Epidemiology and Clinical Symptoms Related to Seasonal Coronavirus Identified in Patients with Acute Respiratory Infections Consulting in Primary Care over Six Influenza Seasons (2014–2020) in France

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
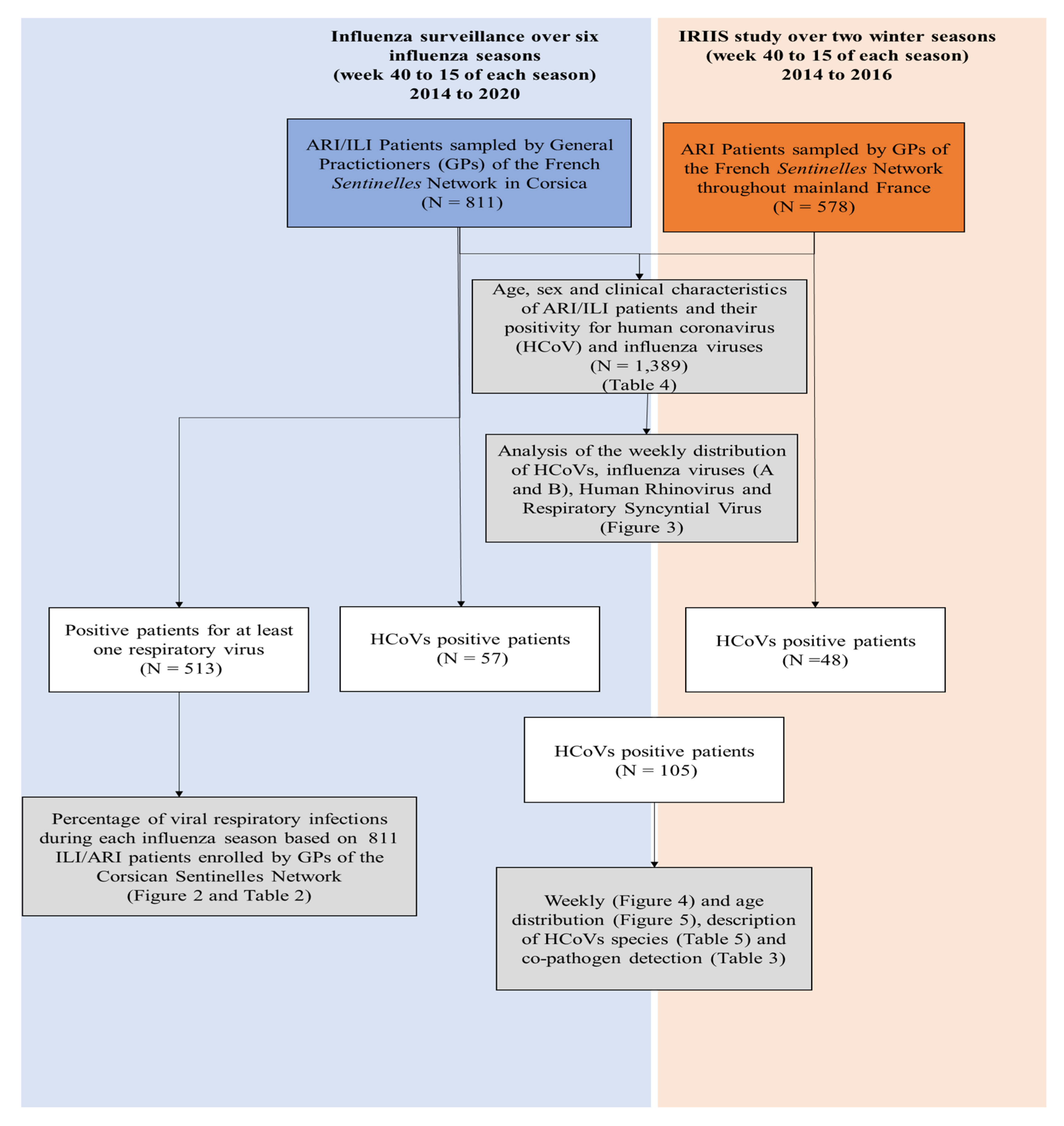
2.1. Clinical Samples
2.2. Viral Diagnostic Testing
2.3. Seasonality of HCoVs in ILI/ARI Patients in General Practice
2.4. Ethical Considerations
2.5. Statistical Analysis
3. Results
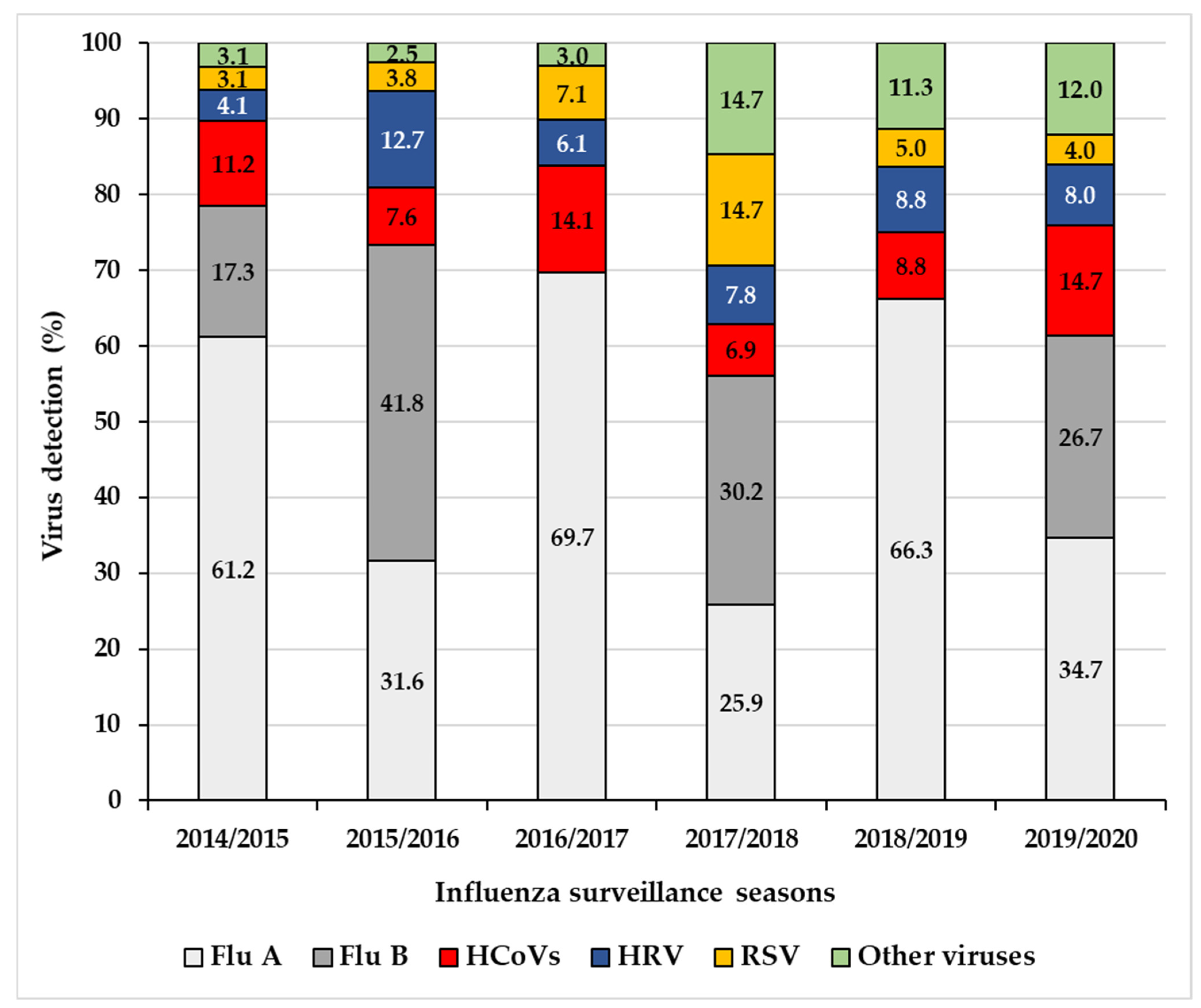
3.1. HCoV Prevalence over Six Influenza Seasons among Patients with ILI/ARI Seen in General Practice in Corsica
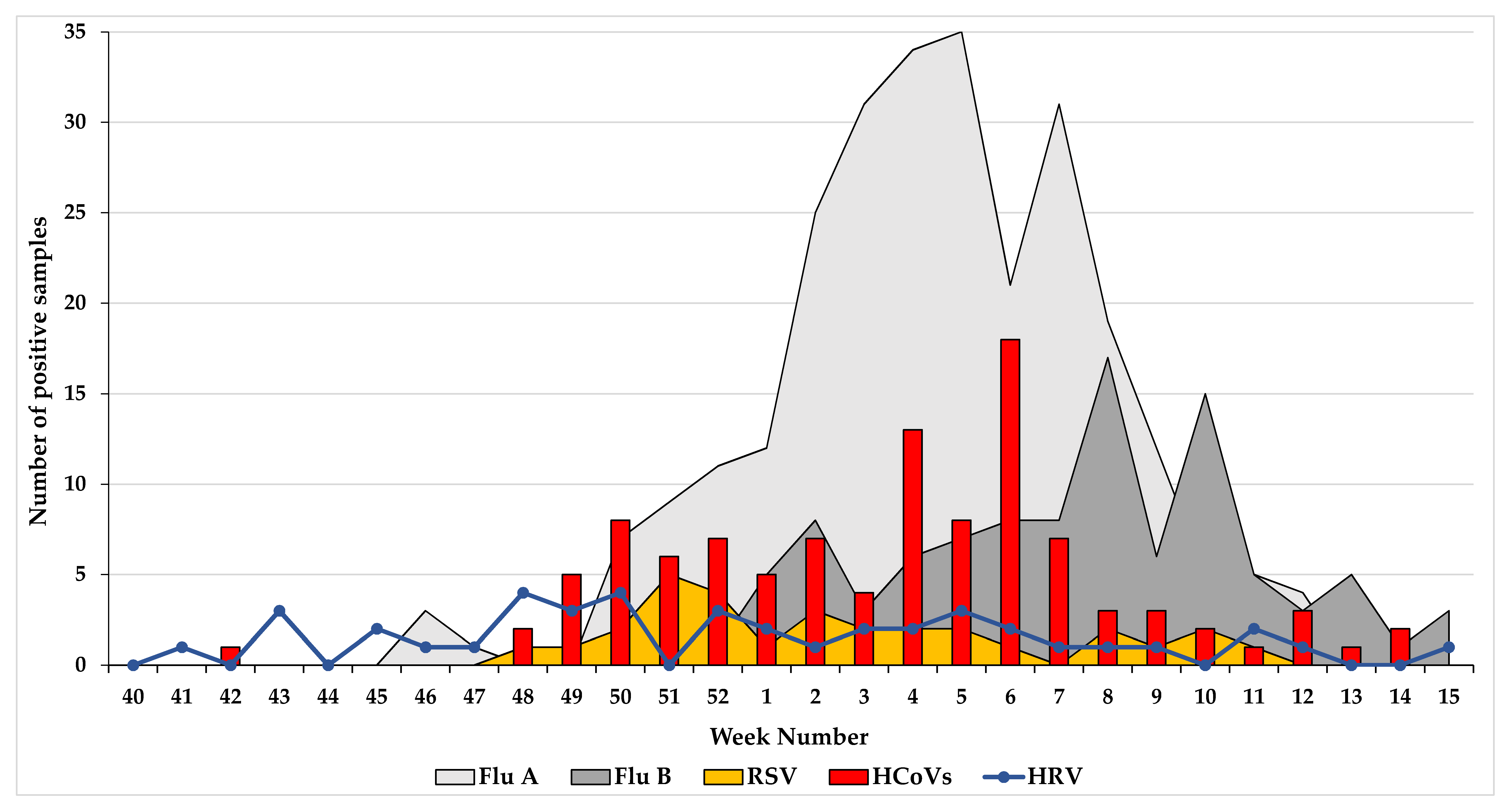
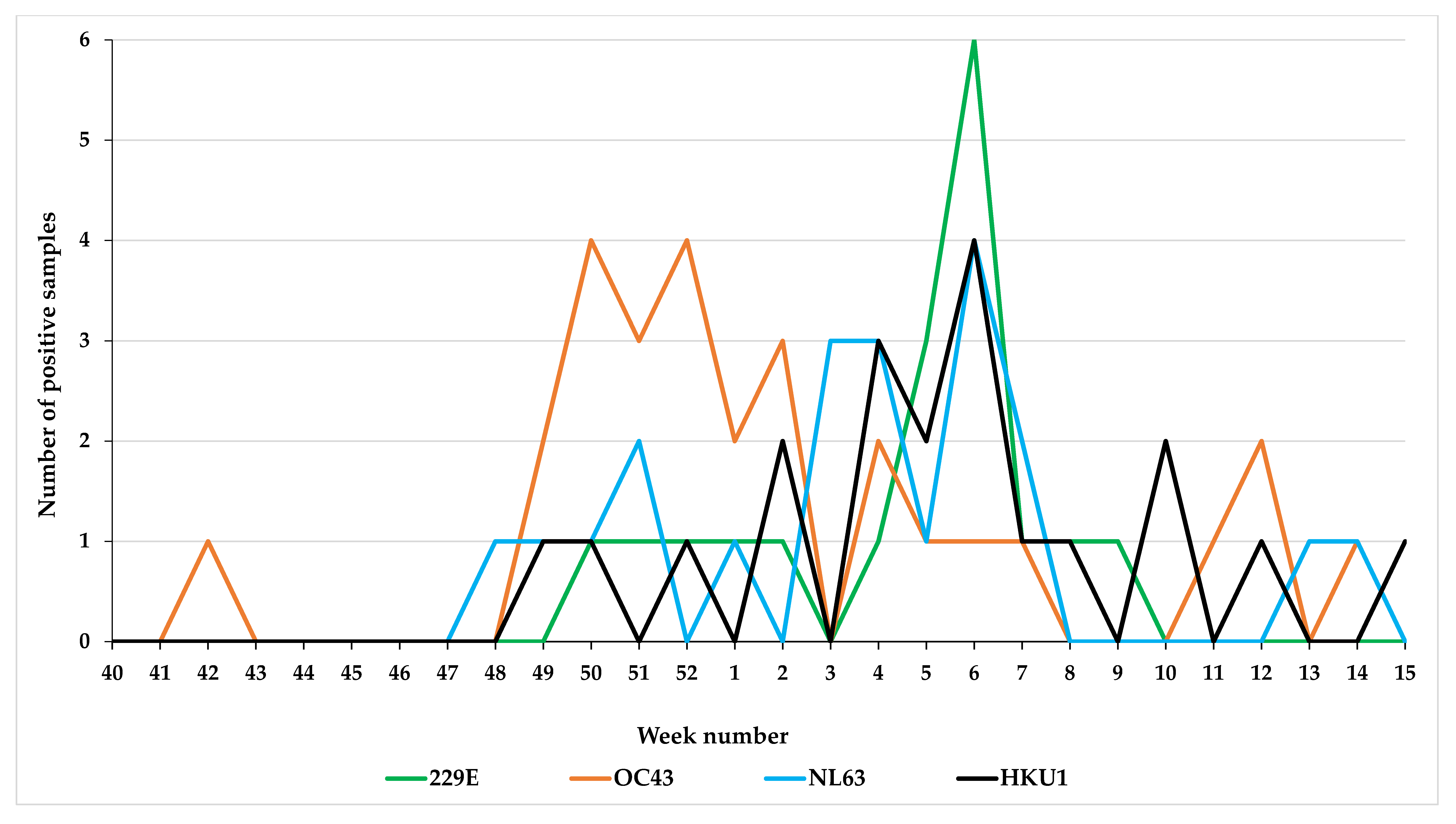
3.2. Seasonality of HCoVs
3.3. Co-Infection in HCoV-Positive Patients
3.4. Age Distribution of HCoV-Positive Patients
3.5. Clinical Characteristics of ARI/ILI Patients and Comparison of Patients according to Their Viral Infection
3.6. Clinical Description of SARS-CoV-2-Positive Patients Seen in General Practice
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cui, J.; Li, F.; Shi, Z. Origin and evolution of pathogenic coronaviruses. Nat. Rev. Genet. 2018, 17, 181–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabeça, T.K.; Granato, C.; Bellei, N.C.J. Epidemiological and clinical features of human coronavirus infections among different subsets of patients. Influ. Other Respir. Viruses 2013, 7, 1040–1047. [Google Scholar] [CrossRef] [PubMed]
- Esper, F.; Ou, Z.; Huang, Y.T. Human coronaviruses are uncommon in patients with gastrointestinal illness. J. Clin. Virol. 2010, 48, 131–133. [Google Scholar] [CrossRef] [PubMed]
- Perlman, S.; Netland, J. Coronaviruses post-SARS: Update on replication and pathogenesis. Nat. Rev. Genet. 2009, 7, 439–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. SARS (Severe Acute Respiratory Syndrome); WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Zaki, A.M.; Van Boheemen, S.; Bestebroer, T.; Osterhaus, A.; Fouchier, R. Isolation of a Novel Coronavirus from a Man with Pneumonia in Saudi Arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef] [PubMed]
- WHO. Coronavirus Disease (COVID-19) Outbreak; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Graham, N.M.H. THE EPIDEMIOLOGY OF ACUTE RESPIRATORY INFECTIONS IN CHILDREN AND ADULTS: A GLOBAL PERSPECTIVE. Epidemiol. Rev. 1990, 12, 149–178. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.; Alter, H.; Hindiyeh, M.; Mendelson, E.; Shemer-Avni, Y.; Mandelboim, M. Human Coronavirus Infections in Israel: Epidemiology, Clinical Symptoms and Summer Seasonality of HCoV-HKU1. Viruses 2018, 10, 515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamre, D.; Procknow, J.J. A New Virus Isolated from the Human Respiratory Tract? Exp. Boil. Med. 1966, 121, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Almeida, J.D.; Tyrrell, D.A.J. The Morphology of Three Previously Uncharacterized Human Respiratory Viruses that Grow in Organ Culture. J. Gen. Virol. 1967, 1, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Van Der Hoek, L.; Pyrc, K.; Jebbink, M.F.; Vermeulen-Oost, W.; Berkhout, R.J.M.; Wolthers, K.C.; Dillen, P.M.E.W.-V.; Kaandorp, J.; Spaargaren, J.; Berkhout, B. Identification of a new human coronavirus. Nat. Med. 2004, 10, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Woo, P.C.Y.; Lau, S.K.P.; Chu, C.-M.; Chan, K.-H.; Tsoi, H.-W.; Huang, Y.; Wong, B.H.L.; Poon, R.W.S.; Cai, J.J.; Luk, W.-K.; et al. Characterization and Complete Genome Sequence of a Novel Coronavirus, Coronavirus HKU1, from Patients with Pneumonia. J. Virol. 2005, 79, 884–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaunt, E.R.; Hardie, A.; Claas, E.C.J.; Simmonds, P.; Templeton, K.E. Epidemiology and Clinical Presentations of the Four Human Coronaviruses 229E, HKU1, NL63, and OC43 Detected over 3 Years Using a Novel Multiplex Real-Time PCR Method. J. Clin. Microbiol. 2010, 48, 2940–2947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, J.W.; Lam, T.T.-Y.; Zaraket, H.; Lipkin, W.I.; Drews, S.J.; Hatchette, T.F.; Heraud, J.-M.; Koopmans, M.P.G.; Abraham, A.; Baraket, A.; et al. Global epidemiology of non-influenza RNA respiratory viruses: Data gaps and a growing need for surveillance. Lancet Infect. Dis. 2017, 17, e320–e326. [Google Scholar] [CrossRef]
- Jean, A.; Quach, C.; Yung, A.; Semret, M. Severity and Outcome Associated With Human Coronavirus OC43 Infections Among Children. Pediatr. Infect. Dis. J. 2013, 32, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Gagneur, A.; Vallet, S.; Talbot, P.J.; Legrand-Quillien, M.; Picard, B.; Payan, C.; Sizun, J. Outbreaks of human coronavirus in a pediatric and neonatal intensive care unit. Eur. J. Pediatr. 2008, 167, 1427–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hand, J.; Rose, E.B.; Salinas, A.; Lu, X.; Sakthivel, S.K.; Schneider, E.; Watson, J.T. Severe Respiratory Illness Outbreak Associated with Human Coronavirus NL63 in a Long-Term Care Facility. Emerg. Infect. Dis. 2018, 24, 1964–1966. [Google Scholar] [CrossRef] [PubMed]
- Kozak, R.; Prost, K.; Yip, L.; Williams, V.; Leis, J.A.; Mubareka, S. Severity of coronavirus respiratory tract infections in adults admitted to acute care in Toronto, Ontario. J. Clin. Virol. 2020, 126, 104338. [Google Scholar] [CrossRef] [PubMed]
- Minodier, L.; Masse, S.; Capai, L.; Blanchon, T.; Ceccaldi, P.; Werf, S.; Hanslik, T.; Charrel, R.; Falchi, A. Risk factors for seasonal influenza virus detection in stools of patients consulting in general practice for acute respiratory infections in France, 2014-2016. Influ. Other Respir. Viruses 2019, 13, 398–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Real-Time Rt-Pcr-Assays for the Detection of SARS-CoV-2 Institut Pasteur Paris; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Zimmermann, P.; Curtis, N. Coronavirus Infections in Children Including COVID-19. Pediatr. Infect. Dis. J. 2020, 39, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Jevšnik, M.; Uršič, T.; Žigon, N.; Lusa, L.; Krivec, U.; Petrovec, M. Coronavirus infections in hospitalized pediatric patients with acute respiratory tract disease. BMC Infect. Dis. 2012, 12, 365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heimdal, I.; Moe, N.; Krokstad, S.; Christensen, A.; Skanke, L.H.; Nordbø, S.A.; Døllner, H. Human Coronavirus in Hospitalized Children With Respiratory Tract Infections: A 9-Year Population-Based Study From Norway. J. Infect. Dis. 2019, 219, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Monto, A.S.; Dejonge, P.M.; Callear, A.P.; Bazzi, L.A.; Capriola, S.B.; Malosh, R.E.; Martin, E.T.; Petrie, J.G. Coronavirus Occurrence and Transmission Over 8 Years in the HIVE Cohort of Households in Michigan. J. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.-Q.; Chen, D.-H.; Tan, W.-P.; Qiu, S.-Y.; Xu, D.; Liang, H.-X.; Chen, M.-X.; Li, X.; Lin, Z.-S.; Liu, W.-K.; et al. Epidemiology and clinical characteristics of human coronaviruses OC43, 229E, NL63, and HKU1: A study of hospitalized children with acute respiratory tract infection in Guangzhou, China. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 37, 363–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varghese, L.; Zachariah, P.; Vargas, C.; LaRussa, P.; Demmer, R.T.; Furuya, Y.E.; Whittier, S.; Reed, C.; Stockwell, M.S.; Saiman, L. Epidemiology and Clinical Features of Human Coronaviruses in the Pediatric Population. J. Pediatr. Infect. Dis. Soc. 2017, 7, 151–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Killerby, M.E.; Biggs, H.M.; Haynes, A.; Dahl, R.M.; Mustaquim, D.; Gerber, S.I.; Watson, J.T. Human coronavirus circulation in the United States 2014–2017. J. Clin. Virol. 2018, 101, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Dijkman, R.; Jebbink, M.F.; Gaunt, E.R.; Rossen, J.W.; Templeton, K.E.; Kuijpers, T.W.; Van Der Hoek, L. The dominance of human coronavirus OC43 and NL63 infections in infants. J. Clin. Virol. 2012, 53, 135–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vabret, A.; Brouard, J.; Petitjean, J.; Eugene-Ruellan, G.; Freymuth, F. Human coronavirus infections: Importance and diagnosis. La Presse Médicale 1998, 27, 1813–1817. [Google Scholar] [PubMed]
- Parri, N.; Magistà, A.M.; Marchetti, F.; Cantoni, B.; Arrighini, A.; Romanengo, M.; Felici, E.; Urbino, A.; Da Dalt, L.; Verdoni, L.; et al. Characteristic of COVID-19 infection in pediatric patients: Early findings from two Italian Pediatric Research Networks. Eur. J. Nucl. Med. Mol. Imaging 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nickbakhsh, S.; Ho, A.; Marques, D.F.P.; McMenamin, J.; Gunson, R.N.; Murcia, P.R. Epidemiology of Seasonal Coronaviruses: Establishing the Context for the Emergence of Coronavirus Disease 2019. J. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorse, G.J.; Donovan, M.M.; Patel, G.B. Antibodies to coronaviruses are higher in older compared with younger adults and binding antibodies are more sensitive than neutralizing antibodies in identifying coronavirus-associated illnesses. J. Med. Virol. 2020, 92, 512–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, X.; Lu, R.; Wang, Z.; Zhu, N.; Wang, W.; Julian, D.; Chris, B.; Lu, J.; Tan, W. Etiology and clinical characterization of respiratory virus infections in adult patients attending an emergency department in Beijing. PLoS ONE 2012, 7, e32174. [Google Scholar]
- Debiaggi, M.; Canducci, F.; Ceresola, E.R.; Clementi, M. The role of infections and coinfections with newly identified and emerging respiratory viruses in children. Virol. J. 2012, 9, 247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaung, J.; Chan, D.; Pada, S.; Tambyah, P.A. Coinfection with COVID-19 and Coronavirus HKU1—The critical need for repeat testing if clinically indicated. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, C.; Yao, X.; Zhao, Y.; Wu, J.; Huang, P.; Pan, C.; Liu, S.; Pan, C. Comparative review of respiratory diseases caused by coronaviruses and influenza A viruses during epidemic season. Microbes Infect. 2020. [Google Scholar] [CrossRef] [PubMed]
- Asner, S.A.; Michelle, E.; Tran, D.; Smieja, M.; Merglen, A.; Mertz, D. Clinical Disease Severity of Respiratory Viral Co-Infection versus Single Viral Infection: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e99392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.-W.; Wu, X.-X.; Jiang, X.-G.; Xu, K.-J.; Ying, L.-J.; Ma, C.-L.; Li, S.-B.; Wang, H.-Y.; Zhang, S.; Gao, H.-N.; et al. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: Retrospective case series. BMJ 2020, 368, 606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Ge, H.; Wang, X.; Yuan, X.; Xiao, G.; Wang, C.; Deng, T.; Yuan, Q.; Xiao, X. The epidemiology and clinical information about COVID-19. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1011–1019. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Origin of Samples | Period (Week 40 to 15) | N | HCoVs | 229E | OC43 | NL63 | HKU1 | Not Typed |
|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |||
| Influenza Surveillance | 2014/2015 to 2019/2020 | 811 | 57 (7.0) | 12 (21.0) | 20 (35.1) | 11 (19.3) | 11 (19.3) | 3 (5.3) |
| IRIIS | 2015/2016 to 2016/2017 | 578 | 48 (8.3) | 6 (12.0) | 8 (16.0) | 10 (20.0) | 9 (18.0) | 17 (34.0) |
| Total | 2014/2015 to 2019/2020 | 1389 | 105 * (7.5) | 18 (17.1) | 28 (26.6) | 21 (20.0) | 20 (20.0) | 20 (18.1) |
| Overall | Flu A | Flu B | HCoVs | HRV | RSV | Other Viruses | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | n | % | n | % | n | % | n | % | n | % | n | % | |
| 2014/2015 | 151 | 60 | 39.7 | 17 | 11.3 | 11 | 7.3 | 4 | 2.6 | 3 | 2.0 | 3 | 2.0 |
| 2015/2016 | 133 | 25 | 18.8 | 33 | 24.8 | 6 | 4.5 | 10 | 7.5 | 3 | 2.3 | 2 | 1.5 |
| 2016/2017 | 140 | 69 | 49.3 | 0 | 0.0 | 14 | 10.0 | 6 | 4.3 | 7 | 5.0 | 3 | 2.1 |
| 2017/2018 | 150 | 30 | 20.0 | 35 | 23.3 | 8 | 5.3 | 9 | 6.0 | 17 | 11.3 | 17 | 11.3 |
| 2018/2019 | 118 | 53 | 44.9 | 0 | 0.0 | 7 | 5.9 | 7 | 5.9 | 4 | 3.4 | 9 | 7.6 |
| 2019/2020 | 119 | 26 | 21.8 | 20 | 16.8 | 11 | 9.2 | 6 | 5.0 | 3 | 2.5 | 9 | 7.6 |
| TOTAL | 811 | 263 | 32.4 | 105 | 12.9 | 57 | 7.0 | 42 | 5.2 | 37 | 4.6 | 43 | 5.3 |
| Co-Pathogen | HCoVs | 229E | OC43 | NL63 | HKU1 | HCoV Without Species Determination |
|---|---|---|---|---|---|---|
| Flu A | 9 | 5 | 1 | / | 2 | 1 |
| Flu B | 8 | / | 1 | 2 | 3 | 2 |
| RSV | 3 | / | / | 1 | 2 | / |
| HRV | 1 | 1 | / | / | / | / |
| HMPV | 1 | / | / | / | 1 | / |
| HAdV | 1 | / | / | 1 | / | / |
| HCoV-229E | / | 1 | / | / | ||
| HCoV-OC43 | / | / | 1 | / | ||
| HCoV-NL63 | 1 | / | / | / | ||
| HCoV-HKU1 | / | 1 | / | / | ||
| HCoV without species determination | / | / | / | / | ||
| Total | 23 * | 7 | 3 | 5 | 9 | 3 |
| Collected Variable | All Patients ARI./ILI | Patients positive | Patients HCoVs Positive | Negative for All Viruses Tested | ||||||||||||||||||||||
| Influenza Virus A | Influenza Virus B | All HCoVs Positive Patients* | p-Value | Single HCoV | Co-Pathogen | p-Value | p-Value | |||||||||||||||||||
| n | % | n | % | n | % | n | % | FluA/HCoV | FluB/HCoV | n | % | n | % | singleHCoV/ Copathogen | n | % | HCoV/ Negative | |||||||||
| Number of HCoVs positive patients | 1389 | 100.0 | 328 | 23.6 | 212 | 15.3 | 105 | 7.6 | 82 | 78.1 | 23 | 21.9 | 561 | 40.4 | ||||||||||||
| Age | Median Age (years) | 34 | 36 | 28.5 | 34 | / | / | 39.5 | 11.0 | / | 36.0 | / | ||||||||||||||
| Mean Age (Min-Max) (years) | 34.96 (0.08–97.0) | 34.53 (0.08–89) | 31.02 (0.67–91) | 34.61 (0.08–90) | 37.43 (0.50–90.0) | 24.5 (0.08–80) | 36.73 (0.25–90) | |||||||||||||||||||
| Age IQR (years) | 13–53 | 13–51 | 10–48 | 11–52 | 16.0–53.5 | 3.5–44.0 | 17.0–54.0 | |||||||||||||||||||
| n | % | n | % | n | % | n | % | p-Value | n | % | p-Value | n | % | p-Value | n | % | ||||||||||
| 0–14 years | 378 | 27.2 | 88 | 26.8 | 73 | 34.4 | 30 | 28.6 | 0.00005 | 0.908 | 0.535 | 18 | 22.0 | 0.00137 | 12 | 52.2 | 0.00005 | 0.008 | 124 | 22.1 | 0.406 | |||||
| 15–29 years | 210 | 15.1 | 42 | 12.8 | 37 | 17.5 | 14 | 13.3 | 13 | 15.9 | 1 | 4.3 | 0.295 | 93 | 16.6 | |||||||||||
| 30–44 years | 303 | 21.8 | 84 | 25.6 | 42 | 19.8 | 21 | 20.0 | 17 | 20.7 | 4 | 17.4 | 1 | 135 | 24.1 | |||||||||||
| 45–59 years | 268 | 19.3 | 69 | 21.0 | 34 | 16.0 | 25 | 23.8 | 22 | 26.8 | 3 | 13.0 | 0.267 | 104 | 18.5 | |||||||||||
| 60–74 years | 149 | 10.7 | 32 | 9.8 | 16 | 7.5 | 10 | 9.5 | 8 | 9.8 | 2 | 8.7 | 1 | 73 | 13.0 | |||||||||||
| ≥ 75 | 81 | 5.8 | 13 | 4.0 | 10 | 4.7 | 5 | 4.8 | 4 | 4.9 | 1 | 4.3 | 1 | 32 | 5.7 | |||||||||||
| Sex | Female | 758 | 54.6 | 184 | 56.1 | 110 | 51.9 | 51 | 48.6 | 0.782 | 0.216 | 0.633 | 44 | 53.7 | 0.435 | 7 | 30.4 | 0.0174 | 0.06 | 311 | 55.4 | 0.202 | ||||
| Male | 631 | 45.4 | 144 | 43.9 | 102 | 48.1 | 54 | 51.4 | 38 | 46.3 | 16 | 69.6 | 250 | 44.6 | ||||||||||||
| n | % | NA | n | % | NA | n | % | NA | n | % | NA | n | % | NA | n | % | NA | n | % | NA | ||||||
| Symptoms | Fever | 1298 | 95.2 | 25 | 321 | 98.5 | 2 | 205 | 97.2 | 1 | 94 | 91.3 | 2 | 0.00131 | 0.0439 | 72 | 88.9 | 1 | 22 | 100.0 | 1 | 0.198 | 513 | 93.4 | 12 | 0.400 |
| Cough | 1087 | 87.8 | 151 | 247 | 92.2 | 60 | 173 | 88.7 | 17 | 84 | 89.4 | 11 | 0.397 | 1 | 66 | 90.4 | 9 | 18 | 85.7 | 2 | 0.688 | 418 | 82.9 | 57 | 0.128 | |
| Sore throat | 659 | 53.2 | 151 | 125 | 46.6 | 60 | 101 | 51.8 | 17 | 64 | 68.1 | 11 | 0.000465 | 0.011 | 55 | 75.3 | 9 | 9 | 42.9 | 2 | 0.006 | 267 | 53.0 | 57 | 0.0068 | |
| Dyspnea | 241 | 19.5 | 151 | 49 | 14.9 | 0 | 31 | 14.6 | 0 | 32 | 30.5 | 0 | 0.000817 | 0.00152 | 29 | 35.4 | 0 | 3 | 13.0 | 0 | 0.04 | 91 | 16.2 | 0 | 0.000963 | |
| Rhinorrhea | 932 | 75.3 | 151 | 206 | 76.9 | 60 | 150 | 76.9 | 17 | 83 | 88.3 | 11 | 0.017 | 0.0257 | 64 | 87.7 | 9 | 19 | 90.5 | 2 | 1 | 355 | 70.4 | 57 | 0.000201 | |
| Myalgia | 666 | 69.0 | 424 | 123 | 70.7 | 154 | 120 | 74.1 | 50 | 52 | 70.3 | 31 | 1 | 0.533 | 41 | 71.9 | 25 | 11 | 64.7 | 6 | 0.561 | 288 | 71.5 | 158 | 0.889 | |
| Headache | 863 | 69.7 | 151 | 194 | 72.4 | 60 | 147 | 75.4 | 17 | 73 | 77.7 | 11 | 0.343 | 0.769 | 59 | 80.8 | 9 | 14 | 66.7 | 2 | 0.233 | 346 | 68.7 | 57 | 0.0866 | |
| Malaise | 85 | 12.0 | 681 | 26 | 12.7 | 124 | 13 | 14.3 | 121 | 3 | 3.2 | 11 | 0.0104 | 0.00844 | 2 | 2.7 | 9 | 1 | 4.8 | 2 | 0.536 | 36 | 14.9 | 319 | 0.002 | |
| Conjunctivitis | 345 | 24.8 | 0 | 67 | 20.4 | 0 | 59 | 27.8 | 0 | 32 | 30.5 | 0 | 0.0446 | 0.692 | 24 | 29.3 | 0 | 8 | 34.8 | 0 | 0.616 | 141 | 25.1 | 0 | 0.275 | |
| Vomiting | 151 | 10.9 | 0 | 32 | 9.8 | 0 | 20 | 9.4 | 0 | 15 | 14.3 | 0 | 0.208 | 0.252 | 12 | 14.6 | 0 | 3 | 13.0 | 0 | 1 | 66 | 11.8 | 0 | 0.514 | |
| Diarrhea | 154 | 11.1 | 0 | 23 | 7.0 | 0 | 23 | 10.8 | 0 | 10 | 9.5 | 0 | 0.401 | 0.845 | 9 | 11.0 | 0 | 1 | 4.3 | 0 | 0.442 | 68 | 12.1 | 0 | 0.512 | |
| Other symptoms | 184 | 21.0 | 512 | 44 | 16.2 | 56 | 21 | 18.3 | 97 | 18 | 26.9 | 38 | 0.0521 | 0.192 | 15 | 30.6 | 33 | 3 | 16.7 | 5 | 0.757 | 82 | 25.0 | 233 | 0.759 | |
| Anormal lung auscultation | 88 | 26.3 | 1055 | 24 | 25.3 | 233 | 8 | 17.0 | 165 | 8 | 38.1 | 84 | 0.282 | 0.0709 | 6 | 46.2 | 69 | 2 | 25.0 | 15 | 0.4 | 34 | 27.2 | 436 | 0.309 | |
| Other variables | Risk factors | 321 | 23.5 | 22 | 59 | 18.3 | 6 | 41 | 19.4 | 1 | 16 | 15.2 | 0 | 0.555 | 0.4 | 13 | 15.9 | 0 | 3 | 13.0 | 0 | 1 | 145 | 26.4 | 11 | 0.0182 |
| Oseltamivir | 241 | 18.0 | 49 | 88 | 27.7 | 10 | 29 | 14.0 | 5 | 14 | 13.6 | 2 | 0.00348 | 1 | 12 | 15.0 | 2 | 2 | 8.7 | 0 | 0.73 | 88 | 16.4 | 26 | 0.558 | |
| Antibiotics | 173 | 13.3 | 86 | 43 | 14.2 | 25 | 18 | 8.8 | 7 | 10 | 9.9 | 4 | 0.31 | 0.833 | 7 | 8.9 | 3 | 3 | 13.6 | 1 | 0.45 | 73 | 14.1 | 43 | 0.338 | |
| Hospitalization | 39 | 2.9 | 32 | 12 | 3.8 | 10 | 7 | 3.4 | 5 | 2 | 1.9 | 0 | 0.532 | 0.7 | 2 | 2.4 | 0 | 0 | 0.0 | 0 | 1 | 15 | 2.7 | 10 | 1 | |
| Collected Variable | Distribution of HCoV Strain | |||||||||||||
| 229E | OC43 | NL63 | HKU1 | p-Value Variation between Species | ||||||||||
| n | % | n | % | n | % | n | % | |||||||
| Number of HCoVs positive patients | 18 | 17.1 | 28 | 26.7 | 21 | 20.0 | 20 | 19.0 | ||||||
| Age | Median Age (years) | 27 | 31 | 40 | 34.5 | / | ||||||||
| Mean Age (Min-Max) (years) | 31.1 (4–69) | 33.1 (0.5–90.0) | 33.72 (0.08–68) | 36.99 (0.83–80) | ||||||||||
| Age IQR (years) | 11.25–47.5 | 7–48.25 | 15–52 | 4–60.25 | ||||||||||
| n | % | p-Value | n | % | p-Value | n | % | p-Value | n | % | p-Value | |||
| 0–14 years | 6 | 33.3 | 0.156 | 9 | 32.1 | 0.0721 | 5 | 23.8 | 0.0721 | 6 | 30.0 | 0.224 | 0.927 | |
| 15–29 years | 4 | 22.2 | 4 | 14.3 | 4 | 19.0 | 1 | 5.0 | 0.46 | |||||
| 30–44 years | 3 | 16.7 | 4 | 14.3 | 5 | 23.8 | 5 | 25.0 | 0.75 | |||||
| 45–59 years | 3 | 16.7 | 7 | 25.0 | 6 | 28.6 | 2 | 10.0 | 0.44 | |||||
| 60–74 years | 2 | 11.1 | 2 | 7.1 | 1 | 4.8 | 4 | 20.0 | 0.38 | |||||
| ≥ 75 | 0 | 0.0 | 2 | 7.1 | 0 | 0.0 | 2 | 10.0 | 0.3 | |||||
| Sex | Female | 2 | 11.1 | 0.0000005 | 15 | 53.6 | 0.79 | 13 | 61.9 | 0.217 | 11 | 55.0 | 0.752 | 0.00209 |
| Male | 16 | 88.9 | 13 | 46.4 | 8 | 38.1 | 9 | 45.0 | ||||||
| n | % | NA | n | % | NA | n | % | NA | n | % | NA | |||
| Symptoms | Fever | 17 | 94.4 | 0 | 26 | 92.9 | 0 | 16 | 84.2 | 2 | 19 | 95.0 | 0 | 0.140 |
| Cough | 14 | 100.0 | 4 | 22 | 91.7 | 4 | 17 | 89.5 | 2 | 15 | 78.9 | 1 | 0.261 | |
| Sore throat | 11 | 78.6 | 4 | 14 | 58.3 | 4 | 15 | 78.9 | 2 | 11 | 57.9 | 1 | 0.307 | |
| Dyspnea | 3 | 16.7 | 0 | 4 | 14.3 | 0 | 7 | 33.3 | 0 | 8 | 40.0 | 0 | 0.138 | |
| Rhinorrhea | 13 | 92.9 | 4 | 23 | 95.8 | 4 | 16 | 84.2 | 2 | 16 | 84.2 | 1 | 0.509 | |
| Myalgia | 7 | 77.8 | 9 | 10 | 66.7 | 13 | 13 | 76.5 | 4 | 12 | 66.7 | 2 | 0.861 | |
| Headache | 13 | 92.9 | 4 | 20 | 83.3 | 4 | 14 | 73.7 | 2 | 13 | 68.4 | 1 | 0.322 | |
| Malaise | 0 | 0.0 | 4 | 0 | 0.0 | 4 | 0 | 0.0 | 2 | 3 | 15.8 | 1 | 0.0247 | |
| Conjunctivitis | 4 | 22.2 | 0 | 11 | 39.3 | 0 | 6 | 28.6 | 0 | 6 | 30.0 | 0 | 0.656 | |
| Vomiting | 1 | 5.6 | 0 | 5 | 17.9 | 0 | 4 | 19.0 | 0 | 2 | 10.0 | 0 | 0.543 | |
| Diarrhea | 1 | 5.6 | 0 | 1 | 3.6 | 0 | 2 | 9.5 | 0 | 3 | 15.0 | 0 | 0.517 | |
| Other symptoms | 4 | 30.8 | 5 | 3 | 15.0 | 8 | 2 | 15.4 | 8 | 3 | 25.0 | 8 | 0.669 | |
| Anormal lung auscultation | 1 | 33.3 | 15 | 4 | 66.7 | 22 | 1 | 16.7 | 15 | 2 | 33.3 | 14 | 0.343 | |
| Other variables | Risk factors | 0 | 0.0 | 0 | 3 | 10.7 | 0 | 3 | 14.3 | 0 | 5 | 25.0 | 0 | 0.138 |
| Oseltamivir | 3 | 16.7 | 0 | 2 | 7.1 | 0 | 3 | 15.8 | 2 | 4 | 20.0 | 0 | 0.607 | |
| Antibiotics | 2 | 11.1 | 0 | 1 | 3.6 | 0 | 3 | 15.0 | 1 | 1 | 5.9 | 3 | 0.515 | |
| Hospitalization | 1 | 5.6 | 0 | 0 | 0.0 | 0 | 0 | 0.0 | 0 | 0 | 0.0 | 0 | 0.275 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masse, S.; Capai, L.; Villechenaud, N.; Blanchon, T.; Charrel, R.; Falchi, A. Epidemiology and Clinical Symptoms Related to Seasonal Coronavirus Identified in Patients with Acute Respiratory Infections Consulting in Primary Care over Six Influenza Seasons (2014–2020) in France. Viruses 2020, 12, 630. https://doi.org/10.3390/v12060630
Masse S, Capai L, Villechenaud N, Blanchon T, Charrel R, Falchi A. Epidemiology and Clinical Symptoms Related to Seasonal Coronavirus Identified in Patients with Acute Respiratory Infections Consulting in Primary Care over Six Influenza Seasons (2014–2020) in France. Viruses. 2020; 12(6):630. https://doi.org/10.3390/v12060630
Chicago/Turabian StyleMasse, Shirley, Lisandru Capai, Natacha Villechenaud, Thierry Blanchon, Rémi Charrel, and Alessandra Falchi. 2020. "Epidemiology and Clinical Symptoms Related to Seasonal Coronavirus Identified in Patients with Acute Respiratory Infections Consulting in Primary Care over Six Influenza Seasons (2014–2020) in France" Viruses 12, no. 6: 630. https://doi.org/10.3390/v12060630