
The Relationships between HIV-1 Infection, History of Methamphetamine Use Disorder, and Soluble Biomarkers in Blood and Cerebrospinal Fluid

Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Participants
2.2. Plasma and Cerebrospinal Fluid Biomarker Sampling and Measurement
2.3. Affect Assessment and Neuropsychological Testing
2.4. Data Processing and Statistical Analyses
3. Results
3.1. Demographics
3.2. Concentrations of Individual Plasma and CSF Biomarkers
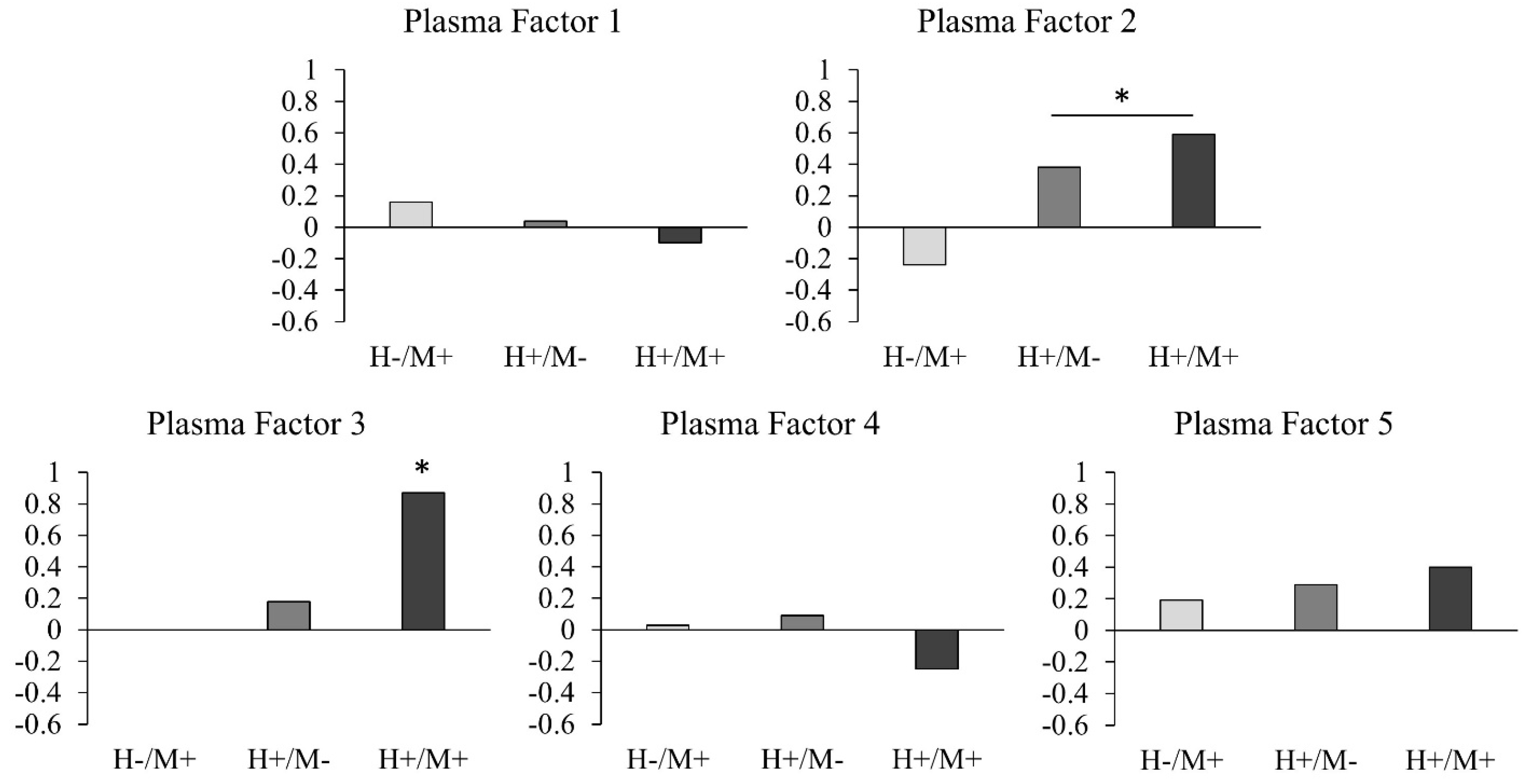
3.3. Factor Analysis of Plasma and CSF Biomarkers
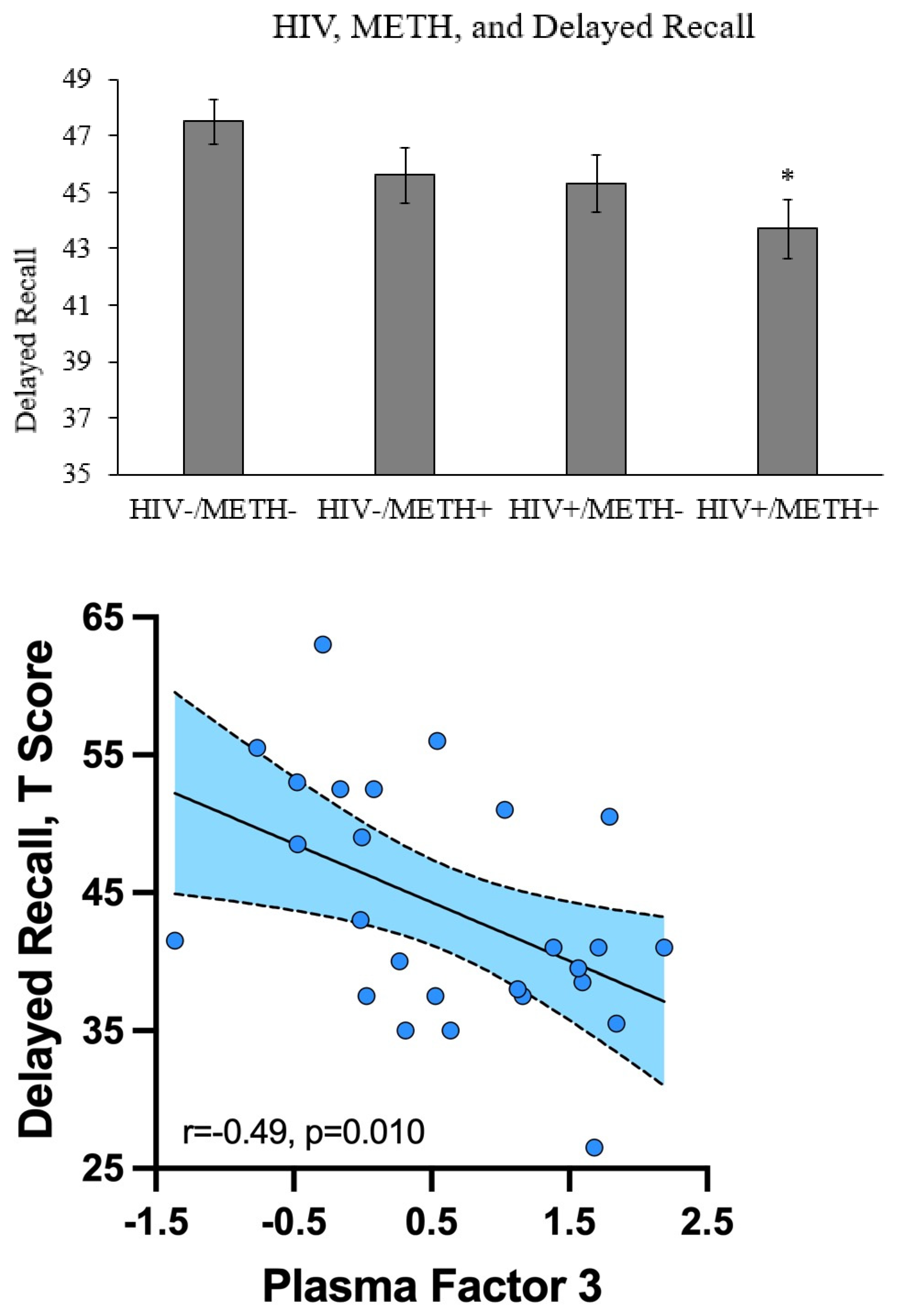
3.4. Correlations with Affective and Cognitive Measures
4. Discussion
4.1. Significance of Findings
4.2. Strengths and Limitations of This Study
4.3. Practical Implications
4.4. Directions for Future Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Hartzler, B.; Dombrowski, J.C.; Crane, H.M.; Eron, J.J.; Geng, E.H.; Mathews, W.C.; Mayer, K.H.; Moore, R.D.; Mugavero, M.J.; Napravnik, S.; et al. Prevalence and Predictors of Substance Use Disorders Among HIV Care Enrollees in the United States. AIDS Behav. 2017, 21, 1138–1148. [Google Scholar] [CrossRef]
- Clark, T.; Marquez, C.; Hare, B.C.; John, D.M.; Klausner, D.J. Methamphetamine use, transmission risk behavior and internet use among HIV-infected patients in medical care, San Francisco, 2008. AIDS Behav 2012, 16, 396–403. [Google Scholar] [CrossRef] [Green Version]
- Osuji, F.N.; Onyenekwe, C.C.; Ahaneku, J.E.; Ukibe, N.R. The effects of highly active antiretroviral therapy on the serum levels of pro-inflammatory and anti-inflammatory cytokines in HIV infected subjects. J. Biomed. Sci. 2018, 25, 1–8. [Google Scholar] [CrossRef]
- Vera, J.H.; Guo, Q.; Cole, J.H.; Boasso, A.; Greathead, L.; Kelleher, P.; Rabiner, E.A.; Kalk, N.; Bishop, C.; Gunn, R.N.; et al. Neuroinflammation in treated HIV-positive individuals: A TSPO PET study. Neurology 2016, 86, 1425–1432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papageorgiou, M.; Raza, A.; Fraser, S.; Nurgali, K.; Apostolopoulos, V. Methamphetamine and its immune-modulating effects. Maturitas 2019, 121, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Wang, Y.; Li, Q.; Zhong, Y.; Chen, L.; Du, Y.; He, J.; Liao, L.; Xiong, K.; Yi, C.-X.; et al. The Main Molecular Mechanisms Underlying Methamphetamine- Induced Neurotoxicity and Implications for Pharmacological Treatment. Front. Mol. Neurosci. 2018, 11, 186. [Google Scholar] [CrossRef] [PubMed]
- Kohno, M.; Loftis, J.M.; Huckans, M.; Dennis, L.E.; McCready, H.; Hoffman, W.F. The relationship between interleukin-6 and functional connectivity in methamphetamine users. Neurosci. Lett. 2018, 677, 49–54. [Google Scholar] [CrossRef]
- Nakajima, A.; Yamada, K.; Nagai, T.; Uchiyama, T.; Miyamoto, Y.; Mamiya, T.; He, J.; Nitta, A.; Mizuno, M.; Tran, M.H.; et al. Role of Tumor Necrosis Factor- in Methamphetamine-Induced Drug Dependence and Neurotoxicity. J. Neurosci. 2004, 24, 2212–2225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liśkiewicz, A.; Przybyła, M.; Park, M.; Liśkiewicz, D.; Nowacka-Chmielewska, M.; Małecki, A.; Barski, J.; Lewin-Kowalik, J.; Toborek, M. Methamphetamine-associated cognitive decline is attenuated by neutralizing IL-1 signaling. Brain, Behav. Immun. 2019, 80, 247–254. [Google Scholar] [CrossRef]
- Sekine, Y.; Ouchi, Y.; Sugihara, G.; Takei, N.; Yoshikawa, E.; Nakamura, K.; Iwata, Y.; Tsuchiya, K.J.; Suda, S.; Suzuki, K.; et al. Methamphetamine causes microglial activation in the brains of human abusers. J. Neurosci. 2008, 28, 5756–5761. [Google Scholar] [CrossRef]
- Letendre, S.L.; Cherner, M.; Ellis, R.; Marquie-Beck, J.; Gragg, B.; Marcotte, T.; Heaton, R.K.; McCutchan, J.A.; Grant, I. The effects of hepatitis C, HIV, and methamphetamine dependence on neuropsychological performance: Biological correlates of disease. AIDS 2005, 19, S72–S78. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Shi, Z.; Liu, J.; Wang, Y. HIV transactivator of transcription enhances methamphetamine-induced Parkinson’s-like behavior in the rats. NeuroReport 2014, 25, 860–864. [Google Scholar] [CrossRef] [Green Version]
- Fulcher, J.A.; Shoptaw, S.; Makgoeng, S.B.; Elliott, J.; Ibarrondo, F.J.; Ragsdale, A.; Brookmeyer, R.; Anton, P.A.; Gorbach, P.M. Brief Report: Recent Methamphetamine Use Is Associated with Increased Rectal Mucosal Inflammatory Cytokines, Regardless of HIV-1 Serostatus. J. Acquir. Immune Defic. Syndr. 2018, 78, 119–123. [Google Scholar] [CrossRef]
- Rippeth, J.D.; Heaton, R.K.; Carey, C.L.; Marcotte, T.D.; Moore, D.J.; Gonzalez, R.; Wolfson, T.; Grant, I. the HNRC Group Methamphetamine dependence increases risk of neuropsychological impairment in HIV infected persons. J. Int. Neuropsychol. Soc. 2004, 10, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Carey, C.L.; Woods, S.P.; Rippeth, J.D.; Gonzalez, R.; Heaton, R.K.; Grant, I. Additive Deleterious Effects of Methamphetamine Dependence and Immunosuppression on Neuropsychological Functioning in HIV Infection. AIDS Behav. 2006, 10, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Bandera, A.; Taramasso, L.; Bozzi, G.; Muscatello, A.; Robinson, J.A.; Burdo, T.H.; Gori, A. HIV-Associated Neurocognitive Impairment in the Modern ART Era: Are We Close to Discovering Reliable Biomarkers in the Setting of Virological Suppression? Front. Aging Neurosci. 2019, 11, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loftis, J.M.; Janowsky, A. Neuroimmune Basis of Methamphetamine Toxicity. Int. Rev. Neurobiol. 2014, 118, 165–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, G.S.; Robertson, G.J. Wide Range Achievement Test-4: Professional Manual; Psychological Assessment Resources, Inc.: Lutz, FL, USA, 2006. [Google Scholar]
- Heaton, R.K.; Miller, S.; Taylor, M.; Grant, I. Revised Comprehensive Norms for an Expanded Halstead-Reitan Battery: Demographically Adjusted Neuropsychological Norms for African Americans and Caucasian Adults; Psychological Assessment Resources, Inc.: Lutz, FL, USA, 2004. [Google Scholar]
- Heaton, R.K.; Taylor, M.J.; Manly, J.J. Demographic Effects and Use of Demographically Corrected Norms with the WAIS-III and WMS-III. In Clinical Interpretation of the WAIS-III and WMS-III; Academic Press: Cambridge, MA, USA, 2003; pp. 181–210. [Google Scholar]
- Harada, A.; Sekido, N.; Akahoshi, T.; Wada, T.; Mukaida, N.; Matsushima, K. Essential involvement of interleukin-8 (IL-8) in acute inflammation. J. Leukoc. Biol. 1994, 56, 559–564. [Google Scholar] [CrossRef]
- Deshmane, S.L.; Kremlev, S.; Amini, S.; Sawaya, B.E. Monocyte Chemoattractant Protein-1 (MCP-1): An Overview. J. Interf. Cytokine Res. 2009, 29, 313–326. [Google Scholar] [CrossRef]
- Cross, M.J.; Claesson-Welsh, L. FGF and VEGF function in angiogenesis: Signalling pathways, biological responses and therapeutic inhibition. Trends Pharmacol. Sci. 2001, 22, 201–207. [Google Scholar] [CrossRef]
- Angelo, L.S.; Kurzrock, R. Vascular Endothelial Growth Factor and Its Relationship to Inflammatory Mediators. Clin. Cancer Res. 2007, 13, 2825–2830. [Google Scholar] [CrossRef] [Green Version]
- Janssen, L.J. Isoprostanes: An overview and putative roles in pulmonary pathophysiology. Am. J. Physiol. Lung Cell. Mol. Physiol. 2001, 280, L1067–L1082. [Google Scholar] [CrossRef] [Green Version]
- You, T.; Bi, Y.; Li, J.; Zhang, M.; Chen, X.; Zhang, K. IL-17 induces reactive astrocytes and up-regulation of vascular endothelial growth factor (VEGF) through JAK/STAT signaling. Sci. Rep. 2017, 7, srep41779. [Google Scholar] [CrossRef] [PubMed]
- Schnittker, D.; Kwofie, K.; Ashkar, A.; Trigatti, B.; Richards, C.D. Oncostatin M and TLR-4 Ligand Synergize to Induce MCP-1, IL-6, and VEGF in Human Aortic Adventitial Fibroblasts and Smooth Muscle Cells. Mediat. Inflamm. 2013, 2013, 317503. [Google Scholar] [CrossRef] [PubMed]
- Scholz, H.; Yndestad, A.; Damås, J.K.; Wæhre, T.; Tonstad, S.; Aukrust, P.; Halvorsen, B. 8-Isoprostane increases expression of interleukin-8 in human macrophages through activation of mitogen-activated protein kinases. Cardiovasc. Res. 2003, 59, 945–954. [Google Scholar] [CrossRef] [Green Version]
- Yuan, L.; Qiao, L.; Wei, F.; Yin, J.; Liu, L.; Ji, Y.; Smith, D.; Li, N.; Chen, D. Cytokines in CSF correlate with HIV-associated neurocognitive disorders in the post-HAART era in China. J. NeuroVirology 2013, 19, 144–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, A.M.; Jang, J.H.; Easley, K.A.; Fuchs, D.; Gisslen, M.; Zetterberg, H.; Blennow, K.; Ellis, R.J.; Franklin, D.; Heaton, R.K.; et al. Cognitive and Neuronal Link with Inflammation: A Longitudinal Study in People with and Without HIV Infection. J. Acquir. Immune Defic. Syndr. 2020, 85, 617–625. [Google Scholar] [CrossRef]
- Perry, W.; Hilsabeck, R.C.; Hassanein, T.I. Cognitive Dysfunction in Chronic Hepatitis C: A Review. Dig. Dis. Sci. 2007, 53, 307–321. [Google Scholar] [CrossRef]
- Cherner, M.; Letendre, S.; Heaton, R.K.; Durelle, J.; Marquie-Beck, J.; Gragg, B.; Grant, I. Hepatitis C augments cognitive deficits associated with HIV infection and methamphetamine. Neurology 2005, 64, 1343–1347. [Google Scholar] [CrossRef]
- Meade, T.; Manolios, N.; Cumming, S.R.; Conaghan, P.G.; Katz, P. Cognitive Impairment in Rheumatoid Arthritis: A Systematic Review. Arthritis Care Res. 2018, 70, 39–52. [Google Scholar] [CrossRef]
- Kandlur, A.; Satyamoorthy, K.; Gangadharan, G. Oxidative Stress in Cognitive and Epigenetic Aging: A Retrospective Glance. Front. Mol. Neurosci. 2020, 13, 41. [Google Scholar] [CrossRef] [Green Version]
- Tangestani Fard, M.; Stough, C. A Review and Hypothesized Model of the Mechanisms That Underpin the Relationship Between Inflammation and Cognition in the Elderly. Front. Aging Neurosci. 2019, 11, 56. [Google Scholar] [CrossRef] [Green Version]
- Kraft, A.D.; Harry, G.J. Features of Microglia and Neuroinflammation Relevant to Environmental Exposure and Neurotoxicity. Int. J. Environ. Res. Public Health 2011, 8, 2980–3018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, L.; Peng, J.S.; Wang, X.; Wang, Y.J.; Luo, G.X.; Ho, W.Z. Methamphetamine enhances Hepatitis C virus replication in human hepatocytes. J. Viral Hepat. 2008, 15, 261–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salamanca, S.A.; Sorrentino, E.E.; Nosanchuk, J.D.; Martinez, L.R. Impact of methamphetamine on infection and immunity. Front. Neurosci. 2015, 8, 445. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| HIV-/METH- (n = 52) | HIV-/METH+ (n = 16) | HIV+ /METH- (n = 31) | HIV+ /METH+ (n = 26) | p Value | |
|---|---|---|---|---|---|
| Age (years) | 46.0 ± 17.0 | 39.1 ± 14.1 | 47.0 ± 14.8 | 40.0 ± 7.0 | 0.013 |
| Sex (%) | M: 48.1; F: 51.9 | M: 62.5; F: 37.5 | M: 87.1; F: 12.9 | M: 96.1; F: 3.8 | <0.0005 |
| Ethnicity (%) | Asian: 5.8; Afr Am: 15.4; Hisp: 23; Other: 0; Cauc: 55.8 | Asian: 6.2; Afr Am: 25.0; Hisp: 18.7; Other: 0; Cauc: 50.0 | Asian: 0; Afr Am: 6.5; Hisp: 29.0; Other: 3.2; Cauc: 61.3 | Asian: 0; Afr Am: 3.8; Hisp: 38.4; Other: 3.8% Cauc: 53.8 | NS |
| Education (years) | 15.0 ± 2.0 | 12.2 ± 2.8 | 14.4 ± 2.4 | 14.2 ± 2.1 | 0.024 |
| Age at first METH use (years) | - | 24.5 ± 12.8 | - | 25.7 ± 8.0 | NS |
| Days since last METH use (days) | - | 260 ± 524 | - | 168 ± 169 | NS |
| Total quantity METH use (grams) | - | 6346 ± 11,530 | - | 2382 ± 2691 | NS |
| Current CD4+ cell count (cells/uL) | - | - | 750 ± 309 | 665 ± 257 | NS |
| Estimated duration of HIV infection (years) | - | - | 13.1 ± 10.1 | 8.0 ± 5.5 | 0.025 |
| Plasma HIV RNA < 50 copies/mL (%) | - | - | 83.9 | 84.6 | NS |
| Current ART use (%) | - | - | 90.3 | 100 | NS |
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | |
|---|---|---|---|---|---|
| CRP | 0.843 | ||||
| IL-6 | 0.730 | ||||
| D-dimer | 0.581 | ||||
| CXCL10 | 0.753 | ||||
| sTNFR2 | 0.694 | ||||
| ICAM1 | 0.635 | ||||
| uPAR | 0.566 | ||||
| IL-8 | 0.737 | ||||
| VEGF | 0.713 | ||||
| Ccl2 | 0.671 | ||||
| 8-isoprostane | 0.532 | ||||
| 8-oxo-dG | 0.781 | ||||
| MDA | 0.621 | ||||
| sCD14 | 0.834 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walter, T.J.; Iudicello, J.; Cookson, D.R.; Franklin, D.; Tang, B.; Young, J.W.; Perry, W.; Ellis, R.; Heaton, R.K.; Grant, I.; et al. The Relationships between HIV-1 Infection, History of Methamphetamine Use Disorder, and Soluble Biomarkers in Blood and Cerebrospinal Fluid. Viruses 2021, 13, 1287. https://doi.org/10.3390/v13071287
Walter TJ, Iudicello J, Cookson DR, Franklin D, Tang B, Young JW, Perry W, Ellis R, Heaton RK, Grant I, et al. The Relationships between HIV-1 Infection, History of Methamphetamine Use Disorder, and Soluble Biomarkers in Blood and Cerebrospinal Fluid. Viruses. 2021; 13(7):1287. https://doi.org/10.3390/v13071287
Chicago/Turabian StyleWalter, T. Jordan, Jennifer Iudicello, Debra Rosario Cookson, Donald Franklin, Bin Tang, Jared W. Young, William Perry, Ronald Ellis, Robert K. Heaton, Igor Grant, and et al. 2021. "The Relationships between HIV-1 Infection, History of Methamphetamine Use Disorder, and Soluble Biomarkers in Blood and Cerebrospinal Fluid" Viruses 13, no. 7: 1287. https://doi.org/10.3390/v13071287