuang, T.; Salmon, D.; Yu, H. Evaluation of the safety profile of COVID-19 vaccines: A rapid review. BMC Med. 2021, 19, 173. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef]
- Moghnieh, R.; Mekdashi, R.; El-Hassan, S.; Abdallah, D.; Jisr, T.; Bader, M.; Jizi, I.; Sayegh, M.H.; Rahman Bizri, A. Immunogenicity and reactogenicity of BNT162b2 booster in BBIBP-CorV-vaccinated individuals compared with homologous BNT162b2 vaccination: Results of a pilot prospective cohort study from Lebanon. Vaccine 2021, 39, 6713–6719. [Google Scholar] [CrossRef]
- Cao, Y.; Yisimayi, A.; Bai, Y.; Huang, W.; Li, X.; Zhang, Z.; Yuan, T.; An, R.; Wang, J.; Xiao, T.; et al. Humoral immune response to circulating SARS-CoV-2 variants elicited by inactivated and RBD-subunit vaccines. Cell Res. 2021, 31, 732–741. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Number (%) | Acceptance of a Third Dose of COVID-19 Vaccination | p Value | |
|---|---|---|---|---|
| Yes (%) | 95% CI | |||
| Sociodemographic characteristics | ||||
| Region | 0.06 | |||
| Eastern | 1357 (43.5) | 1256 (92.6) | 91.1–93.9 | |
| Central | 962 (30.8) | 911 (94.7) | 93.1–96.0 | |
| Western | 800 (25.6) | 756 (94.5) | 92.8–95.9 | |
| Age group(years) | <0.01 * | |||
| ≤20 | 162 (5.2) | 150 (92.6) | 87.8–95.9 | |
| 21–30 | 1747 (56.0) | 1652 (94.6) | 93.4–95.6 | |
| 31–40 | 934 (29.9) | 877 (93.9) | 92.2–95.3 | |
| 41–50 | 194 (6.2) | 177 (91.2) | 86.6–94.6 | |
| >50 | 82 (2.6) | 67 (81.7) | 72.3–88.9 | |
| Sex | 0.08 | |||
| Female | 1608 (51.6) | 1519 (94.5) | 93.3–95.5 | |
| Male | 1511 (48.4) | 1404 (92.9) | 91.5–94.1 | |
| Education§ | <0.01 * | |||
| High school or polytechnic school | 184 (5.9) | 162 (88.0) | 82.8–92.1 | |
| Junior college | 413 (13.2) | 373 (90.3) | 87.2–92.9 | |
| Bachelor’s degree | 2357 (75.6) | 2238 (95.0) | 94.0–95.8 | |
| Postgraduate degree | 165 (5.3) | 150 (90.9) | 85.8–94.6 | |
| Occupation | <0.01 * | |||
| Civil servant | 77 (2.5) | 75 (97.4) | 91.9–99.5 | |
| Employees of enterprise | 1986 (63.7) | 1866 (94.0) | 92.8–94.9 | |
| Employees of public Institutions | 367 (11.8) | 359 (97.8) | 95.9–99.0 | |
| Individual household | 238 (7.6) | 208 (87.4) | 82.7–91.2 | |
| Student | 384 (12.3) | 361 (94.0) | 91.3–96.1 | |
| Others | 67 (2.1) | 54 (80.6) | 70.0–88.7 | |
| Monthly household income per capita(RMB) | 0.01 * | |||
| ≤3000 | 411 (13.2) | 385 (93.7) | 91.0–95.7 | |
| 3001–5000 | 558 (17.9) | 506 (90.7) | 88.1–92.9 | |
| 5001–10,000 | 1370 (43.9) | 1285 (93.8) | 92.4–95.0 | |
| 10,001–20,000 | 641 (20.6) | 613 (95.6) | 93.8–97.0 | |
| >20,000 | 139 (4.5) | 134 (96.4) | 92.3–98.6 | |
| Health status | ||||
| History of chronic disease | 0.05 | |||
| Yes | 238 (7.6) | 216 (90.8) | 86.6–93.9 | |
| No | 2881 (92.4) | 2707 (94.0) | 93.0–94.8 | |
| History of COVID-19 vaccination | <0.01 * | |||
| Sinopharm BIBP | 1137 (36.5) | 1085 (95.4) | 94.1–96.5 | |
| Sinovac | 1770 (56.7) | 1668 (94.2) | 93.1–95.3 | |
| Convidecia | 118 (3.8) | 110 (93.2) | 87.6–96.7 | |
| No | 94 (3.0) | 60 (63.8) | 53.8–73.0 | |
| Knowledge factors | ||||
| Total knowledge score on COVID-19 | <0.01 * | |||
| Low (score 0–4) | 26 (0.03) | 19 (73.1) | 54.3–87.1 | |
| Moderate (score 5–10) | 1495 (47.9) | 1380 (92.3) | 90.9–93.6 | |
| High (score 11–15) | 1598 (51.2) | 1524 (95.4) | 94.3–96.3 | |
| Total knowledge score on COVID-19 vaccination | 0.01 * | |||
| Low (score 0) | 22 (0.71) | 18 (81.8) | 62.4–93.5 | |
| Moderate (score 1–2) | 1793 (57.5) | 1665 (92.9) | 91.6–94.0 | |
| High (score 3) | 1304 (41.8) | 1240 (95.1) | 93.8–96.2 | |
| Total | 3119 (100) | 2923 (93.7) | 92.9–94.6 | |
| Dimensions of Health Belief Model | Item | Response | Number (%) | Acceptance of a Third Dose of COVID-19 Vaccine | p Value | |
|---|---|---|---|---|---|---|
| Yes (%) | 95% CI | |||||
| Perceived susceptibility | Are you concerned about getting COVID-19 | Not concerned | 814 (26.1) | 734 (90.2) | 88.0–92.1 | <0.05 * |
| Concerned | 2305 (73.9) | 2189 (95.0) | 94.0–95.8 | |||
| Are you worried about your family contracting the COVID-19 | Not concerned | 547 (17.5) | 488 (89.2) | 86.4–91.6 | <0.05 * | |
| Concerned | 2572 (82.5) | 2435 (94.7) | 93.8–95.5 | |||
| Perceived severity | People who get COVID-19 are more likely to get severe illness | Disagree | 1548 (49.6) | 1438 (92.9) | 91.5–94.1 | 0.06 |
| Agree | 1571 (50.4) | 1485 (94.5) | 93.3–95.6 | |||
| When you get COVID-19, your family’s health may be at risk | Disagree | 192 (6.2) | 164 (85.4) | 79.9–89.9 | <0.05 * | |
| Agree | 2927 (93.8) | 2759 (94.3) | 93.4–95.1 | |||
| Perceived barriers | A third dose of COVID-19 vaccine can cause infection | Disagree | 2903 (93.1) | 2726 (93.9) | 93.0–94.7 | 0.115 |
| Agree | 216 (6.9) | 197 (91.2) | 86.9–94.4 | |||
| It is not safe to get a third dose against COVID-19 | Disagree | 3079 (98.7) | 2891 (93.9) | 93.0–94.7 | <0.05 * | |
| Agree | 40 (1.3) | 32 (80.0) | 65.8–90.1 | |||
| It is not effective to get a third dose against COVID-19 | Disagree | 2976 (95.4) | 2811 (94.5) | 93.6–95.2 | <0.05 * | |
| Agree | 143 (4.6) | 112 (8.3) | 71.0–84.5 | |||
| Perceived benefits | It is good to strengthen your health with COVID-19 vaccination | Disagree | 794 (25.5) | 678 (85.4) | 82.8–87.7 | <0.05 * |
| Agree | 2325 (74.5) | 2245 (96.6) | 95.8–97.2 | |||
| It is good for family health when vaccinating a third dose | Disagree | 801 (25.7) | 685 (85.5) | 83.0–87.8 | <0.05 * | |
| Agree | 2318 (74.3) | 2238 (96.5) | 95.7–97.2 | |||
| A third dose can provide better protection against COVID-19 | Disagree | 479 (15.4) | 400 (83.5) | 80.0–86.6 | <0.05 * | |
| Agree | 2640 (84.6) | 2523 (95.6) | 94.7–96.3 | |||
| Cues to action | If your doctor/nurse recommends that you get a third dose against COVID-19, you will choose it | Disagree | 509 (16.3) | 404 (79.4) | 75.7–82.7 | <0.05 * |
| Agree | 2610 (83.7) | 2519 (96.5) | 95.8–97.2 | |||
| If your family recommends you to get a third dose, you will take it | Disagree | 709 (22.7) | 600 (84.6) | 81.8–87.1 | <0.05 * | |
| Agree | 2410 (77.3) | 2323 (96.40) | 95.6–97.1 | |||
| If the community recommends that you get a third dose against COVID-19, you will choose it | Disagree | 930 (29.8) | 782 (84.10) | 81.6–86.3 | <0.05 * | |
| Agree | 2189 (70.2) | 2141 (97.80) | 97.1–98.4 | |||
| Characteristics | Univariable Model | Multivariable Model | ||
|---|---|---|---|---|
| Crude OR (95% CI) | p Value | Adjusted OR (95% CI) | p Value | |
| Sociodemographic characteristics | ||||
| Age group(years) | ||||
| ≤20 | 1 (reference) | 1 (reference) | ||
| 21–30 | 1.39 (0.75–2.60) | 0.30 | 1.22 (0.50–2.98) | 0.67 |
| 31–40 | 1.23 (0.65–2.35) | 0.53 | 1.19 (0.45–3.19) | 0.73 |
| 41–50 | 0.83 (0.39–1.80) | 0.64 | 1.15 (0.37–3.58) | 0.81 |
| >50 | 0.36 (0.16–0.81) | 0.01 * | 0.39 (0.12–1.33) | 0.13 |
| Education§ | ||||
| High school or polytechnic school | 1 (reference) | 1 (reference) | ||
| Junior college | 1.27 (0.73–2.20) | 0.40 | 0.88 (0.42–1.81) | 0.72 |
| Bachelor’s degree | 2.55 (1.58–4.14) | <0.01 * | 1.20 (0.60–2.39) | 0.61 |
| Postgraduate degree | 1.36 (0.68–2.72) | 0.38 | 0.61 (0.23–1.65) | 0.33 |
| Occupation | ||||
| Civil servant | 1 (reference) | 1 (reference) | ||
| Employees of enterprise | 0.42 (0.10–1.71) | 0.22 | 0.21 (0.046–0.98) | 0.05 * |
| Employees of public Institutions | 1.20 (0.25–5.745) | 0.82 | 0.84 (0.15–4.59) | 0.84 |
| Individual household | 0.19 (0.04–0.79) | 0.02 * | 0.11 (0.02–0.53) | 0.01 * |
| Student | 0.42 (0.10–1.81) | 0.24 | 0.18 (0.03–1.01) | 0.05 |
| Others | 0.11 (0.02–0.51) | 0.01 * | 0.10 (0.02–0.57) | 0.01 * |
| Monthly household income per capita (RMB) | ||||
| ≤3000 | 1 (reference) | 1 (reference) | ||
| 3001–5000 | 0.66 (0.40–1.07) | 0.09 | 0.69 (0.31–1.54) | 0.37 |
| 5001–10,000 | 1.02 (0.65–1.61) | 0.93 | 0.72 (0.32–1.65) | 0.44 |
| 10,001–20,000 | 1.48 (0.85–2.56) | 0.16 | 1.25 (0.50–3.13) | 0.64 |
| >20,000 | 1.81 (0.68–4.81) | 0.23 | 2.13 (0.55–8.28) | 0.27 |
| History of COVID-19 vaccination | ||||
| Sinopharm BBIP | 11.82 (7.14–19.58) | <0.01 * | 6.55 (3.30–12.98) | <0.01 * |
| Sinovac | 9.27 (5.82–14.77) | <0.01 * | 5.22 (2.72–10.02) | <0.01 * |
| Convidecia | 7.79 (3.39–17.90) | <0.01 * | 5.80 (2.04–16.48) | <0.01 * |
| No | 1 (reference) | 1 (reference) | ||
| Knowledge factors | ||||
| Total knowledge score on COVID-19 | ||||
| Low (score 0–4) | 1 (reference) | 1 (reference) | ||
| Moderate (score 5–10) | 4.42 (1.82–10.74) | <0.01 * | 0.60 (0.17–2.12) | 0.42 |
| High (score 11–15) | 7.59 (3.09–18.61) | <0.01 * | 0.89 (0.24–3.21) | 0.85 |
| Total knowledge score on COVID-19 vaccination | ||||
| Low (score 0) | 1 (reference) | 1 (reference) | ||
| Moderate (score 1–2) | 2.89 (0.96–8.67) | 0.06 | 0.41 (0.10–1.76) | 0.23 |
| High (score 3) | 4.31 (1.42–13.09) | 0.01 * | 0.49 (0.11–2.12) | 0.34 |
| Health belief factors | ||||
| Perceived susceptibility | ||||
| Low | 1 (reference) | 1 (reference) | ||
| Moderate | 1.89 (1.38–2.59) | <0.01 * | 2.41 (1.62–3.58) | <0.01 * |
| High | 2.60 (1.63–4.13) | <0.01 * | 2.48 (1.42–4.31) | <0.01 * |
| Perceived severity | ||||
| Low | 1 (reference) | 1 (reference) | ||
| Moderate | 1.00 (0.43–2.35) | 1.00 | 0.45 (0.14–1.46) | 0.18 |
| High | 1.54 (0.65–3.65) | 0.33 | 0.48 (0.15–1.56) | 0.22 |
| Perceived barriers | ||||
| Low | 5.40 (2.34–12.45) | <0.01 * | 2.706 (0.92–7.93) | 0.07 |
| Moderate | 0.87 (0.38–2.01) | 0.75 | 0.25 (0.16–0.37) | 0.49 |
| High | 1 (reference) | 1 (reference) | ||
| Perceived benefit | ||||
| Low | 1 (reference) | 1 (reference) | ||
| Moderate | 3.45 (1.57–7.57) | <0.01 * | 0.50 (0.16–1.55) | 0.23 |
| High | 19.17 (8.70–42.26) | <0.01 * | 1.78 (0.56–5.66) | 0.33 |
| Cues to action | ||||
| Low | 1 (reference) | 1 (reference) | ||
| Moderate | 7.30 (3.90–13.67) | <0.01 * | 3.91 (1.68–9.10) | <0.01 * |
| High | 61.28 (32.17–116.72) | <0.01 * | 23.66 (9.97–56.23) | <0.01 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qin, C.; Wang, R.; Tao, L.; Liu, M.; Liu, J. Acceptance of a Third Dose of COVID-19 Vaccine and Associated Factors in China Based on Health Belief Model: A National Cross-Sectional Study. Vaccines 2022, 10, 89. https://doi.org/10.3390/vaccines10010089
Qin C, Wang R, Tao L, Liu M, Liu J. Acceptance of a Third Dose of COVID-19 Vaccine and Associated Factors in China Based on Health Belief Model: A National Cross-Sectional Study. Vaccines. 2022; 10(1):89. https://doi.org/10.3390/vaccines10010089
Chicago/Turabian StyleQin, Chenyuan, Ruitong Wang, Liyuan Tao, Min Liu, and Jue Liu. 2022. "Acceptance of a Third Dose of COVID-19 Vaccine and Associated Factors in China Based on Health Belief Model: A National Cross-Sectional Study" Vaccines 10, no. 1: 89. https://doi.org/10.3390/vaccines10010089