Comparing the Efficacy of OnabotulinumtoxinA, Sacral Neuromodulation, and Peripheral Tibial Nerve Stimulation as Third Line Treatment for the Management of Overactive Bladder Symptoms in Adults: Systematic Review and Network Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Results
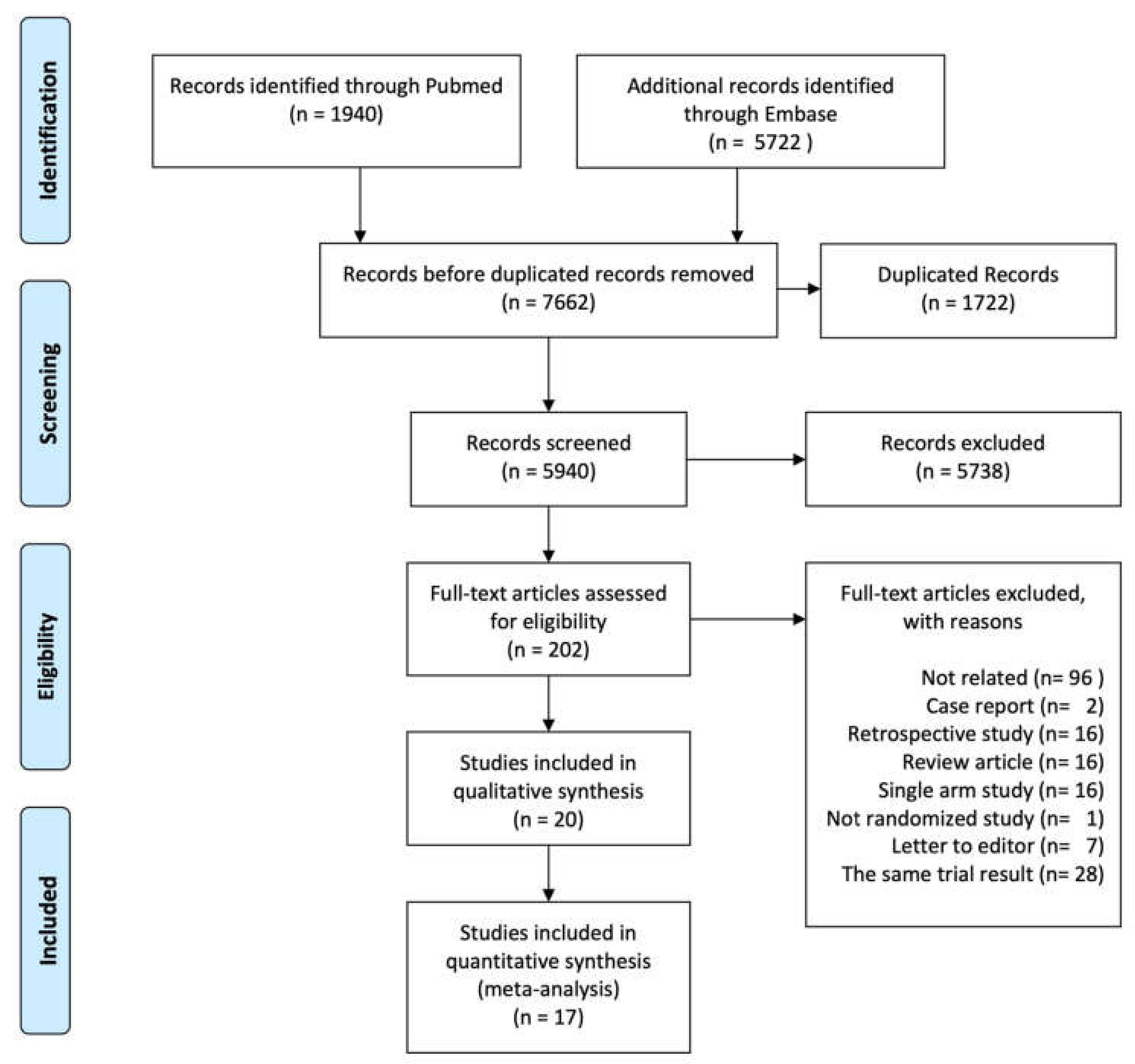
2.1. Included Studies
2.2. Study and Participant Characteristics
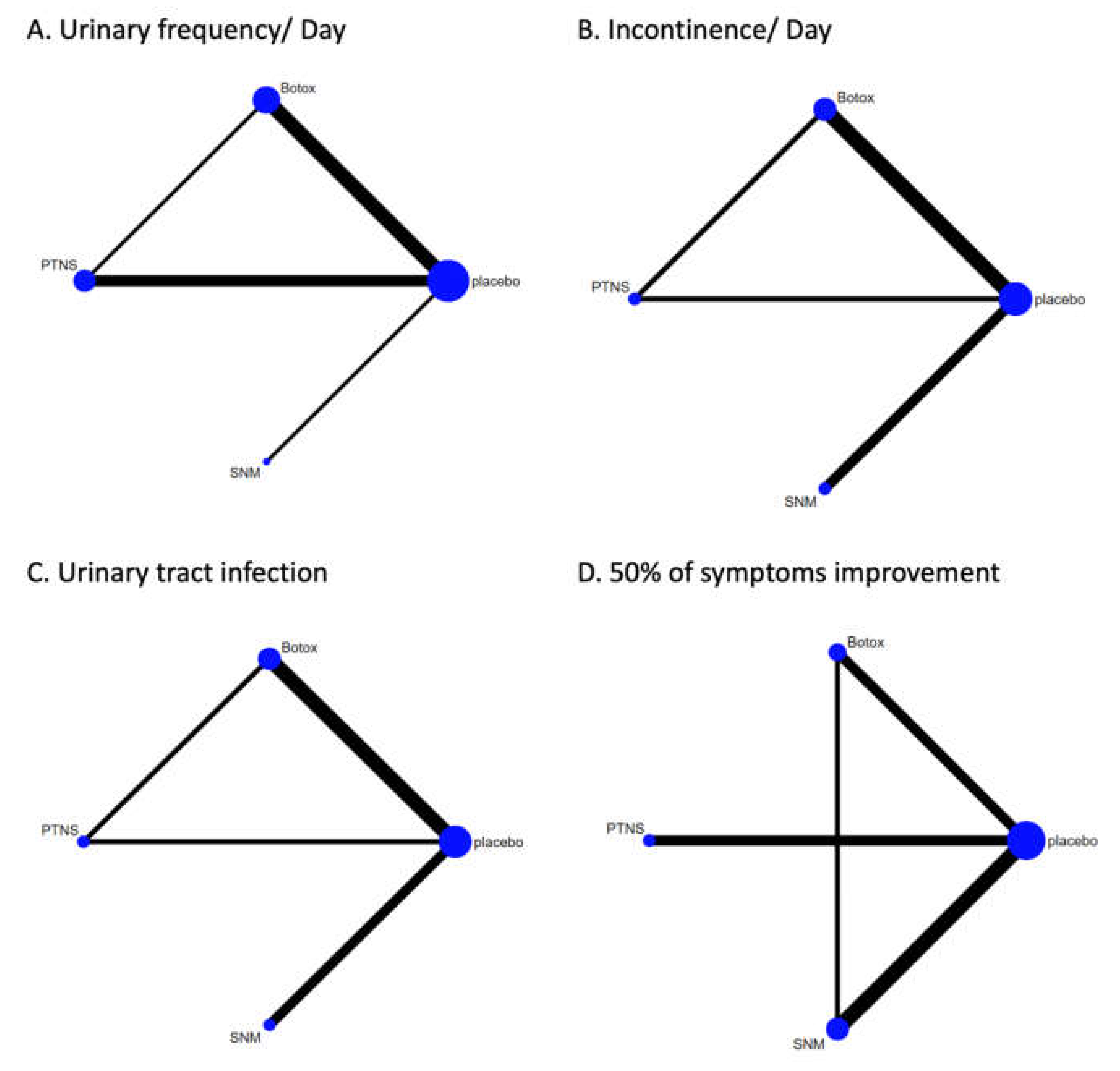
2.3. Networks
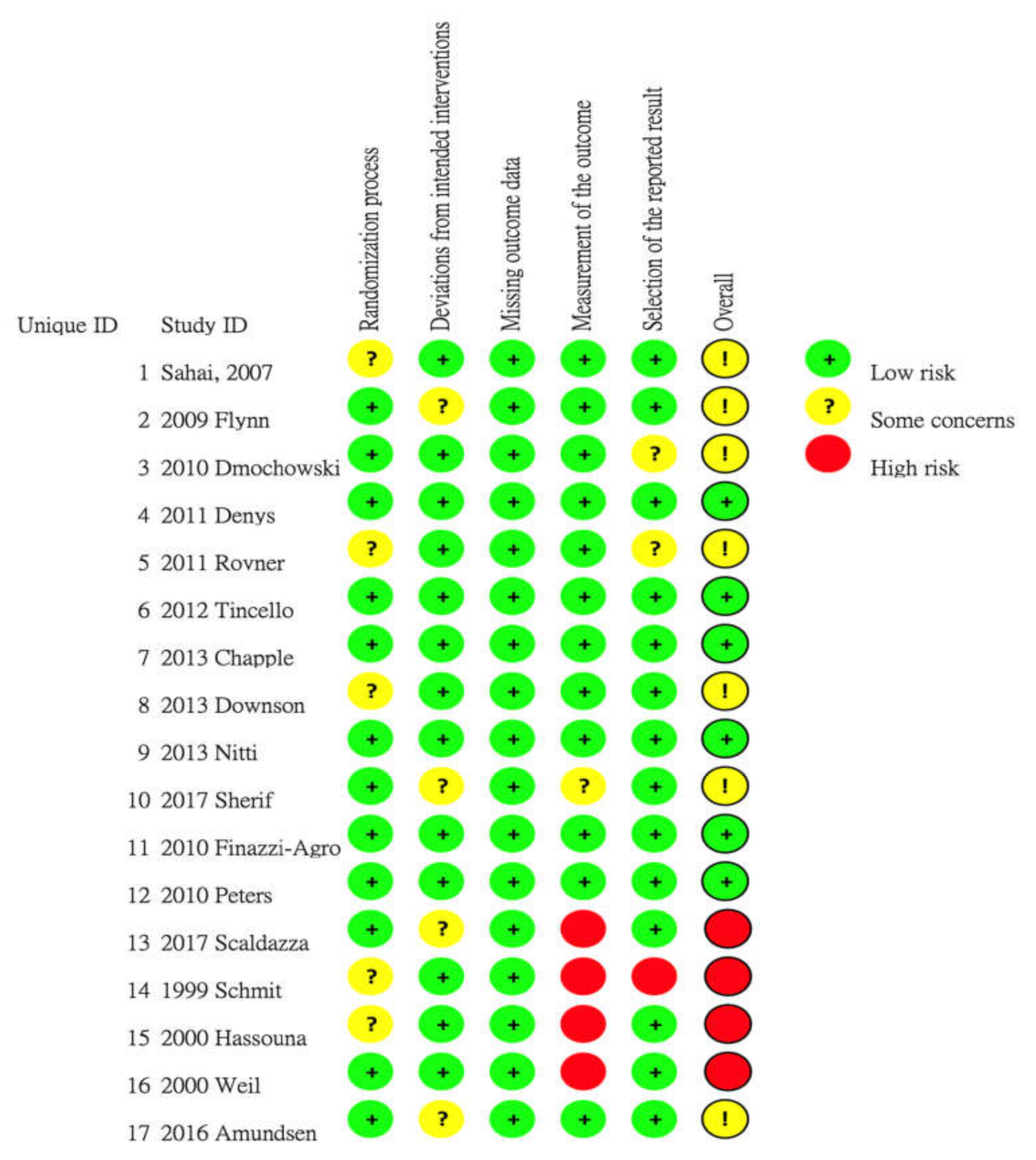
2.4. Risk of Bias Assessment
2.5. Network Meta-Analysis on the Outcomes of Interests
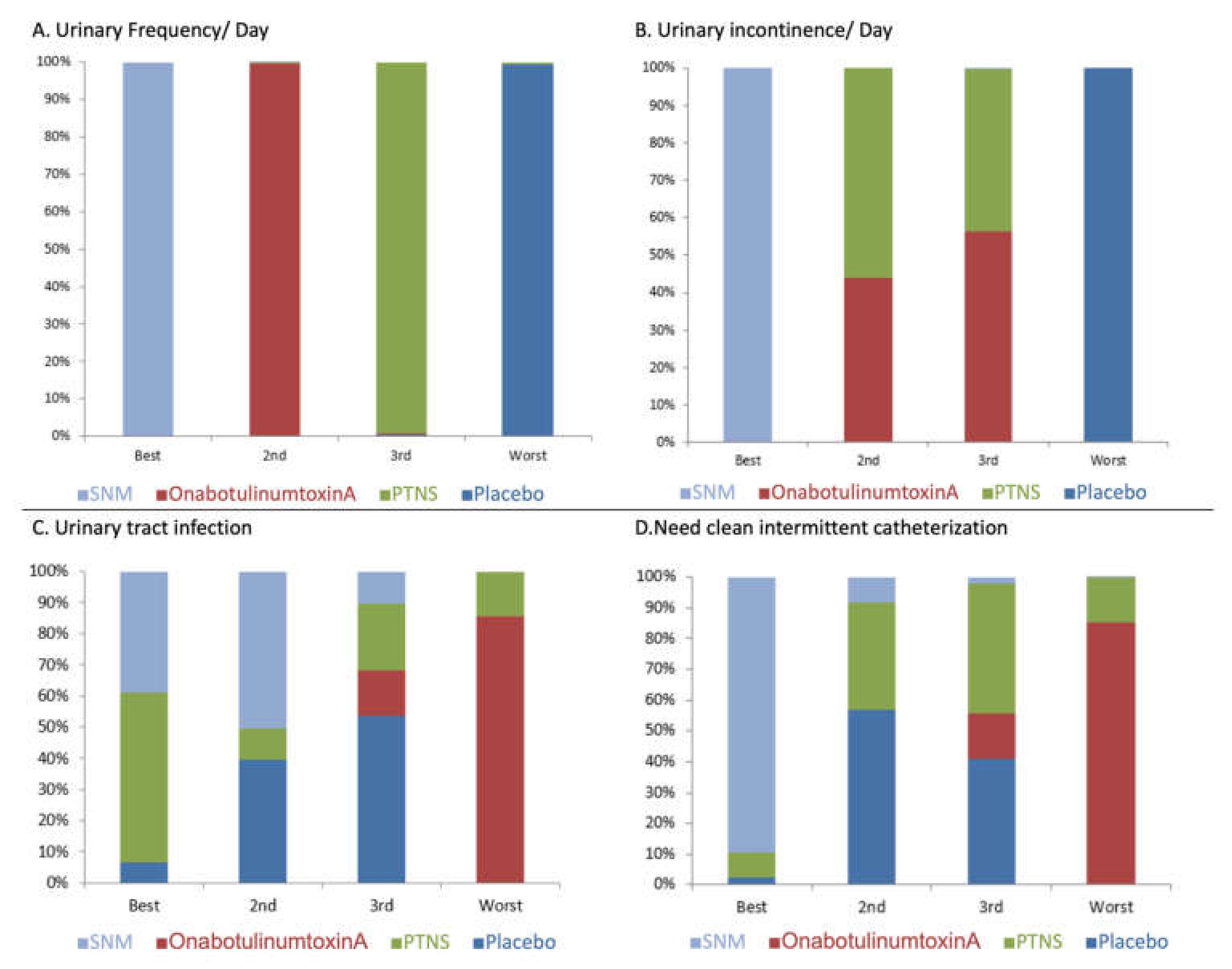
2.5.1. Efficacy
Urinary Frequency per Day
Urinary Incontinence Episodes per Day
≥50% Symptom Improvement at 12 Weeks Follow-up
2.6. Complications
2.6.1. Urinary Tract Infection
2.6.2. Urine Retention Needing Clean Intermittent Catheterization
3. Discussion
4. Conclusions
5. Material and Methods
5.1. Search Strategy and Eligibility Criteria
5.2. Data Extraction and Quality Asessment
5.3. Network Development
5.4. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
References
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; Van Kerrebroeck, P.; Victor, A.; Wein, A.; Standardisation Sub-Committee of the International Continence Society. The standardisation of terminology of lower urinary tract function: Report from the standardisation sub-committee of the international continence society. Neurourol. Urodyn. 2002, 21, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Irwin, D.E.; Kopp, Z.S.; Agatep, B.; Milsom, I.; Abrams, P. Worldwide prevalence estimates of lower urinary tract symptoms, overactive bladder, urinary incontinence and bladder outlet obstruction. BJU Int. 2011, 108, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- Lightner, D.J.; Gomelsky, A.; Souter, L.; Vasavada, S.P. Diagnosis and treatment of overactive bladder (Non-Neurogenic) in adults: AUA/SUFU guideline amendment 2019. J. Urol. 2019, 202, 558–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niu, H.L.; Ma, Y.H.; Zhang, C.J. Comparison of OnabotulinumtoxinA versus sacral neuromodulation for refractory urinary urge incontinence: A systematic review and meta-analysis of randomized controlled trials. Int. J. Surg. 2018, 60, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Arruda, R.M.; Takano, C.C.; Girão, M.J.B.C.; Haddad, J.M.; Aleixo, G.F.; Castro, R.A. Treatment of non-neurogenic overactive bladder with OnabotulinumtoxinA: Systematic review and meta-analysis of prospective, randomized, placebo-controlled clinical trials. Rev. Bras. Ginecol. Obstet. 2018, 40, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Sahai, A.; Khan, M.S.; Dasgupta, P. Efficacy of botulinum toxin-A for treating idiopathic detrusor overactivity: Results from a single center, randomized, double-blind, placebo controlled trial. J. Urol. 2007, 177, 2231–2236. [Google Scholar] [CrossRef]
- Flynn, M.K.; Amundsen, C.L.; Perevich, M.; Liu, F.; Webster, G.D. Outcome of a randomized, double-blind, placebo controlled trial of botulinum A toxin for refractory overactive bladder. J. Urol. 2009, 181, 2608–2615. [Google Scholar] [CrossRef] [Green Version]
- Dmochowski, R.; Chapple, C.; Nitti, V.W.; Chancellor, M.; Everaert, K.; Thompson, C.; Daniell, G.; Zhou, J.; Haag-Molkenteller, C. Efficacy and safety of onabotulinumtoxinA for idiopathic overactive bladder: A double-blind, placebo controlled, randomized, dose ranging trial. J. Urol. 2010, 184, 2416–2422. [Google Scholar] [CrossRef]
- Rovner, E.; Kennelly, M.; Schulte-Baukloh, H.; Zhou, J.; Haag-Molkenteller, C.; Dasgupta, P. Urodynamic results and clinical outcomes with intradetrusor injections of onabotulinumtoxinA in a randomized, placebo-controlled dose-finding study in idiopathic overactive bladder. Neurourol. Urodyn. 2011, 30, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Denys, P.; Le Normand, L.; Ghout, I.; Costa, P.; Chartier-Kastler, E.; Grise, P.; Hermieu, J.F.; Amarenco, G.; Karsenty, G.; Saussine, C.; et al. Efficacy and safety of low doses of onabotulinumtoxinA for the treatment of refractory idiopathic overactive bladder: A multicentre, double-blind, randomised, placebo-controlled dose-ranging study. Eur. Urol. 2012, 61, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Tincello, D.G.; Kenyon, S.; Abrams, K.R.; Mayne, C.; Toozs-Hobson, P.; Taylor, D.; Slack, M. Botulinum toxin a versus placebo for refractory detrusor overactivity in women: A randomised blinded placebo-controlled trial of 240 women (the RELAX study). Eur. Urol. 2012, 62, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Chapple, C.; Sievert, K.D.; MacDiarmid, S.; Khullar, V.; Radziszewski, P.; Nardo, C.; Thompson, C.; Zhou, J.; Haag-Molkenteller, C. OnabotulinumtoxinA 100 U significantly improves all idiopathic overactive bladder symptoms and quality of life in patients with overactive bladder and urinary incontinence: A randomised, double-blind, placebo-controlled trial. Eur. Urol. 2013, 64, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Dowson, C.; Sahai, A.; Watkins, J.; Dasgupta, P.; Khan, M.S. The safety and efficacy of botulinum toxin-A in the management of bladder oversensitivity: A randomised double-blind placebo-controlled trial. Int. J. Clin. Pract. 2011, 65, 698–704. [Google Scholar] [CrossRef] [Green Version]
- Nitti, V.W.; Dmochowski, R.; Herschorn, S.; Sand, P.; Thompson, C.; Nardo, C.; Yan, X.; Haag-Molkenteller, C.; EMBARK Study Group. OnabotulinumtoxinA for the treatment of patients with overactive bladder and urinary incontinence: Results of a phase 3, randomized, placebo controlled trial. J. Urol. 2013, 189, 2186–2193. [Google Scholar] [CrossRef]
- Sherif, H.; Khalil, M.; Omar, R. Management of refractory idiopathic overactive bladder: Intradetrusor injection of botulinum toxin type A versus posterior tibial nerve stimulation. Can. J. Urol. 2017, 24, 8838–8846. [Google Scholar]
- Finazzi-Agro, E.; Petta, F.; Sciobica, F.; Pasqualetti, P.; Musco, S.; Bove, P. Percutaneous tibial nerve stimulation effects on detrusor overactivity incontinence are not due to a placebo effect: A randomized, double-blind, placebo controlled trial. J. Urol. 2010, 184, 2001–2006. [Google Scholar] [CrossRef]
- Peters, K.M.; Carrico, D.J.; Perez-Marrero, R.A.; Khan, A.U.; Wooldridge, L.S.; Davis, G.L.; Macdiarmid, S.A. Randomized trial of percutaneous tibial nerve stimulation versus Sham efficacy in the treatment of overactive bladder syndrome: Results from the SUmiT trial. J. Urol. 2010, 183, 1438–1443. [Google Scholar] [CrossRef]
- Scaldazza, C.V.; Morosetti, C.; Giampieretti, R.; Lorenzetti, R.; Baroni, M. Percutaneous tibial nerve stimulation versus electrical stimulation with pelvic floor muscle training for overactive bladder syndrome in women: Results of a randomized controlled study. Int. Braz. J. Urol. 2017, 43, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, R.A.; Jonas, U.; Oleson, K.A.; Janknegt, R.A.; Hassouna, M.M.; Siegel, S.W.; van Kerrebroeck, P.E. Sacral nerve stimulation for treatment of refractory urinary urge incontinence. Sacral Nerve Stimulation Study Group. J. Urol. 1999, 162, 352–357. [Google Scholar] [CrossRef]
- Hassouna, M.M.; Siegel, S.W.; Nyeholt, A.A.; Elhilali, M.M.; van Kerrebroeck, P.E.; Das, A.K.; Gajewski, J.B.; Janknegt, R.A.; Rivas, D.A.; Dijkema, H.; et al. Sacral neuromodulation in the treatment of urgency-frequency symptoms: A multicenter study on efficacy and safety. J. Urol. 2000, 163, 1849–1854. [Google Scholar] [CrossRef]
- Weil, E.H.; Ruiz-Cerda, J.L.; Eerdmans, P.H.; Janknegt, R.A.; Bemelmans, B.L.; van Kerrebroeck, P.E. Sacral root neuromodulation in the treatment of refractory urinary urge incontinence: A prospective randomized clinical trial. Eur. Urol. 2000, 37, 161–171. [Google Scholar] [CrossRef]
- Amundsen, C.L.; Richter, H.E.; Menefee, S.A.; Komesu, Y.M.; Arya, L.A.; Gregory, W.T.; Myers, D.L.; Zyczynski, H.M.; Vasavada, S.; Nolen, T.L.; et al. OnabotulinumtoxinA vs Sacral Neuromodulation on Refractory Urgency Urinary Incontinence in Women: A Randomized Clinical Trial. JAMA 2016, 316, 1366–1374. [Google Scholar] [CrossRef] [PubMed]
- Amundsen, C.L.; Komesu, Y.M.; Chermansky, C.; Gregory, W.T.; Myers, D.L.; Honeycutt, E.F.; Vasavada, S.P.; Nguyen, J.N.; Wilson, T.S.; Harvie, H.S.; et al. Two-year outcomes of sacral neuromodulation versus OnabotulinumtoxinA for refractory urgency urinary incontinence: A randomized trial. Eur. Urol. 2018, 74, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Arlandis, S.; Castro, D.; Errando, C.; Fernandez, E.; Jimenez, M.; Gonzalez, P.; Crespo, C.; Staeuble, F.; Rodriguez, J.M.; Brosa, M. Cost-effectiveness of sacral neuromodulation compared to botulinum neurotoxin a or continued medical management in refractory overactive bladder. Value Health 2011, 14, 219–228. [Google Scholar] [CrossRef] [Green Version]
- Martinson, M.; MacDiarmid, S.; Black, E. Cost of neuromodulation therapies for overactive bladder: Percutaneous tibial nerve stimulation versus sacral nerve stimulation. J. Urol. 2013, 189, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, N.Y.; Amundsen, C.L.; Visco, A.G.; Myers, E.R.; Wu, J.M. Cost-effectiveness of sacral neuromodulation versus intravesical botulinum A toxin for treatment of refractory urge incontinence. J. Urol. 2009, 182, 2799–2804. [Google Scholar] [CrossRef] [PubMed]
- Leong, R.K.; de Wachter, S.G.; Joore, M.A.; van Kerrebroeck, P.E. Cost-effectiveness analysis of sacral neuromodulation and botulinum toxin a treatment for patients with idiopathic overactive bladder. BJU Int. 2011, 108, 558–564. [Google Scholar] [CrossRef]
- Wagg, A.; Franks, B.; Ramos, B.; Berner, T. Persistence and adherence with the new beta-3 receptor agonist, mirabegron, versus antimuscarinics in overactive bladder: Early experience in Canada. Can. Urol. Assoc. J. 2015, 9, 343–350. [Google Scholar] [CrossRef] [Green Version]
- Yeaw, J.; Benner, J.S.; Walt, J.G.; Sian, S.; Smith, D.B. Comparing adherence and persistence across 6 chronic medication classes. J. Manag. Care Pharm. 2009, 15, 728–740. [Google Scholar] [CrossRef]
- Carlson, K.; Civitarese, A.; Baverstock, R. OnabotulinumtoxinA for the treatment of idiopathic overactive bladder is effective and safe for repeated use. Can. Urol. Assoc. J. 2017, 11, e179–e183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoag, N.; Plagakis, S.; Pillay, S.; Edwards, A.W.; Gani, J. Sacral neuromodulation for refractory overactive bladder after prior intravesical onabotulinumtoxinA treatment. Neurourol. Urodyn. 2017, 36, 1377–1381. [Google Scholar] [CrossRef] [PubMed]
- Martins-Silva, C.; Cruz, F. Efficacy and safety of OnabotulinumtoxinA in patients with urinary incontinence due to neurogenic detrusor overactivity: Update of the pivotal randomised, double-blind, placebo-controlled trials. Eur. Urol. Focus 2016, 2, 329–331. [Google Scholar] [CrossRef]
- Banakhar, M.A.; Al-Shaiji, T.; Hassouna, M. Sacral neuromodulation and refractory overactive bladder: An emerging tool for an old problem. Ther. Adv. Urol. 2012, 4, 179–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, S.W.; Catanzaro, F.; Dijkema, H.E.; Elhilali, M.M.; Fowler, C.J.; Gajewski, J.B.; Hassouna, M.M.; Janknegt, R.A.; Jonas, U.; van Kerrebroeck, P.E.; et al. Long-term results of a multicenter study on sacral nerve stimulation for treatment of urinary urge incontinence, urgency-frequency, and retention. Urology 2000, 56, 87–91. [Google Scholar] [CrossRef]
- S Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year [ref.] | Trial Registration | Study Design | Participants | Exclusion Criteria | Group Sample | Follow-up (month) | Outcomes |
|---|---|---|---|---|---|---|---|
| OnabotulinumtoxinA vs. placebo | |||||||
| 2007 Sahai [7] | ISRCTN 16995641 | Randomized, Double blinded | OAB symptoms > 6 months, refractory or intolerant to medication | Neurological disease, BOO, anticoagulant therapy, pregnancy, IC, indwelling catheter, PVR >200 mL, previous bladder surgery, UC, UTI, neuromuscular transmission disease | Cystoscopy injection OnabotulinumtoxinA 200U (n = 16) vs. Cystoscopy Injection with Placebo (n = 18) | 6 | Change in MMC, Urgency, UUI, urinary frequency/day, IIQ-7, UDI-6, MBC, PVR, UTI, CIC |
| 2009 Flynn [8] | N/A | Randomized, Double blinded | OAB symptoms with UUI, refractory to medication, multiple daily incontinence and pad weight/day > 100 gm | Neurological condition, fecal incontinence or absent detrusor contraction | Cystoscopy injection OnabotulinumtoxinA 200 U/ 300 U n = 15) vs. Cystoscopy injection with Placebo (n = 7) | 1.5 | Incontinence, urinary frequency/ day, nocturia/ IIQ7, UDI6, pads/day, pads weight/ day, MBC, PVR, UTI, CIC |
| 2010 Dmochowski [9] | N/A | Randomized, Double blinded | OAB symptoms with UUI > 6 months, refractory or intolerant to medication | CIC, pelvic/urological abnormalities, disease related bladder dysfunction | OnabotulinumtoxinA 50 U/100 U/150 U/200 U/300 U (n = 268) vs. Cystoscopy injection with Placebo (n = 43) | 9 | UUI, KHQ, UTI, CIC, PVR >200 mL, urine retention |
| 2011 Rovner [10] | N/A | Randomized, Double blinded | OAB symptoms with UUI, refractory or intolerant to medication | Predominant SUI, pelvic or urologic abnormality or disease affect bladder function, frequent UTI, PVR >200, or VV >3000 | OnabotulinumtoxinA 50 U/100 U/150 U/200 U/300 U (n = 268) vs. Placebo (n = 43) | 9 | UUI, urinary frequency/day, Voided volume, MBC, CIC, PVR >200 mL |
| 2012 Denys [11] | NCT 00231491 | Randomized, Double blinded | OAB syndrome and Detrusor overactivity (≥3 urgency/ 3 days, frequency), refractory or intolerant to medication | UTI, predominant SUI, PVR >150, Qmax <15, anticoagulation/ antineoplastic or exposed to OnabotulinumtoxinA | OnabotulinumtoxinA 50 U/100 U/150 U (n = 70) vs. placebo (n = 29) | 6 | Urgency, UUI, urinary frequency, pads/day, MBC, PVR > 50% reduction, > 75% reduction UIE, EQ-5D, IQoL, UTI, CIC |
| 2012 Tincello [12] | ISRCTN 26091555 | Randomized, Double blinded | OAB symptoms and Detrusor overactivity (frequency, ≥2 urgency /day), refractory or intolerant to medication | SUI, neurologic disease, voiding dysfunction or contraindicated to OnabotulinumtoxinA | OnabotulinumtoxinA 200 U (n = 122) vs. placebo (n = 118) | 3 | Incontinence, urgency, urinary frequency/day, IQoL, UTI, CIC |
| 2013 Chapple [13] | NCT 00910520 | Randomized, Double blinded | OAB syndrome with UUI, refractory or intolerant to medication in the past 12 months | Previous OnabotulinumtoxinA treatment, with neurologic reason, predominance of SUI and pelvic/ urologic abnormalities, bladder surgery or disease affect bladder function | OnabotulinumtoxinA 100 U (n = 277) vs. placebo (n = 271) | 6 | Incontinence, urgency, UUI, urinary frequency/day, nocturia, continent, PVR, > 50% reduction UIE, ICIQ-SF, IUSS, IQoL, UTI, CIC, |
| 2011 Dowson [14] | ISRCTN 57577615 | Randomized, Double blinded | Bladder oversensitivity, refractory or intolerant to medication | Pregnancy, breast feeding, IC, neurological condition, BOO, indwelling catheter, previous bladder surgery, previous OnabotulinumtoxinA treatment, anticoagulation agent use | OnabotulinumtoxinA 100 U (n = 10) vs. placebo (n = 11) | 3 | Urinary frequency/day, Urgency, UUI, IIQ-7, UDI-6, PPBC, MBC, UTI, CIC |
| 2013 Nitti [15] | NCT 00910845 | Randomized, Double blinded | OAB syndrome, refractory or intolerant to medication | Predominance of SUI | OnabotulinumtoxinA 100 U (n = 278) vs. placebo (n = 272) | 3 | Incontinence, urgency, urinary frequency/day, nocturia, PVR, UUI, I-QoL, KHQ, UTI, CIC |
| OnabotulinumtoxinA vs. PTNS | |||||||
| 2017 Sherif [16] | N/A | Randomized | OAB symptoms, refractory or intolerant to medication | Nerve damage, pregnant, pacemaker, defibrillator, UTI, coagulopathy, BOO, neurogenic bladder, previous RT or bladder cancer, s/p incontinence surgery | OnabotulinumtoxinA 100 U (n = 30) vs. PTNS (n = 30) | 9 | Incontinence, urgency, urinary frequency/day, nocturia, OABSS, QoL, frequency, nocturia, PVR, Urgency scale, MBC, UTI, CIC |
| PTNS vs. placebo | |||||||
| 2010 Finazzi-Agro [17] | N/A | Randomized, Double blinded | female, UI with detrusor overactivity incontinence, refractory or intolerant to medication | Pregnancy or plan / UTI, fistula, stone, Interstitial cystitis, DM, pacemaker/ defibrillator | PTNS (n = 17) vs. placebo (n = 15) | 3 | Incontinence, urinary frequency/day, nocturia, >50% reduction UIE |
| 2010 Peters [18] | N/A | Randomized, Double blinded | OAB syndrome (OAB-q ≥4, voiding ≥10/day), refractory or intolerant to medication | Pregnant or plan/ neurogenic bladder/ previous use of OnabotulinumtoxinA / pacemaker/ defibrillator/ UTI/ use of TENS | PTNS (n = 103) vs. placebo (n = 105) | 3 | urinary frequency/day, nocturia, OAB-qSF, SF-36, GRA, voiding volume, UUI |
| 2016 Scaldazza [19] | N/A | Randomized | Female with OAB syndrome | SUI, UTI, neurological disease, bladder stone, POP, pregnancy, DM, anti-incontinence surgery, pelvic tumor, radiation | PTNS (n = 30) vs. placebo (n = 30) | 3 | urinary frequency/day, voiding volume, nocturia, OAB-qSF, PPIUS, PGI-I >50% reduction UIE |
| SNM vs. Placebo | |||||||
| 1999 Schmidt [20] | N/A | Randomized | UUI, poor response to anti-cholinergic agents | Neurological condition, SUI, pelvic pain symptoms | SNM (n = 34) vs. delay SNM (n = 42) | 6 | Incontinence, pads/day, >50% reduction UIE, SF-36, implant revision |
| 2000 Hassouna [21] | N/A | Randomized | Urgency/ frequency symptoms, refractory to medication | Neurological condition, SUI, pelvic pain symptoms | SNM (n = 25) vs. no SNM (n = 26) | 6 | Urinary frequency/day, MBC, >50% reduction UIE, implant revision, SF-36 |
| 2000 Weil [22] | N/A | Randomized | Refractory urinary urge incontinence | SUI, SCI, CVA within 6 months, DD, bleeding complication, VUR or hydronephrosis, UTI, pelvic pain | SNM (n = 22) vs. conservative treatment (n = 20) | 6 | Incontinence, pad use, implant revision rate, >50% reduction UIE |
| SNM vs. OnabotulinumtoxinA | |||||||
| 2016 Amundsen [23,24] | NCT 01502956 | Randomized | UUI, refractory or intolerant to 1st and 2nd line therapy | Neurological disease, PVR >150 | SNM (n = 174) vs. OnabotulinumtoxinA 200U (n = 190) | 24 | UUI, urinary incontinence, pads, nocturia urinary frequency/day, CIC, UTI, > 50% reduction UIE, Questionnaire SF, Satisfaction Questionnaire, PGI-I, Sandvik |
| Endpoint | Comparison | N | I2 (%) | p Value | Standard Mean Difference (95% CI) |
|---|---|---|---|---|---|
| Urinary frequency/ day | OnabotulinumtoxinA vs. Placebo | 4 | 92 | < 0.001 | −0.65 (-0.24–−1.06) |
| PTNS vs. OnabotulinumtoxinA | 1 | −1.02 (−1.55–−0.48) | |||
| PTNS vs. Placebo | 3 | 37.1 | 0.204 | −0.37 (-0.03–−0.70) | |
| SNM vs. Placebo | 1 | −1.12 (-0.53–−1.71) | |||
| Urge urine incontinence | OnabotulinumtoxinA vs. Placebo | 2 | 70.7 | 0.065 | −0.37 (−0.05–-0.79) |
| Urgency Episode | OnabotulinumtoxinA vs. Placebo | 4 | 97.6 | <0.001 | −0.84 (-0.08–-1.60) |
| Maximal | PTNS vs. Placebo | 1 | 1.35 (0.79–1.92) | ||
| SNM vs. Placebo | 1 | 0.91 (0.33–1.48) | |||
| I-QoL | OnabotulinumtoxinA vs. Placebo | 2 | 99.1 | <0.001 | 0.98 (−0.89–2.86) |
| PTNS vs. Placebo | 1 | 0.86 (0.13–1.59) | |||
| Incontinence | OnabotulinumtoxinA vs. Placebo | 3 | 97.8 | <0.001 | -0.84 (-1.62–-0.06) |
| PTNS vs. OnabotulinumtoxinA | 1 | 0.54 (0.02–1.06) | |||
| PTNS vs. Placebo | 1 | -1.49 (-2.28–-0.70) | |||
| SNM vs. Placebo | 2 | 74.6 | 0.047 | -2.10 (-3.07–-1.12) | |
| ≥50% Improvement | Placebo vs. OnabotulinumtoxinA | 2 | 0.0 | 0.410 | 0.53 (0.40–0.70) |
| PTNS vs. OnabotulinumtoxinA | 2 | 0.0 | 0.371 | 0.50 (0.32–0.76) | |
| Placebo vs. PTNS | 3 | 52.5 | 0.122 | 0.21 (0.07–0.61) | |
| SNM vs. Placebo | 1 | 1.27 (0.87–1.87) | |||
| Urinary tract infection | OnabotulinumtoxinA vs. Placebo | 8 | 0 | 0.486 | 2.55 (1.89–3.43) |
| PTNS vs. OnabotulinumtoxinA | 1 | 0.20 (0.01–4.34) | |||
| SNM vs. OnabotulinumtoxinA | 1 | 0.33 (0.19–0.56) | |||
| Clean intermittent catherization | OnabotulinumtoxinA vs. Placebo | 9 | 0 | 0.786 | 5.95 (3.08–11.46) |
| PTNS vs. OnabotulinumtoxinA | 1 | 0.20 (0.01–4.34) | |||
| SNM vs. OnabotulinumtoxinA | 1 | 0.01 (0.00–0.23) |
| Placebo | OnabotulinumtoxinA | PTNS | SNM | |
|---|---|---|---|---|
| Urinary frequency/ Day (SMD, 95% CI) | ||||
| Placebo | 0 | −0.65 (-0.24–-1.06) | −0.37 (-0.03–-0.70) | −1.12 (-0.53–-1.71) |
| OnabotulinumtoxinA | −1.72 (-1.23–-2.21) | 0 | −1.02 (−1.55–−0.48) | |
| PTNS | −0.80 (-0.15–-1.14) | −0.92 (−1.59–−0.26) | 0 | |
| SNM | −8.10 (-4.04–-12.16) | −6.38 (-2.29–-10.47) | −7.30 (−3.19–-11.41) | 0 |
| Incontinence/ Day (SMD, 95% CI) | ||||
| Placebo | 0 | −0.84 (−0.06–1.62) | −1.49 (−0.70–2.28) | −2.10 (-1.12–3.07) |
| OnabotulinumtoxinA | −1.96 (-0.92–-3.00) | 0 | −0.54 (-0.03–-1.06) | |
| PTNS | −2.05 (-0.56–-3.53) | -0.08 (−1.37–1.53) | 0 | |
| SNM | -10.96 (-8.60–-13.31) | −8.99 (−6.42–-11.57) | −8.91 (-6.12–-11.70) | 0 |
| Urinary tract infection (OR, 95% CI) | ||||
| Placebo | 1 | 2.54 (1.89–3.44) | ||
| OnabotulinumtoxinA | 3.06 (2.26–4.15) | 1 | 0.20 (0.01–4.35) | 0.33 (0.19–0.56) |
| PTNS | 0.57 (0.03–12.62) | 0.19 (0.01–4.06) | 1 | |
| SNM | 10.73 (0.39–1.38) | 0.24 (0.14–0.42) | 1.28 (0.06–29.29) | 1 |
| Clean intermittent catheterization (OR, 95% CI) | ||||
| Placebo | 1 | 5.95 (3.08–11.46) | ||
| OnabotulinumtoxinA | 6.92 (3.18–15.06) | 1 | 0.20 (0.01–4.34) | 0.01 (0.00–0.23) |
| PTNS | 1.29 (0.05–31.93) | 0.19 (0.01–4.19) | 1 | |
| SNM | 0.08 (0.00–1.46) | 0.01 (0.00–0.19) | 0.06 (0.00–4.01) | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo, C.-W.; Wu, M.-Y.; Yang, S.S.-D.; Jaw, F.-S.; Chang, S.-J. Comparing the Efficacy of OnabotulinumtoxinA, Sacral Neuromodulation, and Peripheral Tibial Nerve Stimulation as Third Line Treatment for the Management of Overactive Bladder Symptoms in Adults: Systematic Review and Network Meta-Analysis. Toxins 2020, 12, 128. https://doi.org/10.3390/toxins12020128
Lo C-W, Wu M-Y, Yang SS-D, Jaw F-S, Chang S-J. Comparing the Efficacy of OnabotulinumtoxinA, Sacral Neuromodulation, and Peripheral Tibial Nerve Stimulation as Third Line Treatment for the Management of Overactive Bladder Symptoms in Adults: Systematic Review and Network Meta-Analysis. Toxins. 2020; 12(2):128. https://doi.org/10.3390/toxins12020128
Chicago/Turabian StyleLo, Chi-Wen, Mei-Yi Wu, Stephen Shei-Dei Yang, Fu-Shan Jaw, and Shang-Jen Chang. 2020. "Comparing the Efficacy of OnabotulinumtoxinA, Sacral Neuromodulation, and Peripheral Tibial Nerve Stimulation as Third Line Treatment for the Management of Overactive Bladder Symptoms in Adults: Systematic Review and Network Meta-Analysis" Toxins 12, no. 2: 128. https://doi.org/10.3390/toxins12020128