
Declining Prevalence of SARS-CoV-2 Antibodies among Vaccinated Nursing Home Residents and Staff Six Months after the Primary BNT162b2 Vaccination Campaign in Belgium: A Prospective Cohort Study
 , , ,
, , ,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Size
2.2. Study Population and Recruitment
2.3. Ethical Considerations
2.4. Data Collection
2.4.1. Antibody Testing
2.4.2. Questionnaire
2.5. Statistical Analysis
3. Results
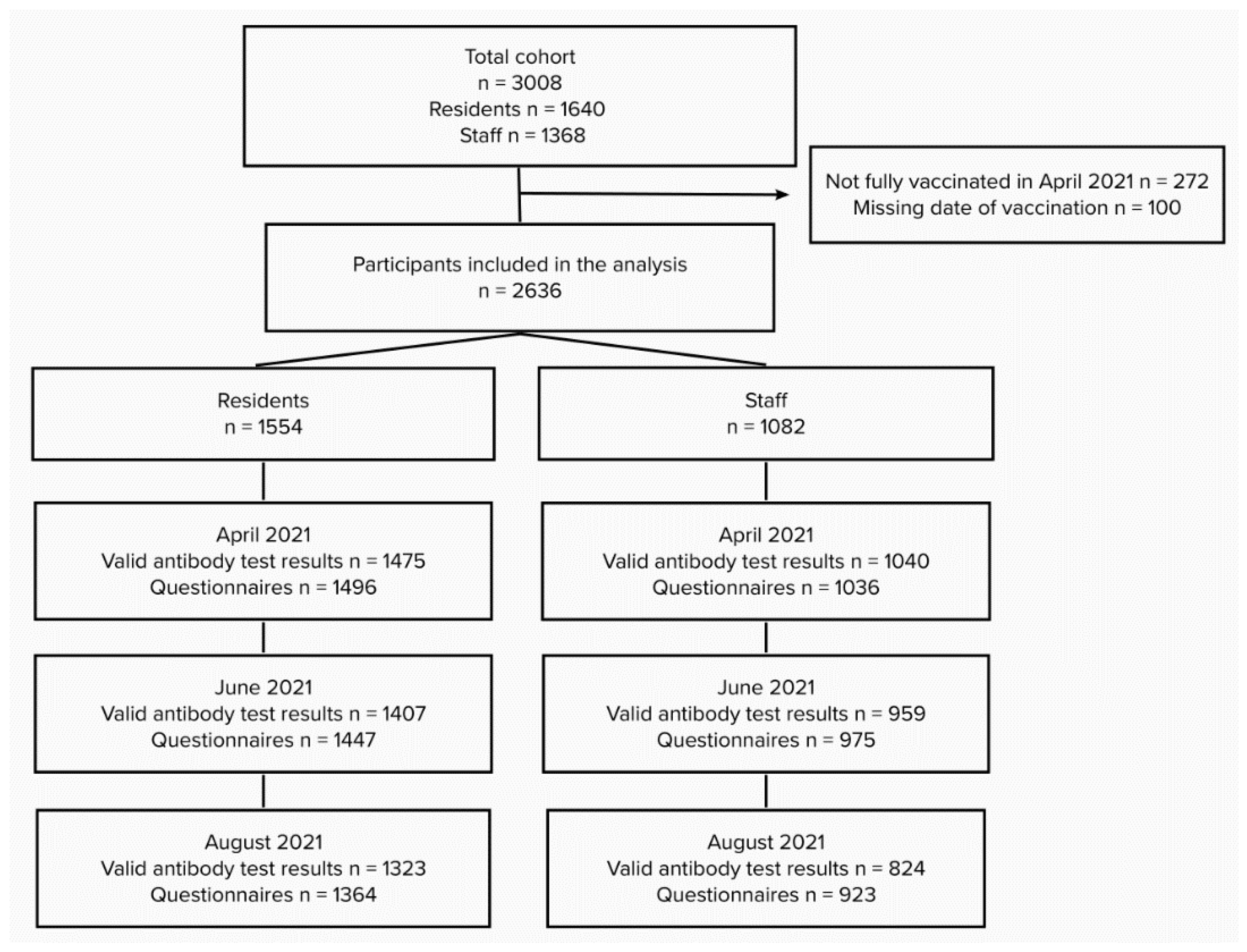
3.1. Participation
3.2. Participant Characteristics
3.3. Prevalence of SARS-CoV-2 Antibodies among NHR and NHS Four and Six Months after BNT162b2 Vaccination
3.4. Association between SARS-CoV-2 Seropositivity and Age, Comorbidities, Care Dependency, Self-Reported History of SARS-CoV-2 Infection, and Time after Vaccination in NHR and NHS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peeters, I.; Vermeulen, M.; Bustos Sierra, N.; Renard, F.; Van der Heyden, J.; Scohy, A.; Braeye, T.; Bossuyt, N.; Haarhuis, F.; Proesmans, K.; et al. Surveillance van COVID-19 Gerelateerde Mortaliteit in België, Epidemiologie en Methodologie Tijdens 1e en 2e Golf (Maart 2020–14 Februari 2021); Contract No.: D/2021/14.440/55; Sciensano: Brussels, Belgium, 2021. [Google Scholar]
- Control ECDC. Overview of the Implementation of COVID-19 Vaccination Strategies and Deployment Plans in the EU/EEA14 June 2021; ECDC: Stockholm, Sweden, 2021.
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Bewoner Woonzorgcentrum Gemiddeld 87 Jaar Zorg en Ondersteuning voor Ouderen-Statistiek Vlaanderen: Intermutalistisch Agentschap. 2022. Available online: https://www.vlaanderen.be/statistiek-vlaanderen/zorg/zorg-en-ondersteuning-voor-ouderen#bronnen (accessed on 26 April 2022).
- Akner, G. Analysis of multimorbidity in individual elderly nursing home residents. Development of a multimorbidity matrix. Arch. Gerontol. Geriatr. 2009, 49, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Kwetkat, A.; Heppner, H.J. Comorbidities in the Elderly and Their Possible Influence on Vaccine Response. Interdiscip. Top. Gerontol. Geriatr. 2020, 43, 73–85. [Google Scholar] [PubMed]
- Remarque, E.J.; de Bruijn, I.A.; Boersma, W.J.A.; Masurel, N.; Ligthart, G.J. Altered antibody response to influenza H1N1 vaccine in healthy elderly people as determined by HI, ELISA, and neutralization assay. J. Med. Virol. 1998, 55, 82–87. [Google Scholar] [CrossRef]
- Ridda, I.; Macintyre, C.R.; Lindley, R.; Gao, Z.; Sullivan, J.S.; Yuan, F.F.; Gao, Z.; Sullivan, J.S.; Yuan, F.F.; McIntyre, P.B. Immunological responses to pneumococcal vaccine in frail older people. Vaccine 2009, 27, 1628–1636. [Google Scholar] [CrossRef]
- Nath, K.; Viswanathan, S.; Upham, J.; Davies, J.; Towers, M.; Looke, D.; Pritchard, A.; Burel, J. Clinical factors associated with the humoral immune response to influenza vaccination in chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2013, 9, 51–56. [Google Scholar] [CrossRef] [Green Version]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R. Waning Immune Humoral Response to BNT162b2 COVID-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Spike-antibody waning after second dose of BNT162b2 or ChAdOx1. Lancet 2021, 398, 385–387. [Google Scholar]
- Matsunaga, H.; Takeuchi, H.; Oba, Y.; Fujimi, S.; Honda, T.; Tomonaga, K. Waning of Anti-SARS-CoV-2 Spike Antibody Levels 100 to 200 Days after the Second Dose of the BNT162b2 Vaccine. Vaccines 2022, 10, 177. [Google Scholar] [CrossRef]
- Triest, D.; Geebelen, L.; De Pauw, R.; De Craeye, S.; Vodolazkaia, A.; Verbrugghe, M.; Magerman, K.; Robben, L.; Pannus, P.; Neven, K.; et al. Performance of five rapid serological tests in mild-diseased subjects using finger prick blood for exposure assessment to SARS-CoV-2. J. Clin. Virol. 2021, 142, 104897. [Google Scholar] [CrossRef] [PubMed]
- Wallace, M.; Shelkey, M.; Hartford Institute for Geriatric Nursing. Katz Index of Independence in Activities of Daily Living (ADL). Urologic Nursing 2007, 27, 93–94. [Google Scholar] [PubMed]
- Canaday, D.H.; Carias, L.; Oyebanji, O.A.; Keresztesy, D.; Wilk, D.; Payne, M.; Aung, H.; Denis, K.S.; Lam, E.C.; Wilson, B.; et al. Reduced BNT162b2 Messenger RNA Vaccine Response in Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2)-Naive Nursing Home Residents. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, 2112–2115. [Google Scholar] [CrossRef]
- Canaday, D.H.; Oyebanji, O.A.; Keresztesy, D.; Payne, M.; Wilk, D.; Carias, L.; Aung, H.; Denis, K.S.; Lam, E.C.; Rowley, C.F.; et al. Significant Reduction in Vaccine-Induced Antibody Levels and Neutralization Activity Among Healthcare Workers and Nursing Home Residents 6 Months Following Coronavirus Disease 2019 BNT162b2 mRNA Vaccination. Clin. Infect. Dis. 2022, 75, 884–887. [Google Scholar] [CrossRef] [PubMed]
- Muller, L.; Andree, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J. Age-dependent Immune Response to the Biontech/Pfizer BNT162b2 Coronavirus Disease 2019 Vaccination. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, 2065–2072. [Google Scholar] [CrossRef]
- Witkowski, W.; Gerlo, S.; De Smet, E.; Wejda, M.; Acar, D.; Callens, S.; Heytens, S.; Padalko, E.; Vercruysse, H.; Cools, P.; et al. Humoral and Cellular Responses to COVID-19 Vaccination Indicate the Need for Post-Vaccination Testing in Frail Population. Vaccines 2022, 10, 260. [Google Scholar] [CrossRef]
- Palache, A.; Beyer, W.; Sprenger, M.; Masurel, N.; de Jonge, S.; Vardy, A.; Charpentier, B.; Noury, J.; van Beek, W.; Borst, R.; et al. Antibody response after influenza immunization with various vaccine doses: A double-blind, placebo-controlled, multi-centre, dose—Response study in elderly nursing-home residents and young volunteers. Vaccine 1993, 11, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Kovaiou, R.D.; Herndler-Brandstetter, D.; Grubeck-Loebenstein, B. Age-related changes in immunity: Implications for vaccination in the elderly. Expert Rev. Mol. Med. 2007, 9, 1–17. [Google Scholar] [CrossRef]
- Frasca, D.; Blomberg, B.B. B cell function and influenza vaccine responses in healthy aging and disease. Curr. Opin. Immunol. 2014, 29, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Earle, K.A.; Ambrosino, D.M.; Fiore-Gartland, A.; Goldblatt, D.; Gilbert, P.B.; Siber, G.R.; Dull, P.; Plotkin, S.A. Evidence for antibody as a protective correlate for COVID-19 vaccines. Vaccine 2021, 39, 4423–4428. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Sciensano. Belgium COVID-19 Epidemiological Situation: Nursing Homes Surveilance. 2022. Available online: https://datastudio.google.com/embed/reporting/7e11980c-3350-4ee3-8291-3065cc4e90c2/page/FHD7B (accessed on 6 June 2022).



{kind=link}
{kind=link}
| April 2021 | June 2021 | August 2021 | ||||
|---|---|---|---|---|---|---|
| Number a Positive/Total | Prevalence % (95% CI b) | Number a Positive/Total | Prevalence % (95% CI b) | Number a Positive/Total | Prevalence % (95% CI b) | |
| Residents | ||||||
| 60–69 | 102/107 | 95 (89–98) | 99/102 | 97 (92–99) | 68/98 | 68 (58–77) |
| 70–79 | 216/227 | 95 (90–97) | 200/218 | 91 (86–94) | 151/211 | 70 (63–76) |
| 80–89 | 647/721 | 90 (87–93) | 588/692 | 85 (81–88) | 437/648 | 68 (62–73) |
| 90+ | 352/390 | 90 (87–93) | 306/366 | 84 (79–88) | 229/339 | 69 (63–74) |
| TOTAL | 1345/1475 | 91 (89–93) | 1219/1407 | 87 (83–89) | 904/1323 | 68 (64–72) |
| Staff c | ||||||
| <30 | 171/172 | 99 (96–100) | 152/153 | 99 (95–100) | 128/139 | 92 (87–95) |
| 30–39 | 267/269 | 99 (97–100) | 234/237 | 99 (96–100) | 174/197 | 88 (83–93) |
| 40–49 | 270/272 | 99 (97–100) | 253/255 | 99 (96–100) | 181/203 | 89 (84–93) |
| 50–59 | 293/299 | 98 (95–99) | 286/289 | 99 (97–100) | 233/265 | 88 (83–91) |
| TOTAL | 1029/1040 | 99 (98–99) | 950/959 | 99 (98–100) | 734/824 | 89 (86–91) |
| Odds Ratios for SARS-CoV-2 Seropositivity | ||||||
|---|---|---|---|---|---|---|
| Residents a | Staff b | |||||
| Predictor | Odds Ratios | 95% CI c | p-Value | Odds Ratios | 95% CI c | p-Value |
| (Intercept) d | 8.18 | 6.18–10.82 | <0.001 | 78.19 | 40.71–150.18 | <0.001 |
| 4 months after vaccination (June 2021) | 0.60 | 0.50–0.72 | <0.001 | 1.34 | 0.66–2.70 | 0.417 |
| 6 months after vaccination (August 2021) | 0.17 | 0.13–0.20 | <0.001 | 0.08 | 0.04–0.15 | <0.001 |
| History of SARS-CoV-2 infection e | 19.43 | 7.73–48.83 | <0.001 | 2.38 | 0.49–11.55 | 0.281 |
| Male gender | 0.84 | 0.64–1.09 | 0.193 | 0.70 | 0.40–1.22 | 0.212 |
| Age | 0.80 | 0.69–0.91 | 0.001 | 0.87 | 0.72–1.05 | 0.146 |
| Presence of comorbidities: 1 or more g | 0.84 | 0.66–1.07 | 0.164 | NA f | NA f | NA f |
| High care dependency level: C, Cd or D h | 0.70 | 0.56–0.88 | 0.002 | NA f | NA f | NA f |
| (June 2021 * History of COVID-19 infection) i | 0.59 | 0.26–1.32 | 0.199 | 0.69 | 0.14–3.33 | 0.644 |
| (August 202 1* History of COVID-19 infection) i | 0.64 | 0.26–1.57 | 0.329 | 1.89 | 0.38–9.38 | 0.435 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyers, E.; Deschepper, E.; Duysburgh, E.; De Rop, L.; De Burghgraeve, T.; Van Ngoc, P.; Digregorio, M.; Delogne, S.; Coen, A.; De Clercq, N.; et al. Declining Prevalence of SARS-CoV-2 Antibodies among Vaccinated Nursing Home Residents and Staff Six Months after the Primary BNT162b2 Vaccination Campaign in Belgium: A Prospective Cohort Study. Viruses 2022, 14, 2361. https://doi.org/10.3390/v14112361
Meyers E, Deschepper E, Duysburgh E, De Rop L, De Burghgraeve T, Van Ngoc P, Digregorio M, Delogne S, Coen A, De Clercq N, et al. Declining Prevalence of SARS-CoV-2 Antibodies among Vaccinated Nursing Home Residents and Staff Six Months after the Primary BNT162b2 Vaccination Campaign in Belgium: A Prospective Cohort Study. Viruses. 2022; 14(11):2361. https://doi.org/10.3390/v14112361
Chicago/Turabian StyleMeyers, Eline, Ellen Deschepper, Els Duysburgh, Liselore De Rop, Tine De Burghgraeve, Pauline Van Ngoc, Marina Digregorio, Simon Delogne, Anja Coen, Nele De Clercq, and et al. 2022. "Declining Prevalence of SARS-CoV-2 Antibodies among Vaccinated Nursing Home Residents and Staff Six Months after the Primary BNT162b2 Vaccination Campaign in Belgium: A Prospective Cohort Study" Viruses 14, no. 11: 2361. https://doi.org/10.3390/v14112361