Exploring Plant-Based Ethnomedicine and Quantitative Ethnopharmacology: Medicinal Plants Utilized by the Population of Jasrota Hill in Western Himalaya

 , , , and
, , , and 
Abstract
:1. Introduction
2. Material and Methods
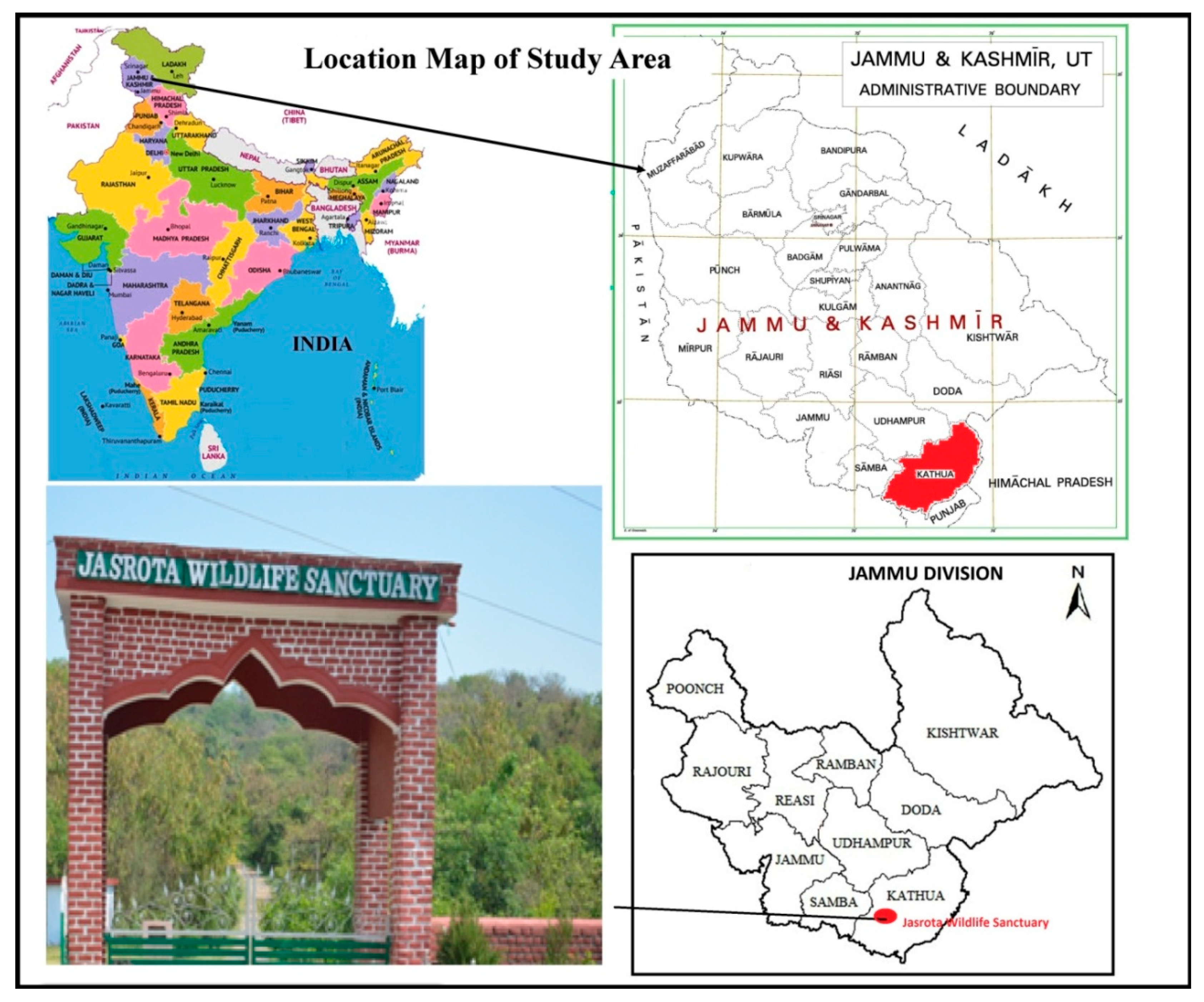
2.1. Study Area and the Local Populace
2.2. Data Collection
2.2.1. Field Surveys
2.2.2. Ethnobotanical Data Collection
Sampling Design and Methods
Informants and Interviews with Local People
2.2.3. Ailment Categories
2.3. Data Analysis
2.3.1. Informant Consensus Factor (ICF)
2.3.2. Literature Reviews
Species Identity and Library Consultation
Electronic Databases
3. Results and Discussion
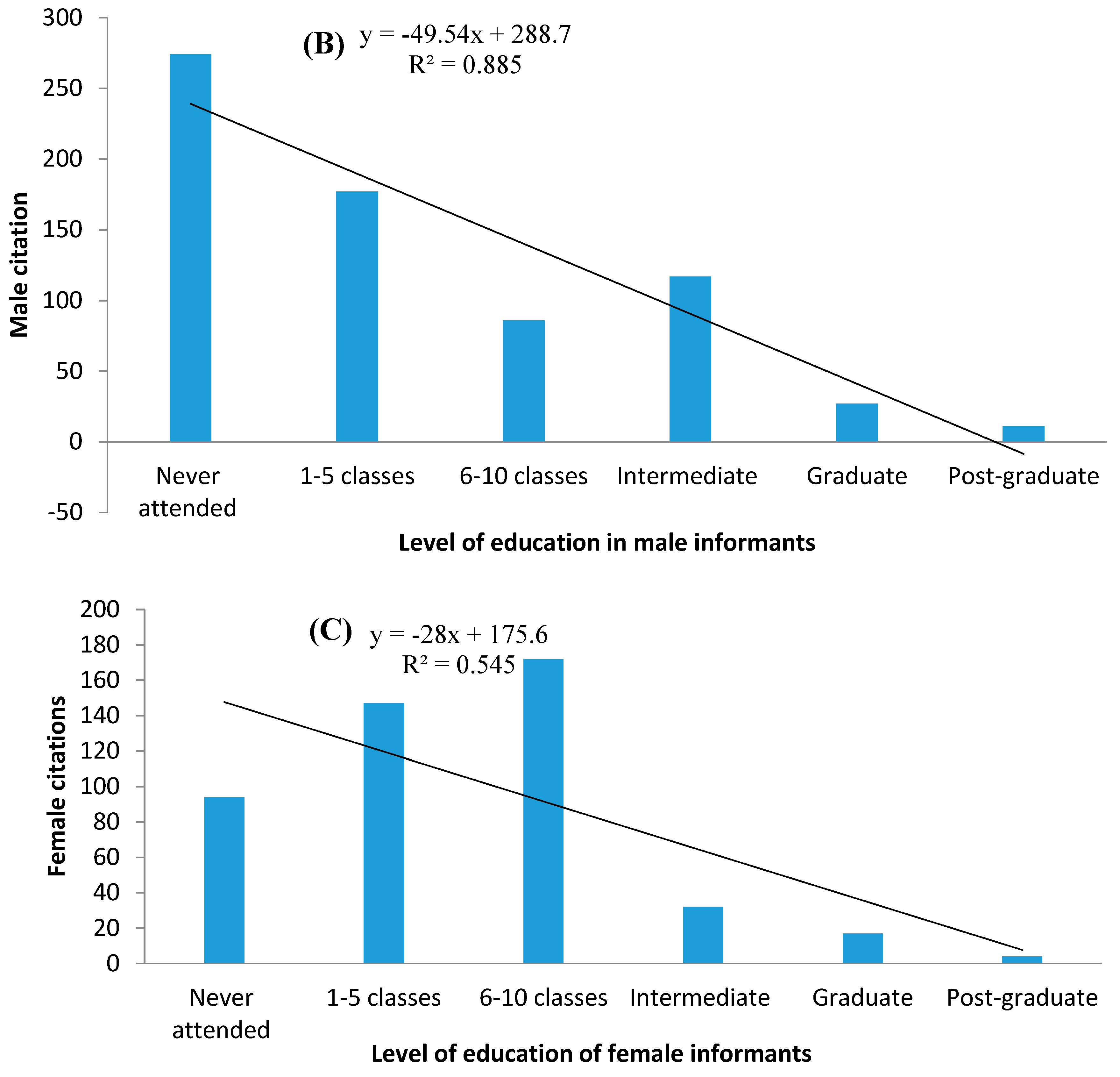
3.1. Characteristics of Informants
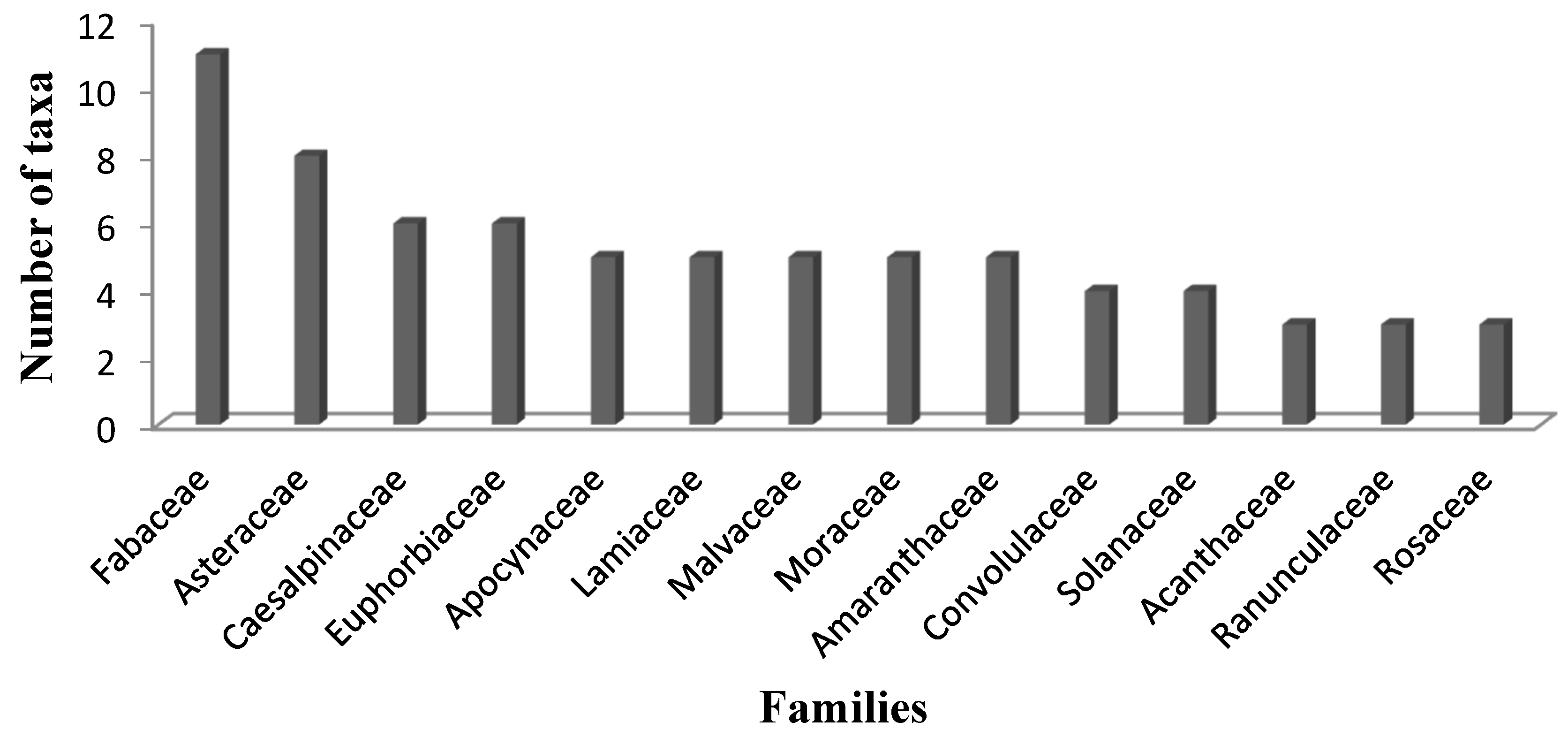
3.2. Floristic Analysis Offamilies of Medicinal Plants
3.3. Medicinal Plant Species, Use-Reports (UR), and Associated Knowledge
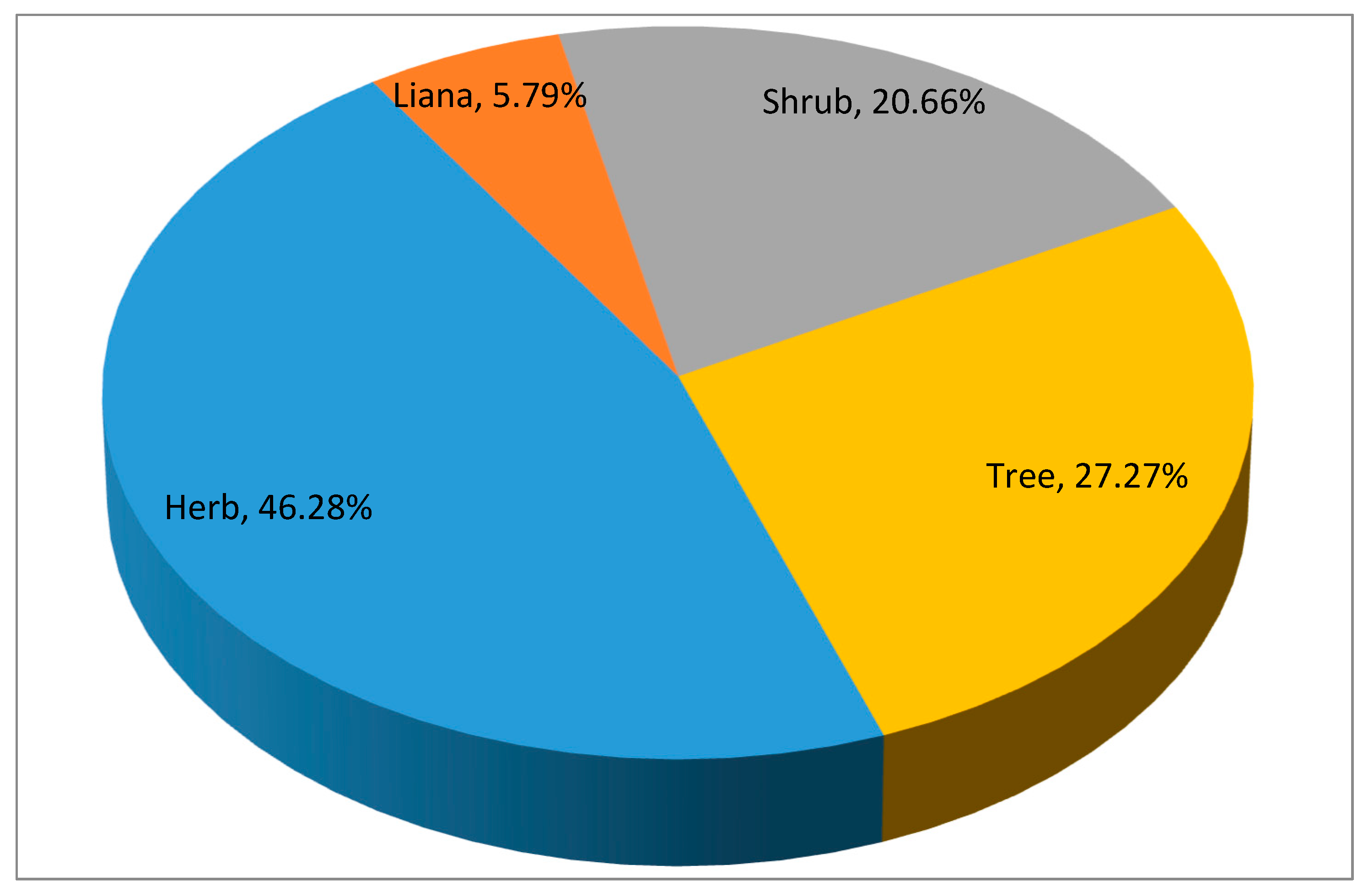
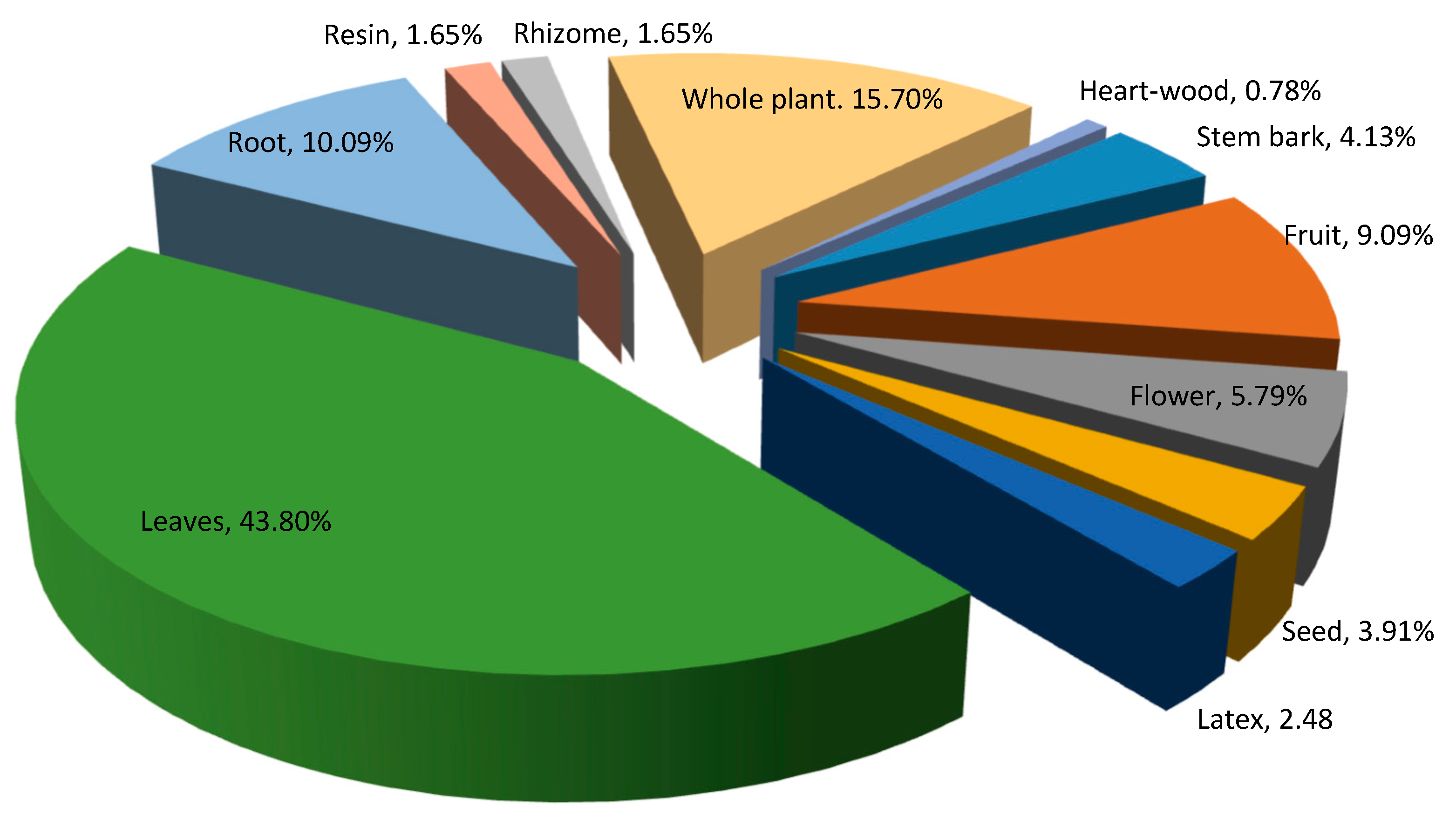
3.4. Life-Form and Plants Parts Used for Medicinal Value
3.5. Herbal Remedies and Ingredients Added
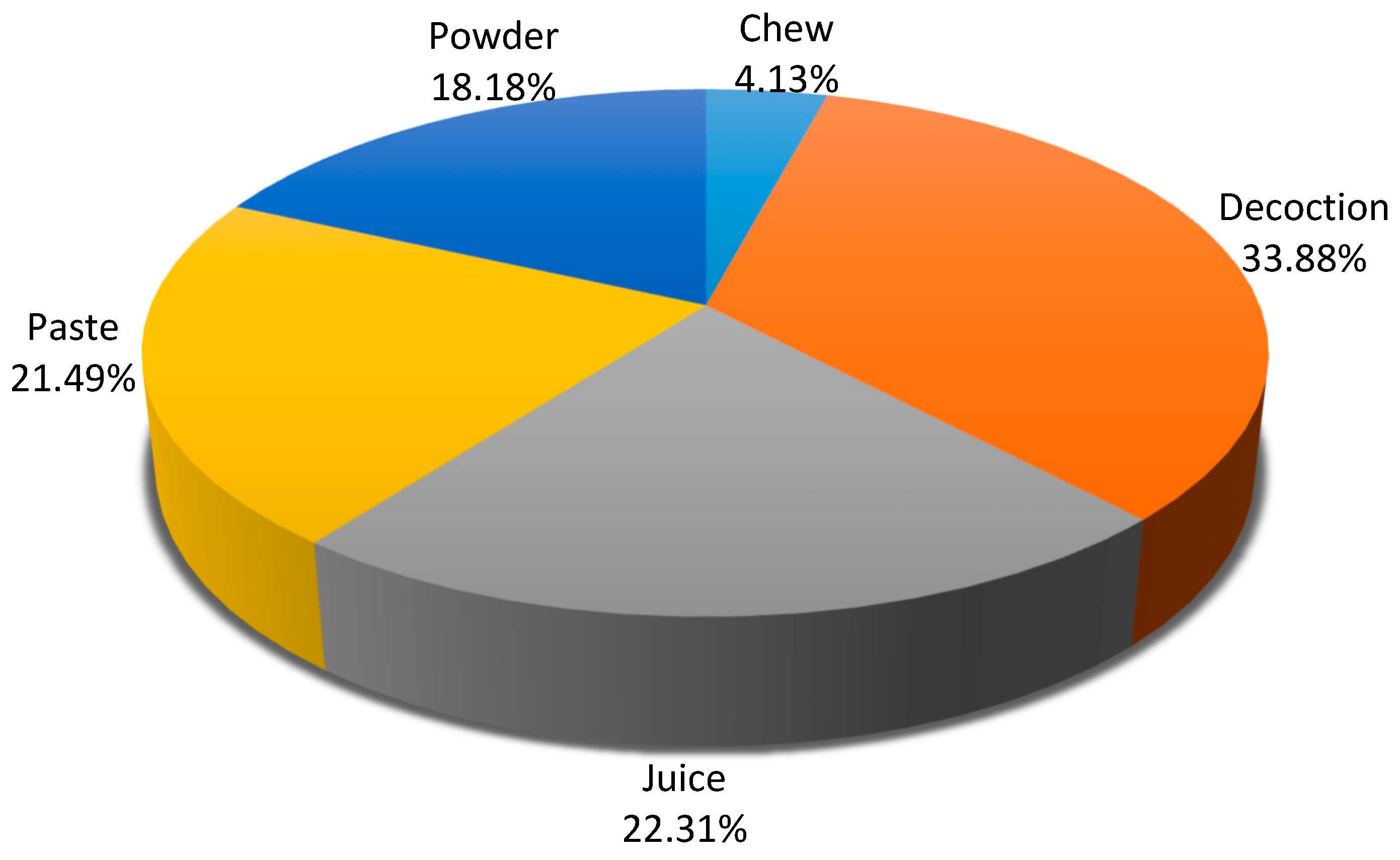
3.6. Preparation and Mode of Administration
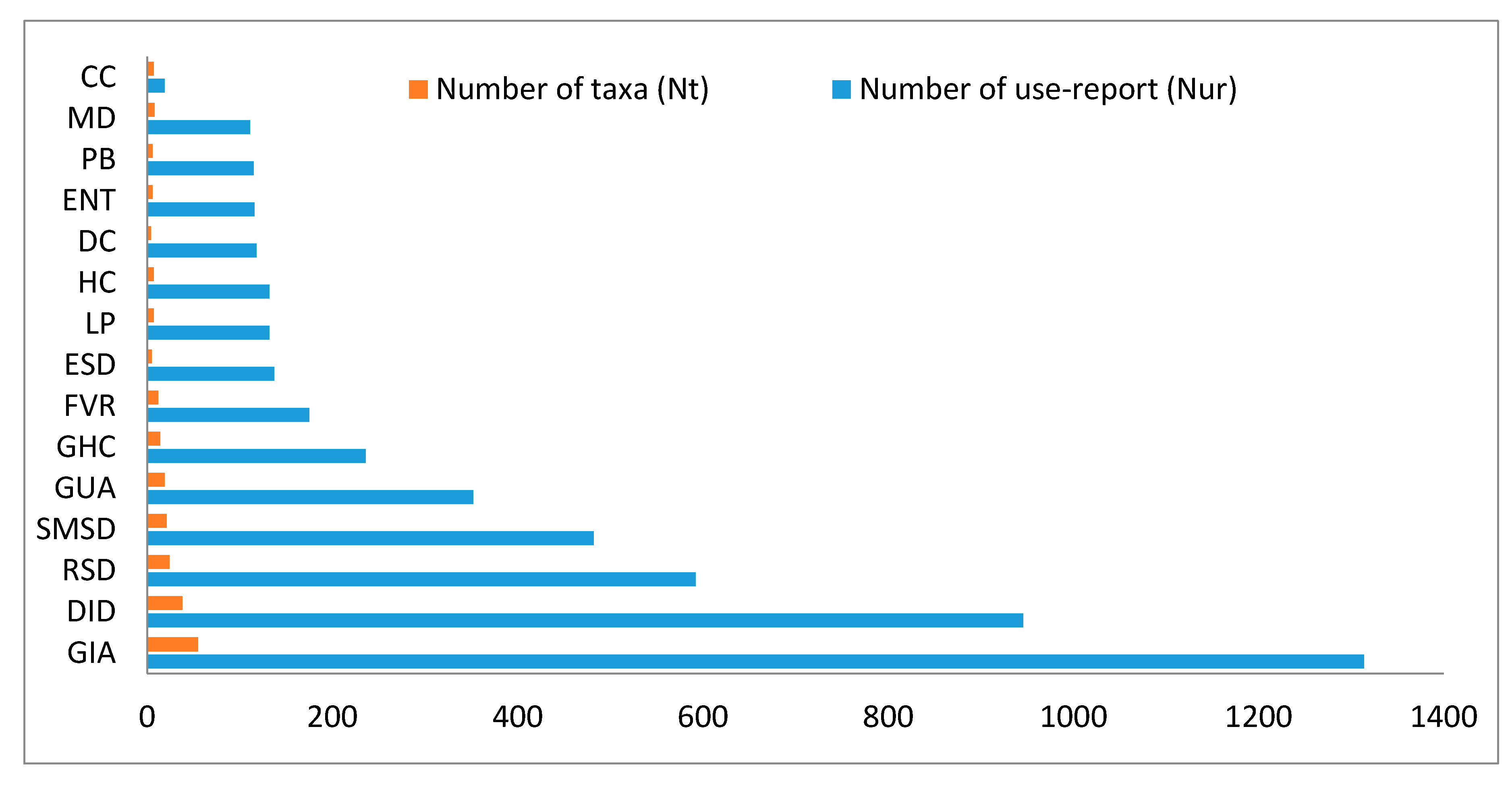
3.7. Informants Consensus factor (ICF) and Ailment Category
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Singh, B. Plants for Human Survival and Medicine; CRC Press: Boca Raton, FL, USA; Taylor & Francis: London, UK; New York, NY, USA; New India Publishing Agency: New Delhi, India, 2019; 524p. [Google Scholar]
- Ortiz, A.C.; Musarella, C.M.; Gomes, C.J.P.; Canas, R.Q.; Fuentes, J.C.P.; Cano, E. Phytosociological study, diversity and conservation status of the Cloud Forest in the Dominican Republic. Plants 2020, 9, 741. [Google Scholar] [CrossRef]
- Colalto, C. What phytotherapy needs: Evidence-based guidelines for better clinical practice. Phytother. Res. 2018. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Singh, A.; Singh, B.; Maurya, R.; Kumar, B. Structural characterization and quantitative determination of bioactive compounds in ethanolic extraction of Boerhaavia diffusa by liquid chromatography-tandem mass spectrometry. J. Sep. Sci. Plus. 2018. [Google Scholar] [CrossRef]
- Sidigia, I.; Nyaigotti-Chacha, C.; Kanunah, M.P. Traditional Medicine in Africa; East African Educational Publishers: Nairobi, Kenya, 1990. [Google Scholar]
- Sharma, Y.P.; Singh, B. Human-plant Relations and Future Drug Discovery; New India Publishing Agency: New Delhi, India, 2020; 392p. [Google Scholar]
- Thakur, S.; Tashi, N.; Singh, B.; Dutta, H.C.; Singh, B. Ethnobotanical plants used for gastrointestinal ailments by the inhabitants of Kishtwar plateau in Northwestern Himalaya, India. Indian J. Tradit. Knowle. 2020, 19, 1–11. [Google Scholar]
- Dubey, N.K.; Kumar, R.; Tripathi, P. Global promotion of herbal medicine: India’s opportunity. Curr. Sci. 2004, 86, 37–41. [Google Scholar]
- Balunas, M.J.; Kinghorn, A.D. Drug discovery from medicinal plants. Life Sci. J. 2005, 78, 431–441. [Google Scholar] [CrossRef]
- Baig, B.A.; Ramamoorthy, D.; Bhat, T.A. Threatened medicinal plants of Menwarsar Pahalgam, Kashmir Himalayas: Distribution pattern and current conservation status. Proc. Int. Acad. Ecol. Environ. Sci. 2013, 3, 25–35. [Google Scholar]
- Fabricant, D.S.; Farnsworth, N.R. The value of plants used in traditional medicine for drug discovery. Environ. Health Perspect. 2001, 109, 69–75. [Google Scholar]
- Ahmad, L.; Semotiuk, A.; Zafar, M.; Ahmad, M.; Sultana, S.; Liu, Q.; Zada, M.P.; Abidin, S.Z.U.; Yaseen, G. Ethnopharmacological documentation of medicinal plants used for hypertension among the local communities of DIR Lower Pakistan. J. Ethnopharmacol. 2015, 175, 138–146. [Google Scholar] [CrossRef]
- Maruca, G.; Spampinato, G.; Turiano, D.; Laghetti, G.; Musarella, C.M. Ethnobotanical notes about medicinal and useful plants of the Reventino Massif tradition (Calabria region, Southern Italy). Genet. Resour. Crop Evol. 2019, 66, 1027–1040. [Google Scholar] [CrossRef]
- Amini, A. Illustrated Dictionary of Therapeutic Plants and Their Traditional Usage in Kurdistan; Taqbostan Publication: Khoramabad, Iran, 1997. [Google Scholar]
- Tabuti, J.R.S.; Lye, K.A.; Dhillion, S.S. Traditional herbal drugs of Bulamogi, Uganda: Plants, use and administration. J. Ethnopharmacol. 2003, 88, 19–44. [Google Scholar] [CrossRef]
- Musarella, C.M.; Paglianiti, I.; Spampinato, G. Ethnobotanical study in the Poro and Preserre Calabresi territory (Vibo Valentia, S-Italy). Atti. Soc. Tosc. Sci. Nat. Mem. Serie. B 2019. [Google Scholar] [CrossRef]
- Bunalema, L.; Obakiro, S.; Tabuti, J.R.S.; Waako, P. Knowledge on plants used traditionally in the treatment of tuberculosis in Uganda. J. Ethnopharmacol. 2014, 151, 999–1004. [Google Scholar] [CrossRef] [PubMed]
- Spampinato, G.; Musarella, C.M.; Cano-Ortiz, A.; Signorino, G. Habitat, occurrence and conservation status of the Saharo-Macaronesian and Southern-Mediterranean element Fagonia cretica L. (Zygophyllaceae) in Italy. J. Arid Land 2018, 10, 140–151. [Google Scholar] [CrossRef] [Green Version]
- Singh, B. Plants of Commercial Value; CRC Press: Boca Raton, FL, USA; Taylor & Francis: London, UK; New York, NY, USA; New India Publishing Agency: New Delhi, India, 2019. [Google Scholar]
- Ignacimuthu, S.; Sankarasivaraman, K.; Kesavan, L. Medico-ethnobotanical survey among Kanikar Tribals of Mundanthurai Sanctuary. Fitoterapia 1998, 69, 409–414. [Google Scholar]
- Mukherjee, P.K.; Maiti, K.; Mukherjee, K.; Houghton, P.J. Leads from Indian medicinal plants with hypoglycemic potentials. J. Ethnopharmocol. 2006, 106, 1–28. [Google Scholar] [CrossRef]
- Rates, S.M.K. Plants as source of drugs. Toxicon 2001, 39, 603–613. [Google Scholar] [CrossRef]
- Singh, B. Himalayan Orchid, Diversity and Taxonomy; Write and Print Publication: New Delhi, India, 2015; 225p. [Google Scholar]
- Singh, B.; Singh, B.; Borthakur, S.K.; Phukan, S.J. Contribution to biodiversity hotspot: Assessment of forest types, floristic composition and economic wealth of Nokrek biosphere reserve in Northeast India. Indian Forest. 2018, 144, 734–741. [Google Scholar]
- Singh, B.; Singh, S.; Singh, B.; Kitchlu, S.; Babu, V. Assessing ethnic traditional knowledge, biology and chemistry of Lepidium didymum L., lesser-known wild plants of Western Himalaya. Proc. Natl. Acad. Sci. India Sec. B. Biol. Sci. 2019, 89, 1087–1094. [Google Scholar] [CrossRef]
- Kumar, R.; Bhagat, N. Ethnomedicinal plants of district Kathua, J&K. Int. J. Med. Aromat. Plants 2012, 2, 603–611. [Google Scholar]
- Kaul, M.K.; Sharma, P.K.; Singh, V. Ethnobotanical studies in North-West and Trans Himalaya. J. Health Sci. 1990, 16, 81–87. [Google Scholar]
- Virjee, D.; Kachroo, G.H.; Bhat, G.M.P. Taxo-ethnobotanical studies of the rural areas in the Rajouri district, Jammu. J. Econ. Taxon. Bot. 1984, 5, 831–838. [Google Scholar]
- Bhushan, B.; Kumar, M. Ethnobotanically important medicinal plants of Tehsil Billawar, District Kathua, JandK, India. J. Pharmacogn. Phytochem. 2013, 2, 14–21. [Google Scholar]
- Nawchoo, I.A.; Buth, G.M. Medicinal system of Ladakh, India. J. Ethnopharmocol. 1989, 20, 137–146. [Google Scholar]
- Visvanath, M.V.; Mankad, N.R. Medicinal plants of Ladakh (J&K). J. Econ. Taxon. Bot. 1984, 5, 401–407. [Google Scholar]
- Siddique, M.A.A.; Jhon, A.Q.; Paul, T.M. Status of important medicinal plants of Kashmir Himalayas. Adv. Plant Sci. 1995, 8, 134–139. [Google Scholar]
- Tantray, M.A.; Tariq, K.A.; Mir, M.M.; Bhat, M.A.; Shawl, A.S. Ethnomedicinal survey of Shopian, Kashmir (J and K), India. Asian J. Tradit. Med. 2009, 4, 1–6. [Google Scholar]
- Singh, B.; Sultan, P.; Hassan, Q.P.; Gairola, S.; Bedi, Y.S. Ethnobotany traditional knowledge, and diversity of wild edible plants and fungi: A case study in the Bandipora district of Kashmir Himalaya, India. J. Herbs Spices Med. Plant 2016, 22, 247–278. [Google Scholar] [CrossRef]
- Singh, B.; Bedi, Y.S. Eating from raw wild plants in Himalaya: Traditional knowledge documentary on Sheena tribes along LoC border in Kashmir. Indian J. Nat. Prod. Resour. 2017, 8, 269–275. [Google Scholar]
- Singh, B.; Borthakur, S.K.; Phukan, S.J. A survey of ethnomedicinal plants utilized by the indigenous people of Garo hills with special reference to the Nokrek biosphere reserve (Meghalaya), India. J. Herbs Spices Med. Plant 2014, 20, 1–30. [Google Scholar] [CrossRef]
- Singh, B.; Sinha, B.K.; Phukan, S.J.; Borthakur, S.K.; Singh, V.N. Wild edible plants used by Garo tribes of Nokrek biosphere reserve in Meghalaya, India. Indian J. Tradit. Knowle. 2012, 11, 166–171. [Google Scholar]
- Asase, A.; Akwetey, G.A.; Achel, D.G. Ethnopharmacological use of herbal remedies for the treatment of malaria in the Dangme West District of Ghana. J. Ethnopharmocol. 2010, 129, 367–376. [Google Scholar] [CrossRef]
- Singh, B. Botanical Leads for Drug Discovery; Springer Nature, Singapore Pte Ltd.: Singapore, 2020. [Google Scholar] [CrossRef]
- Ashutosh, S.; Pandey, S.; Kaur, T.; Bajpai, R.K. Knowledge based remote sensing and GIS approach for forest type mapping in Kathua district, Jammu and Kashmir. Trop. Ecol. 2010, 51, 21–29. [Google Scholar]
- Rao, P.K.; Hasan, S.S.; Bhellum, B.L.; Manhas, R.K. Ethnomedicinal plants of Kathua district, J&K, India. J. Ethnopharmacol. 2015, 171, 12–27. [Google Scholar] [CrossRef] [PubMed]
- Bhat, T.A.; Nigam, G.; Majaz, M. Study of some medicinal plants of the Shopian District, Kashmir (India) with emphasis on their traditional use by Gujjar and Bakerwal tribes. Asian J. Pharm. Clin. Res. 2012, 5, 94–98. [Google Scholar]
- Jain, S.K.; Rao, R.R. A Handbook of Field and Herbarium Methods; Today and Tomorrow’s Printer: New Delhi, India, 1977; 157p. [Google Scholar]
- Thiers, B. Index Herbariorum: A Global Directory of Public Herbaria and Associated Staff. New York Botanical Garden’s Virtual Herbarium. 2020. Available online: http://sweetgum.nybg.org/science/ih (accessed on 10 September 2020).
- Heinrich, M. Ethnobotany and its role in drug development. Phytotherap. Res. 2000, 14, 479–488. [Google Scholar] [CrossRef]
- Weckerle, C.S.; Boer, H.J.D.; Puri, R.K.; Andel, T.V.; Bussmann, R.W.; Leonti, M. Recommended standards for conducting and reporting ethnopharmacological field studies. J. Ethnopharmacol. 2018, 210, 125–132. [Google Scholar] [CrossRef]
- Bolfarine, H.; Bussab, W.O. Elementos de Amostragem; Edgar Blucher: Sao Paulo, Brazil, 2005. [Google Scholar]
- Scheaffer, R.L.; Mendenhall, W.; Ott, L. Elementary Survey Sampling; Thomson: Belmont, TN, USA, 2006. [Google Scholar]
- Espinosa, M.M.; Bieski, I.; Martins, D.T.D.O. Probability sampling design in ethnobotanical surveys of medicinal plants. Rev. Bras. Farmacogn. 2014, 22, 1362–1367. [Google Scholar] [CrossRef] [Green Version]
- Martin, G.J. Ethnobotany, a Method Manual WWF for Nature International; Chapman and Hall: London, UK, 1995. [Google Scholar]
- Cotton, B.M. Ethnobotany, Principles and Applications; John Wiley and Sons, Ltd.: Chichester, UK, 1996; 424p. [Google Scholar]
- Trotter, R.; Logan, M.; Trotter, R.T.; Logan, M.H. Informant Consensus: A New Approach for Identifying Potentially Effective Medicinal Plants; Redgrave: New York, NY, USA, 1989. [Google Scholar]
- Heinrich, M.; Ankli, A.; Frei, B.; Weimann, C.; Sticher, O. Medicinal plants in Mexico: Healers’ consensus and cultural importance. Soc. Sci. Med. 1998, 47, 91–112. [Google Scholar] [CrossRef]
- Shukla, P.; Singh, B. Analysis of indigenous uses of ethnobotanical herbaceous plants and their diversity among nature-dependent communities in Atraulia of Burhanpur Tehsil, District Azamgarh, Uttar Pradesh. In Plants for Novel Drug Molecules-Ethnobotany to Ethnopharmacology; New India Publishing Agency: New Delhi, India, 2020; pp. 171–191. [Google Scholar]
- Bieski, I.G.C.; Leonti, M.; Arnason, J.T.; Ferrier, J.; Rapinski, M.; Violante, I.M.P.; Balogun, S.O.; Pereira, J.F.C.A.; Figueiredo, R.D.C.F.; Lopes, C.R.A.S.; et al. Ethnobotanical study of medicinal plants by population of Valley of Juruena Region, Legal Amazon, Mato Grosso, Brazil. J. Ethnopharmacol. 2015. [Google Scholar] [CrossRef]
- Heinrich, M.; Edwards, S.; Moerman, D.E.; Leonti, D.E. Ethnopharmacological field studies: A critical assessment of their conceptual basis and methods. J. Ethnopharmacol. 2009, 124, 1–17. [Google Scholar] [CrossRef]
- Gazzaneo, L.R.S.; Lucena, R.F.P.; Albuquerque, U.P. Knowledge and use of medicinal plants by local specialists in a region of Atlantic Forest in the state of Pernambuco (Northeastern Brazil). J. Ethnobiol. Ethnomed. 2005, 1, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, B.M.; Kachroo, P. Flora of Jammu and Plants of Neighbourhood; Bishen Singh Mahendra Pal Singh: Dehra Dun, India, 1981. [Google Scholar]
- Spearman, C. The proof and measurement of association between two things. Am. J. Psychol. 1904, 15, 72–101. [Google Scholar] [CrossRef]
- Mann, H.B.; Whitney, D.R. On a test of whether one of two random variables is stochastically larger than the other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- Kapur, S.K.; Sarin, Y.K. Flora of Trikuta Hills; Bishen Singh Mahendra Pal Singh: Dehradun, India, 1990. [Google Scholar]
- Swami, A.; Gupta, B.K. Flora of Udhampur; Bishen Singh Mahendra Pal Singh: Dehradun, India, 1998. [Google Scholar]
- Duke, J.A. Handbook of Medicinal Herbs; CRC Press: London, UK, 2002. [Google Scholar]
- Khare, C.P. Indian Medicinal Plants, an Illustrated Dictionary; Springer Science Plus Business Media LLC: New York, NY, USA, 2007; 836p. [Google Scholar]
- Sharma, B.M. Illustration of Jammu Plants; Bishen Singh Mahendra Pal Singh: Dehradun, India, 2010; 317p. [Google Scholar]
- Chopra, V.L.; Vishwakarma, R.A. Plants for Wellness and Vigour; New India Publishing Agency: New Delhi, India, 2018; 399p. [Google Scholar]
- APG III. Angiosperm Phylogeny Group, an update of the angiosperm phylogeny group classification for the orders and families of flowering plants: APG III. J. Linn. Soc. 2009, 161, 105–121. [Google Scholar] [CrossRef] [Green Version]
- APG IV. Angiosperm Phylogeny Group, an update of the angiosperm phylogeny group classification for the orders and families of flowering plants: APG IV. Bot. J. Linn. Soc. 2016, 181, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Pereira, C.; Agarez, F.V. Estudo das Plantas Ruderais do Estado do Rio de Janeiro; Leandra (UFRJ): Rio Janeiro, Brazil, 1977; Volume 7, pp. 77–93. [Google Scholar]
- Estomba, D.; Ladio, A.; Lozada, M. Medicinal wild plant knowledge and gathering patterns in Mapuche community from Northwestern Patagonia. J. Ethnopharmacol. 2006, 103, 109–119. [Google Scholar] [CrossRef]
- Yineger, H.; Yewhalaw, D.; Teketay, D. Ethnomedicinal plant knowledge and practice of the Oromo ethnic group in southwestern Ethiopia. J. Ethnobiol. Ethnomed. 2008, 4, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Jan, H.A.; Jan, S.; Bussman, L.A.; Wali, S.; Ahmad, N. Ethnomedicinal survey of the plants used for gynaecological disorders by the indigenous community of district Buner, Pakistan. Ethnobot. Res. Appl. 2020, 16, 26. [Google Scholar]
- Hudaib, M.; Mohammad, M.; Bustanji, Y.; Tayyem, R.; Yousef, M.; Abuirjeie, M.; Aburjai, T. Ethnopharmacological survey of medicinal plants in Jordan, Mujib Nature Reserve and surrounding area. J. Ethnopharmocol. 2008, 120, 63–71. [Google Scholar] [CrossRef]
- Gonzalez, J.A.; Garcia-Barrriuso, M.; Amich, F. Ethnobotanical study of medicinal plants traditionally used in the Arribes del Duero, Western Spain. J. Ethnopharmocol. 2010, 131, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Tabuti, J.R.S.; Kukunda, C.B.; Waako, P.J. Medicinal plants used by traditional medicine practitioners in the treatment of tuberculosis and related ailments in Uganda. J. Ethnopharmocol. 2010, 127, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, K.; Pieroni, A. Folk knowledge of wild food plants among the tribal communities of Thakhte-Sulaiman Hills, North-West Pakistan. J. Ethnobiol. Ethnomed. 2016, 12, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jana, J.C. Use of traditional and underutilized leafy vegetables of subhimalayan terai region of West Bengal. Acta Hortic. 2007, 752, 571–575. [Google Scholar] [CrossRef]
- Shankar, U.; Lama, S.D.; Bawa, K.S. Ecology and economics of domestication of non-timber forest products: An illustration of Broomgramin Darjeeling Himalaya. J. Trop. For. Sci. 2001, 13, 171–191. [Google Scholar]
- Thomas, B.; Mathews, R.P.; Rajendran, A.; Kumar, K.P. Ethnobotanical observations on tribe Arnatans of Nilambur Forest, Western Ghats region of Kerala, India. Res. Plant Biol. 2013, 3, 12–17. [Google Scholar]
- Shrestha, P.M.; Dhillion, S.S. Medicinal plant diversity and use in the highlands of Dolakha district, Nepal. J. Ethnopharmacol. 2003, 86, 81–96. [Google Scholar] [CrossRef]
- Emmanuel, M.M.; Didier, D.S. Medicinal plant knowledge of ethnic groups in Douala town, Cameroon. Am. J. Food Nutr. 2011, 1, 178–184. [Google Scholar] [CrossRef]
- Singh, B.; Borthakur, S.K. Wild medicinal plants used by tribal communities of Meghalaya. J. Econ. Taxon. Bot. 2011, 35, 331–339. [Google Scholar]
- Rao, A.S.; Yadav, S.S.; Singh, P.; Nandal, A.; Singh, N.; Ganaie, S.A.; Yadav, N.; Kumar, R.; Bhandoria, M.S.; Bansal, P. A comprehensive review on ethnomedicine, phytochemistry, pharmacology, and toxicity of Tephrosia purpurea (L.) Pers. Phytother. Res. 2020. [Google Scholar] [CrossRef]
- Bhatia, H.; Sharma, Y.P.; Manhas, R.K.; Kumar, K. Ethnomedicinal plants used by the villagers of district Udhampur, J&K, India. J. Ethnopharmocol. 2014, 151, 1005–1018. [Google Scholar]
- Singh, B.; Shanpru, R. Ethnobotanically important plants in Sacred Forests of Meghalaya. Ann. For. 2010, 18, 270–282. [Google Scholar]
- Ayyanar, M.; Ignacimuthu, S. Ethnobotanical survey of medicinal plants commonly used by Kani tribals in Tirunelveli hills of Western Ghats, India. J. Ethnopharmocol. 2011, 134, 851–864. [Google Scholar] [CrossRef]
- Thakur, S.; Dutt, H.C.; Singh, B.; Sharma, Y.P.; Tashi, N.; Charak, R.S.; Sharma, G.; Vidyarathi, O.P.; Iqbal, T.; Singh, B.; et al. Plant and fungi diversity of Devi Pindiyan Valley in Trikuta Hills of northwestern Himalaya, India. J. Threat. Taxa 2019, 11, 14827–14844. [Google Scholar] [CrossRef]
- Dapar, M.L.G.; Alejandro, G.J.D.A.; Meve, U.; Liede-Schumann, S. Quantitative ethnopharmacological documentation and molecular confirmation of medicinal plants used by the Manobo tribe of Agusan del Sur, Philippines. J. Ethnobiol. Ethnomed. 2020, 16, 14. [Google Scholar] [CrossRef] [Green Version]
- Morales, M.R.; Simon, J.E. New Basil Selections with Compact Inflorescence of the Ornamental Market; Progress in New Crops; Janick, J., Ed.; ASHS Press: Arlington, VA, USA, 1996; pp. 543–546. [Google Scholar]
- Uritu, C.M.; Mihai, C.T.; Stanciu, G.; Dodi, G.; Alexa-Stratulat, T.; Luca, A.; Leon-Constantin, M.; Stefanescu, R.; Bild, V.; Melnic, S.; et al. Medicinal plants of the family Lamiaceae in pain therapy: A review. Pain Res. Manag. 2018. [Google Scholar] [CrossRef] [Green Version]
- Panuccio, M.R.; Fazio, A.; Musarella, C.M.; Mendoza-Fernández, A.J.; Mota, J.F.; Spampinato, G. Seed germination and antioxidant pattern in Lavandula multifida (Lamiaceae): A comparison between core and peripheral populations. Plant Biosyst. 2018, 152, 398–406. [Google Scholar] [CrossRef]
- Pereira, Z.V.; Mussury, R.M.; de Almeida, A.B.; Sangalli, A. Medicinal plants used by Ponta Porã community, Mato Grosso do Sul State. Acta Sci. Biol. Sci. 2009, 31, 293–299. [Google Scholar] [CrossRef]
- Wink, M. Evolution of secondary metabolites in legumes (Fabaceae). S. Afr. J. Bot. 2013, 89, 164–175. [Google Scholar] [CrossRef] [Green Version]
- Bajpai, V.; Singh, A.; Singh, P.; Singh, B.; Pratap, B.; Maurya, R.; Kumar, B. Development of ultra performance liquid chromatography tandem mass spectrometry method for simultaneous identification and quantitation of potential osteogenic phytochemicals in Butea monosperma. J. Chromatogr. Sci. 2018, 56, 738–745. [Google Scholar] [CrossRef]
- Cano, E.; Musarella, C.M.; Cano-Ortiz, A.; Piñar Fuentes, J.C.; Spampinato, G.; Pinto Gomes, C.J. Morphometric analysis and bioclimatic distribution of Glebionis coronaria s.l. (Asteraceae) in the Mediterranean area. PhytoKeys 2017, 81, 103–126. [Google Scholar] [CrossRef] [PubMed]
- Cano, E.; Cano-Ortiz, A.; Musarella, C.M.; Piñar Fuentes, J.C.; Quinto Canas, R.; Spampinato, G.; Pinto Gomes, C.J. Endemic and rare species of Asteraceae from the Southern Iberian Peninsula: Ecology, distribution and syntaxonomy. In Asteraceae: Characteristics, Distribution and Ecology; Nova Science Publishers, Inc.: Hauppauge, NY, USA, 2020; pp. 147–175. ISBN 978-1-53616-632-3. [Google Scholar]
- Tardio, J.; Pardo-de-Santayan, M.; Morales, R. Ethnobotanical review of wild edible plants in Spain. Bot. J. Linn. Soc. 2006, 152, 27–71. [Google Scholar] [CrossRef]
- Singh, A.K.; Raghubansi, A.S.; Singh, J.S. Medical ethnobotany of the tribals of Sonaghati of Sonbhadra district, Uttar Pradesh, India. J. Ethnopharmacol. 2002, 81, 31–41. [Google Scholar] [CrossRef]
- Giday, M.; Asfaw, Z.; Woldu, Z. Ethnomedicinal study of plants used by Sheko ethnic group of Ethiopia. J. Ethnopharmocol. 2010, 132, 75–85. [Google Scholar] [CrossRef]
- Ayyanar, M.; Ignacimuthu, S. Traditional knowledge of Kani tribals in Kouthalai of Tirunelveli hills, Tamil Nadu, India. J. Ethnopharmocol. 2005, 102, 246–255. [Google Scholar] [CrossRef]
- Muthu, C.; Ayyanar, M.; Raja, N.; Ignacimuthu, S. Medicinal plants used by traditional healers in Kancheepuram district of Tamil Nadu, India. J. Ethnobiol. Ethnomed. 2006, 2, 43. [Google Scholar] [CrossRef] [Green Version]
- Uniyal, S.K.; Singh, K.N.; Jamwa, P.; Lal, B. Traditional use of medicinal plants among the tribal communities Chhota, Western Himalaya. J. Ethnobiol. Ethnomed. 2006, 2, 14. Available online: http://www.ethnobiomed.com/content/2/1/14 (accessed on 10 September 2020). [CrossRef] [Green Version]
- Bhatia, H.; Sharma, Y.P.; Manhas, R.K.; Kumar, K. Traditional phytoremedies for the treatment of menstrual disorders in district Udhampur, J&K, India. J. Ethnopharmacol. 2015, 160, 202–210. [Google Scholar]
- Sarin, Y.K.; Kapur, S.K. Plant resource exploitation and their utilization in Trikuta Hills of Jammu province (J&K). J. Econ. Taxon. Bot. 1984, 5, 1143–1158. [Google Scholar]
- Kumari, P.; Joshi, G.C.; Tewari, L.M. Indigenous uses of threatened ethnomedicinal plants used to cure different diseases by ethnic people of Almora district of Western Himalaya. Int. J. Ayurvedic Herb. Med. 2012, 2, 661–678. [Google Scholar]
- Kumari, S.; Batish, D.R.; Singh, H.P.; Negi, K.; Kohli, R.K. An ethnobotanical survey of medicinal plants used by Gujjar community of Trikutta hills in Jammu and Kashmir, India. J. Med. Plant Res. 2013, 7, 2111–2121. [Google Scholar]
- Teklehaymanot, T.; Giday, M.; Medhin, G.; Mekonnen, Y. Knowledge and use of medicinal plants by people around Debre Libanos monastery in Ethiopia. J. Ethnopharmocol. 2007, 111, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Giday, M.; Asfaw, Z.; Woldu, Z. Medicinal plants of the Meinit ethnic group of Ethiopia: An ethnobotanical study. J. Ethnopharmocol. 2009, 124, 513–521. [Google Scholar] [CrossRef]
- Lulekal, E.; Asfaw, Z.; Kelbessa, E.; Van Damme, P. Ethnomedicinal study of plants used for human ailments in Ankober District, North Shewa Zone, Amhara Region, Ethiopia. J. Ethnobiol. Ethnomed. 2013, 9, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adnan, M.; Ullah, I.; Tariq, A.; Murad, W.; Azizullah, A.; Khan, A.L.; Ali, N. Ethnomedicine use in the war affected region of Northwest Pakistan. J. Ethnobiol. Ethnomed. 2014, 10, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giday, M.; Asfaw, Z.; Elmqvist, T.; Woldu, Z. An ethnobotanical study of medicinal plants used by the Zay people in Ethiopia. J. Ethnopharmacol. 2003, 85, 43–52. [Google Scholar] [CrossRef]
- Lee, S.; Xiao, C.; Pei, S. Ethnobotanical survey of medicinal plants at periodic markets of Honghe Prefecture in Yunnan Province, SW China. J. Ethnopharmocol. 2008, 117, 362–377. [Google Scholar] [CrossRef] [PubMed]
- Prasad, N.P.; Singh, R.; Narayanan, L.M.; Natarajan, C.R. Ethnobotany of Kanikkars of South Tamil Nadu. J. Econ. Taxon. Bot. 1996, 12, 292–298. [Google Scholar]
- Mahishi, P.; Srinivasa, B.H.; Shivanna, M.B. Medicinal plant wealth of local communities in some villages in Shimoga District of Karnataka, India. J. Ethnopharmocol. 2005, 98, 307–312. [Google Scholar] [CrossRef]
- Perumalsamy, R.; Thwin, M.M.; Gopalkrishnakone, P.; Ignacimuthu, S. Ethnobotanical survey of folk plants for the treatment of snake bites in Southern part of Tamil nadu, India. J. Ethnopharmocol. 2008, 115, 302–312. [Google Scholar]
- Srithi, K.; Balslev, H.; Wangpakapattanawong, P.; Srisanga, P.; Trisonthi, C. Medicinal plant knowledge and its erosion among the Mien(Yao) in northern Thailand. J. Ethnopharmacol. 2009, 123, 335–342. [Google Scholar] [CrossRef]
- Gupta, R. Survey record of medicinal and aromatic plants of Chamba forestdivision, Himachal Pradesh. Indian Forest. 1964, 90, 454–463. [Google Scholar]
- Gupta, S.K.; Sharma, O.M.P.; Raina, N.S.; Sehgal, S. Ethnobotanical study of medicinal plants of Paddar valley of Jammu and Kashmir, India. Afr. J. Tradit. Complement. Altern. Med. 2013, 10, 59–65. [Google Scholar] [PubMed] [Green Version]
- Basumatary, S.K.; Ahmed, M.; Deka, S.P. Some medicinal plant leaves used by Boro (tribal) people of Goalpara district, Assam. Nat. Prod. Radiance 2004, 3, 88–90. [Google Scholar]
- Ayyanar, M.; Ignacimuthu, S. Medicinal uses and pharmacological Actions of five commonly used Indian Medicinal plants: A mini-review. Iranian J. Pharm. Therapeut. 2008, 7, 107–114. [Google Scholar]
- Ghorbani, A. Studies on pharmaceutical ethnobotany in the region of Turkmen Sahra, North of Iran (Part 1): General results. J. Ethnopharmocol. 2005, 102, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Castellani, D.C. Plantas Medicinais; Agromídia Software: Viçosa, Brazil, 1999. [Google Scholar]
- Srivastava, T.N.; Badola, D.P.; Shah, D.C.; Gupta, O.P. Ethno-medico-botanical exploration of Gurez Valley Kashmir. Bull. Med. Ethno. Bot. Res. 1984, 5, 15–54. [Google Scholar]
- Khan, M.; Kumar, S.; Hamal, I.A. Medicinal plants of Sewa river catchment area in the Northwest Himalaya and its implication for conservation. Ethnobot. Leafl. 2009, 13, 1113–1119. [Google Scholar]
- Ssegawa, P.; Kasenene, J.M. Medicinal plant diversity and uses in the Sango bay area, southern Uganda. J. Ethnopharmacol. 2007, 113, 521–540. [Google Scholar] [CrossRef]
- Upadhyay, B.; Parveen; Dhaker, A.K.; Kumar, A. Ethnomedicinal and ethnopharmaco-statistical studies of Eastern Rajasthan, India. J. Ethnopharmocol. 2010, 129, 64–86. [Google Scholar] [CrossRef]
- Ong, H.G.; Kim, Y.D. Quantitative ethnobotanical study of the medicinal plants used by the Ati Negrito indigenous group in Guimaras Island. Philippines. J. Ethnopharmacol. 2014, 157, 228–242. [Google Scholar] [CrossRef] [PubMed]
- Poonam, K.; Singh, G.S. Ethnobotanical study of medicinal plants used by the Taungya community in Terai Arc Landscape, India. J. Ethnopharmocol. 2009, 123, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Roosita, R.; Kusharto, C.M.; Sekiyama, M.; Fachrurozi, Y.; Ohtsuka, R. Medicinal plants used by the villagers of a Sundanese community in West Java, Indonesia. J. Ethnopharmocol. 2008, 115, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Abe, R.; Ohtani, K. An ethnobotanical study of medicinal plants and traditional therapies on Batan island, the Philippines. J. Ethnopharmacol. 2013, 145, 554–565. [Google Scholar] [CrossRef]
- Lee, S.; Lee, E.; Park, W.; Kim, J.; Kim, E.; Choi, S. Anti-inflammatory and anti-osteoarthritis effects of fermented Achyranthes japonica Nakai. J. Ethnopharmacol. 2012, 142, 634–641. [Google Scholar] [CrossRef]
- Andrade-Cetto, A. Ethnobotanical study of the medicinal plants from Tlanchinol, Hidalgo, Mexico. J. Ethnopharmocol. 2009, 122, 163–171. [Google Scholar] [CrossRef]
- Ragupathy, S.; Steven, N.G.; Maruthakkutti, M.; Velusamy, B.; Ul-Huda, M.M. Consensus of the ‘Malasars’ traditional aboriginal knowledge of medicinal plants in the Velliangiri holy hills, India. J. Ethnobiol. Ethnomed. 2008, 4, 8. Available online: http://www.ethnobiomed.com/content/4/1/8 (accessed on 10 September 2020). [CrossRef] [Green Version]
- Rokaya, M.B.; Munzbergova, Z.; Timsina, B. Ethnobotanical study of medicinal plants from the Humla district of western Nepal. J. Ethnopharmocol. 2010, 130, 485–504. [Google Scholar] [CrossRef]
- Pandikumar, P.; Chellappandian, M.; Mutheeswaran, S.; Ignacimuthu, S. Consensus of local knowledge on medicinal plants among traditional healers in Mayiladumparai block of Theni District, Tamil Nadu, India. J. Ethnopharmacol. 2011. [Google Scholar] [CrossRef]
- Ragupathy, S.; Newmaster, S.G. Valorizing the ‘Irulas’ traditional knowledge of medicinal plants in the Kodiakkarai reserve forest, India. J. Ethnobiol. Ethnomed. 2009, 5, 10. [Google Scholar] [CrossRef] [Green Version]
- Tuomilehto, J.; Lindstrom, J.; Eriksson, J.; Valle, T.; Hamalainen, H. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Ugulu, I.; Baslar, S.; Yorek, N.; Dogan, Y. The investigation and quantitative ethnobotanical evaluation of medicinal plants used around Izmir province, Turkey. J. Med. Plants Res. 2009, 3, 345–367. [Google Scholar]
- Sharma, R.; Manhas, R.K.; Magotra, R. Ethnoveterinary remedies of diseases among milk yielding animals in Kathua, Jammu and Kashmir, India. J. Ethnopharmacol. 2012, 141, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Bolson, M.; Hefler, S.R.; Chaves, E.I.D.; Junior, A.G.; Junior, E.L.C. Ethnomedicinal study of plants used for treatment of human ailments, with residents of the surrounding region of forest fragments of Paraná, Brazil. J. Ethnopharmacol. 2015, 161, 1–10. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Locality | Distance from Jammu (km) | Total Population * | Sample (Population) Fraction | Sample Size of Proposed Informants (n) | Sample Size of Final Informants (fn) | Use-Reports Mentioned (UR) ** | Plant Species Identified | Relative Frequency (Rf,%) |
|---|---|---|---|---|---|---|---|---|
| Jasrota | 82 | 2665 | 0.0858 | 25 | 22 | 943 | 109 | 90.08 |
| Forlain | 75.3 | 6462 | 0.2080 | 11 | 11 | 489 | 59 | 48.76 |
| Kharot | 88.5 | 3549 | 0.1142 | 5 | 5 | 442 | 87 | 71.90 |
| Dhamaal | 42 | 859 | 0.0276 | 9 | 9 | 203 | 43 | 35.54 |
| Amala | 74 | 2021 | 0.0650 | 5 | 5 | 579 | 78 | 64.46 |
| Nanan | 77.6 | 768 | 0.0247 | 13 | 12 | 237 | 23 | 19.01 |
| Budhi | 76 | 3805 | 0.1224 | 10 | 9 | 212 | 29 | 23.97 |
| Merth | 73 | 1795 | 0.0578 | 8 | 8 | 398 | 67 | 55.37 |
| Jasrota fort (inside JWS) | 89 | 6 | 0.0002 | 3 | 2 | 126 | 57 | 47.11 |
| Shehswan | 79.5 | 2095 | 0.0674 | 7 | 6 | 213 | 29 | 23.97 |
| Bhorthain | 76.5 | 2508 | 0.0807 | 6 | 6 | 278 | 43 | 35.54 |
| Chelak | 44 | 4541 | 0.1461 | 18 | 18 | 867 | 101 | 83.47 |
| Total | 31,074 | 120 | 113 | 4987 | 121 |
| Informants | Male | Female | Total |
| 72 (67.72%) | 41 (36.28%) | 113 (100%) | |
| Age class | Male | Female | |
| 21–30 | 11 (15.28%) | 3 (7.32%) | 14 (12.39%) |
| 31–40 | 17 (23.61%) | 9 (21.95%) | 26 (23.01%) |
| 41–50 | 22 (30.56%) | 6 (14.63%) | 28 (24.78%) |
| 51–60 | 8 (11.11%) | 13 (31.71%) | 21 (18.58%) |
| 61–70 | 5 (6.94%) | 3 (7.32%) | 8 (7.08%) |
| 71–80 | 9 (12.50%) | 7 (17.07%) | 16 (14.16%) |
| Total | 72 (100%) | 41 (100%) | 113 (100%) |
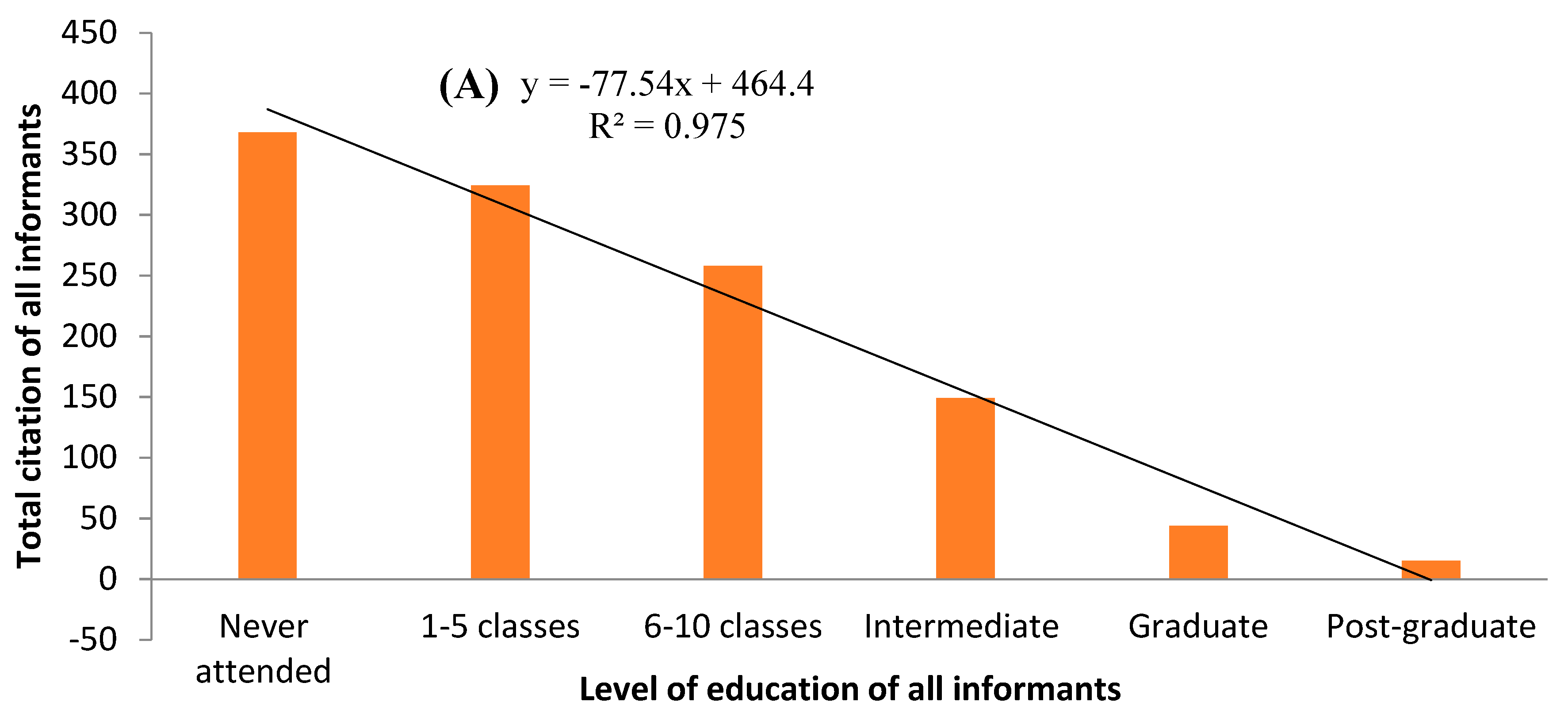
| Literacy level | Male | Female | |
| Never attended a school | 25 (34.72%) | 13 (31.71%) | 38 (33.63%) |
| Attended school for 1–5 classes | 17 (23.61%) | 18 (43.90%) | 35 (30.97%) |
| Attended school for 6–10 classes | 19 (26.39%) | 9 (21.95%) | 28 (24.78%) |
| Intermediate (12th class) | 7 (9.72%) | 1 (2.44%) | 8 (7.08%) |
| Graduate | 3 (4.17%) | 0 (-) | 3 (2.65%) |
| Post-graduate | 1 (1.39%) | 0 (-) | 1 (0.88%) |
| Total | 72 (100%) | 41 (100%) | 113 (100%) |
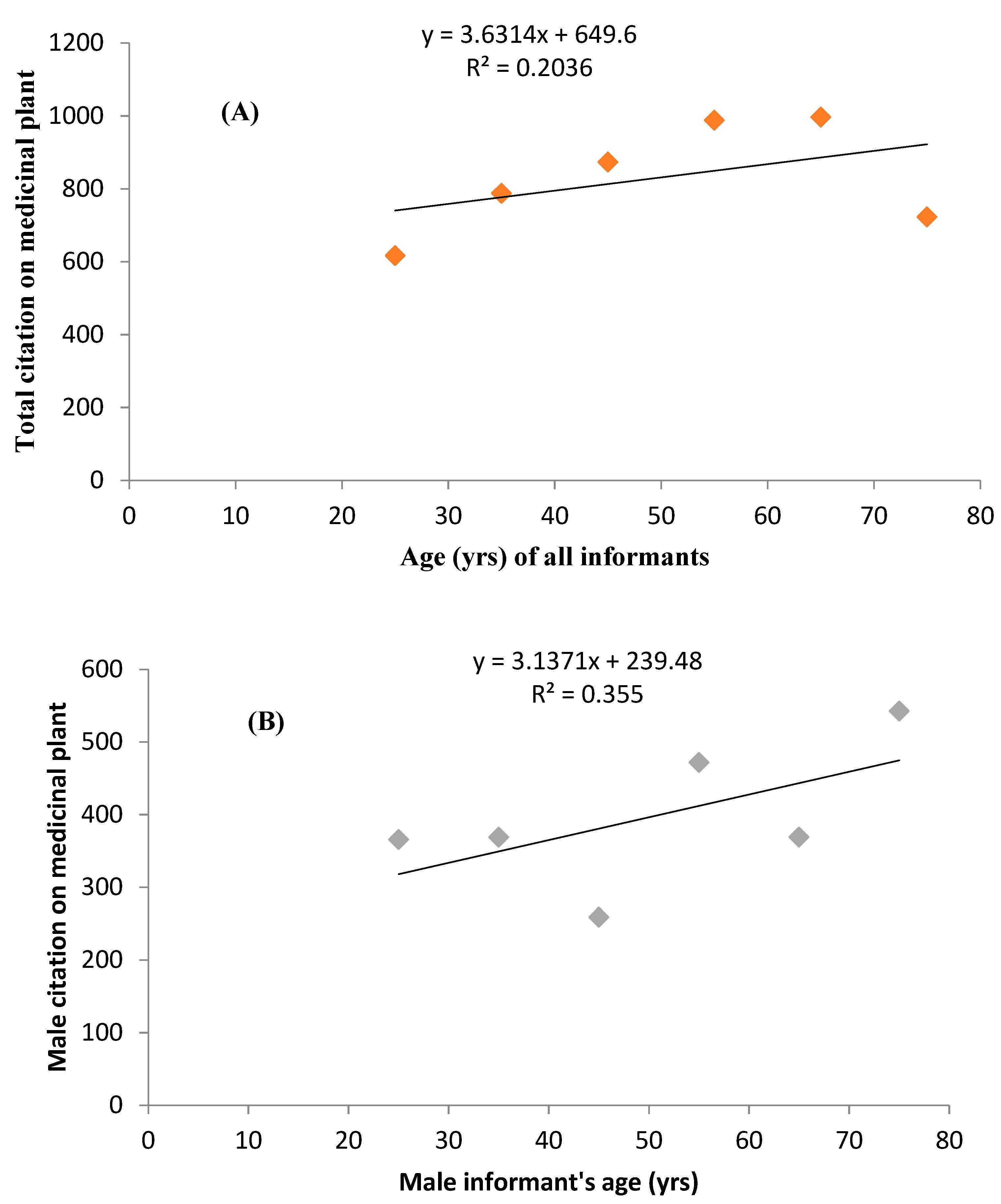
| Spearman rank correlation | r | p | |
| Total individuals or informants (n = 113; α = 0.01) | |||
| Individuals age vs number of citations | 0.257 | <0.001 ** | |
| Male individuals (n = 72; α = 0.01) | |||
| Individuals age vs citation number | 0.314 | <0.001 ** | |
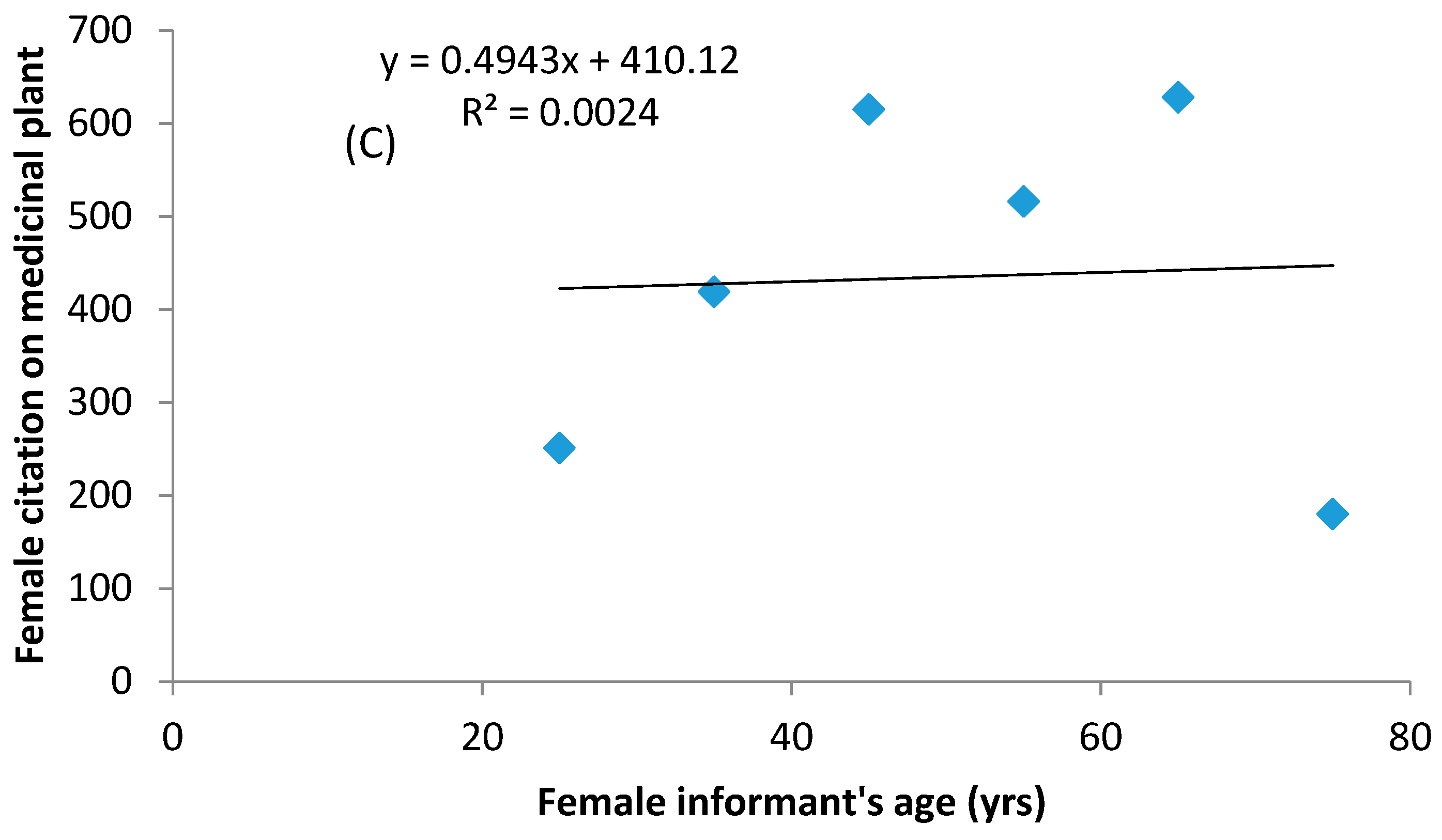
| Female individuals (n = 41; α = 0.01) | |||
| Individuals age vs citation number | 0.200 | <0.012 * |
| Ailments Categories | Important Ailments (or Disease) of a Category | Nur | %Nur | ICF | Nt | %Nt | %WP | %UGP | %BR | %AEP | %LR |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gastro-intestinal ailments (GIA) | constipation, abdominal spasms, acidity, dysentery, diarrhea, flatulence, vomiting, loss of consciousness, intestinal or oral ulcers, indigestion, stomachache, piles, laxative, nausea, aperients, appetizer, anthelmintic infections, halitosis | 1314 | 26.35 | 0.959 | 55 | 45.45 | 24.55 | 33.08 | 47.18 | 24.39 | 1.37 |
| Dermatological infections (DID) | cuts, itching, pimple, skin irritation, wound, abscess, acne, boils, burns, leukoderma, ringworm, leprosy, scabies, dermatitis, warts, stings of allergic plants | 946 | 18.97 | 0.961 | 38 | 31.40 | 18.67 | 24.20 | 22.58 | 17.58 | 24.66 |
| Respiratory systems diseases (RSD) | asthma, bronchitis, pneumonia, chest infection, cough, cold, influenza, pharyngitis, whooping cough | 592 | 11.87 | 0.961 | 24 | 19.83 | 12.28 | 11.49 | 4.84 | 12.50 | 6.85 |
| Skeleto-muscular system disorders (SMSD) | body pain, muscle pain, rheumatic pain, joint pain, bone fractures or bone broken, swellings in bone, arthralgia, | 482 | 9.67 | 0.958 | 21 | 17.36 | 9.08 | 4.90 | 8.87 | 10.80 | 10.96 |
| Gento-urinary ailments (GUA) | abortion, breast pain, delivery pain, lactation, over bleeding, sexual power, urine blockage or painful urination, venereal disease, male fertility, bloody urine, urinary bladder disorders, urinary stones, gynecological disorders (abortion, menstrual problems) | 352 | 7.06 | 0.949 | 19 | 15.70 | 3.96 | 1.23 | 4.84 | 8.85 | 20.55 |
| General health care (GHC) | brain tonic, memory enhancer, strengthening gums, blood purifier, | 246 | 4.93 | 0.947 | 14 | 11.57 | 6.78 | 6.43 | 0.81 | 4.39 | 9.59 |
| Fever (FVR) | body temperature, malaria, hay-fever, febrifuse, antipyretic, typhoid | 175 | 3.51 | 0.937 | 12 | 9.92 | 4.86 | 4.44 | 1.21 | 3.16 | 4.11 |
| Endocrinal system disorders (ESD) | diabetes, adrenal diseases, parathyroid | 137 | 2.75 | 0.971 | 5 | 4.13 | 7.16 | 0.00 | 0.40 | 2.45 | 1.37 |
| Hair care (HC) | removal of dandruffs, graying hair, hair growth, external parasites (lice, ticks), hair loss, hair tonic | 132 | 2.65 | 0.954 | 7 | 5.79 | 5.37 | 0.15 | 1.21 | 2.63 | 1.37 |
| Liver problems (LP) | jaundice, hepatitis, liver enlargement, liver pain | 132 | 2.65 | 0.954 | 7 | 5.79 | 0.90 | 5.51 | 0.00 | 2.72 | 1.37 |
| Dental care (DC) | foul odor, teeth strength, toothache, worms in gum and teeth | 118 | 2.37 | 0.974 | 4 | 3.31 | 2.17 | 0.31 | 0.40 | 2.97 | 2.74 |
| Ear, nose and eye problems (ENT) | color blindness, otalgia, earache, nasal infection, eye pain, blurred vision, conjunctivitis, eye inflammation, ophthalmia | 116 | 2.33 | 0.957 | 6 | 4.96 | 2.05 | 0.46 | 1.21 | 2.85 | 2.74 |
| Poisonous bites (PB) | poison bites, snake bites, scorpion sting | 115 | 2.31 | 0.956 | 6 | 4.96 | 1.41 | 5.21 | 1.61 | 1.83 | 9.59 |
| Mouth disorders (MD) | mouth and tongue ulcer, thrush, leukoplakia, cold sores | 111 | 2.23 | 0.936 | 8 | 6.61 | 0.51 | 2.30 | 0.00 | 2.82 | 1.37 |
| Cancerous (CC) | cancer—lung, tumor | 19 | 0.38 | 0.667 | 7 | 5.79 | 0.26 | 0.31 | 4.84 | 0.06 | 1.37 |
| Botanical Name (Family)/Voucher Specimen Number | Vernacular Name | Life-Form | Part Used | Use-Reports (UR) | Disease Category: Ailments Treated (No. of Use-Reports Included for Particular Ailment Only) | Mode of Usage | Nativity |
|---|---|---|---|---|---|---|---|
| Abrus precatorius L. (Fabaceae)/10103 | rati | L | Lv | 43 | SMSD:15 (bone fracture) RSD: 27 (cough, cold) MD: 8 (tongue ulcer) | decoction | N |
| Acacia catechu Willd. (Fabaceae)/10106 | khair | T | W | 29 | MD:23 (mouth ulcer) GIA: 16 (dysentery) As additive: 2 (UR) | decoction | N |
| Acacia nilotica Willd. (Fabaceae)/10109 | kikar | T | B | 19 | GIA:7 (pile cure) DID:12 (skin diseases) | paste | N |
| Achyranthes aspera L. (Amaranthaceae)/10108 | puthkanda | H | R | 126 | DC:66 (relieve toothache) LP: 28 (jaundice) PB:39 (snakebites) GUA: 37 (gynecological disorders) | chew | N |
| Acorus calamus L. (Acoraceae)/10074 | breen | H | Rh | 99 | GIA:77 (intestinal worms, acidity) LP:10 (liver pain, liver enlargement) RSD:12 (cough, heart infection) | powder | N |
| Adiantum capillus-veneris L. (Adiantaceae)/10104 | hansraj | H | Rh | 103 | GUA:27 (herpes) DID:76 (wound, abscess, acne, boils, burns) | paste | N |
| Aegle marmelos (L) Corr. (Rutaceae)/10102 | bill | T | Lv | 35 | LP:9 (cure jaundice) RSD:3 (asthma) ESD:23 (diabetes and associated disorders) | decoction | N |
| Aerva sanguinolenta (L.) Blume (Amaranthaceae)/10027 | bui | S | R | 28 | ENT:28 (ophthalmic infection in goats) | juice | N |
| Ageratum conyzoides L. (Asteraceae)/10029 | jungli pudina | H | Lv | 69 | DID:69 (stop bleeding of cut andwound) | paste | E |
| Albizia lebbeck (L.) Benth. (Caesalpinaceae)/10111 | sirin | T | B | 6 | GUA:6 (impotency) | powder | E |
| Aloe vera (L.) Burm.f. (Xanthorrhoeaceae)/10112 | sotthu katthalai | H | Lv | 113 | DID:113 (skin injuries, wounds, dermatitis) | paste | E |
| Alternanthera pungens Kunth (Amaranthaceae)/10107 | khaki | H | Wp | 17 | HC:7 (hair tonic) RSD:10 (tight chest, bronchitis, asthma and other lung troubles) | decoction | E |
| Amaranthus spinosus L. (Amaranthaceae)/10114 | kandiari | H | Lv | 12 | GIA:12 (laxative properties) | chew | E |
| Anagallis arvensis L. (Primulaceae)/10117 | kokoon | H | Wp | 32 | SMSD:15 (gout) DID:17 (dermatitis) | decoction | E |
| Argemone mexicana L. (Asteraceae)/10121 | peelikandiari | H | Lv | 18 | DID:7 (ringworm) RSD:11 (cough) | decoction | E |
| Artemisia scoparia Waldst. & Kit. (Asteraceae)/10110 | jhau | H | Wp | 38 | LP:12 (jaundice, hepatitis) GIA:28 (inflammation of gall bladder) | juice | E |
| Asparagus adscendens Roxb. (Asparagaceae)/10086 | sanspod | L | S | 47 | GUA:9 (urinary stones, menstrual problems) GHC:27 (tonic) As additive:11 (UR) | decoction | N |
| Azadirachta indica A.Juss (Meliaceae)/10123 | nim | T | Lv | 71 | GIA:27 (stomach ailments, intestinal worms) LP: 11 (jaundice) DID: 19 (skin irritation) DC: 46 (tooth strength, worms in gum) | juice | N |
| Barleria cristata L. (Acanthaceae)/10115 | jhinti, | S | Lv | 19 | RSD:13 (cough) SMSD:6 (reducing swellings) | decoction | E |
| Bauhinia variegata L. (Caesalpinaceae)/10118 | kared | T | Fl | 34 | GIA:34 (dysentery, diarrhea and piles) | powder | N |
| Boerhavia diffusa L. (Nyctaginaceae)/10076 | lit-sit | H | R | 109 | LP:44 (jaundice) GUA:9 (nocturnal emission, urine stone) GHC:67 (memory enhancement) ESD:8 (adrenal problem) GIA:29 (constipation, stomachache) | decoction | N |
| Bombax ceiba L. (Malvaceae)/10120 | simbal | T | R | 19 | GIA:19 (diarrhea) | decoction | N |
| Buddleja asiatica Lour. (Scrophulariaceae)/10119 | neemda | S | Lv | 37 | DID:19 (skin infections) FVR:17 (malaria) CC:2 (cancer) | paste | N |
| Butea monosperma Taub. (Fabaceae)/10124 | dhak | T | Fl | 24 | GUA:8 (urine blockage) DID:12 (skin problem) ENT:4 (eye inflammation) | powder | N |
| Calotropis procera R.Br. (Ascelpiadaceae)/10127 | desi ak | S | R | 46 | DID:29 (skin diseases) SMSD:17 (joint pain, arthralgia) | paste | E |
| Cannabis sativa L. (Cannabaceae)/10122 | bhang | H | Lv | 47 | PB:13 (poisonous insect bites) GUA:34 (pain relief) | decoction | E |
| Capsella bursa-pastoris Medik (Brassicaceae)/10125 | kralmond | H | Wp | 13 | GUA:5 (bloody urine) GIA:8 (diarrhea) | juice | E |
| Cardamine hirsuta L. (Brassicaceae)/10116 | hairy bittercress | H | Lv | 19 | CC:14 (cancer) GHC:12 (tonic) | juice | N |
| Carissa carandas L. (Apocynaceae)/10128 | kalakki | S | Wp | 38 | GIA:38 (stomachache) | decoction | N |
| Carissa spinarum L. (Apocynaceae)/10036 | garna | S | F | 24 | GIA:24 (stomach stones and piles) | powder | E |
| Cassia fistula L. (Caesalpinaceae)/10011 | karangal | T | Lv | 91 | RSD:2 (pneumonia) GIA:67 (constipation, diarrhea, flatulence) DID:17 (skin infections) RSD:16 (cough, bronchitis) | decoction | N |
| Cassia occidentalis L. (Caesalpinaceae)/10126 | kasundi | S | S | 31 | GIA:17 (aperients, constipation) As additive:14 (UR) | powder | E |
| Cassia tora L. (Caesalpinaceae)/10129 | lohki | H | Lv | 43 | FVR:13 (fever) GIA:16 (stomachache) DID:18 (ringworm, leprosy) PB:2 (snake bite) | decoction | E |
| Catharanthus rosea (L.) G.Don (Apocynaceae)/10132 | sadabahar | H | Lv | 16 | DID:8 (skin disorders) GHC:9 (memory enhancement) CC:15 (cancer) | juice | E |
| Centella asiatica (L.) Urb. (Apiaceae)/10015 | brahmi | H | Lv | 57 | GHC:17 (brain tonic, blood purifier) DID:48 (skin problems) | juice | N |
| Cissampelos pareira L. (Menispermaceae)/10040 | battal bel | L | Lv | 58 | GHC:5 (brain tonic for improving memory) PB:17 (all types poisonous bites) DID:16 (skin infections, skin ulcer) FVR:23 (fever) GUA:19 (urinary problems) | decoction | N |
| Citrus medica L. (Rutaceae)/10130 | gargal | T | Lv | 53 | GIA:53 (diarrhea, stomachache) | powder | N |
| Colebrookia oppositifolia Sm. (Lamiaceae)/10056 | duss | S | Lv | 77 | DID:77 (wound, cut and bruises) | paste | N |
| Convolvulus arvensis L. (Convolvulaceae)/10134 | hiran padi | H | Lv | 11 | DID:11 (skin itching) | paste | N |
| Cuscuta reflexa Roxb. (Convolulaceae)/10131 | andal | L | Wp | 87 | DID:32 (skin itching, wound) GUA:39 (urinary problems) GHC:16 (health tonic) | decoction | N |
| Cynodon dactylon (L.) Pers (Poaceae)/10071 | khabbal | H | R | 33 | GIA:3 (piles) DID:5 (wound) GHC:18 (brain tonic) As additive:7 (UR) | decoction | N |
| Cyperus rotundus L. (Cyperaceae)/10135 | dila | H | R | 67 | PB:37 (antidote for all poisons) FVR:22 (malaria) GUA:8 (menstrual problems) | decoction | N |
| Dalbergia sissoo Roxb. (Fabaceae)/10138 | taail | T | Lv | 8 | GUA:8 (menstrual disorders) | decoction | N |
| Daphne oleoides Schreb (Thymelaeaceae)/10140 | kochhad | S | Lv | 19 | DID:19 (abscess) | paste | N |
| Datura metel L. (Solanaceae)/10137 | umatthai | H | Lv | 47 | ENT:27 (earache) GUA:20 (pain, stomachache) | juice | E |
| Dioscorea deltoidea Wall ex Kunth. (Dioscoreaceae)/10133 | kins | L | Lv | 42 | DID:27 (wounds, burns) SMSD:15 (swelling) | paste | N |
| Eclipta prostrata L. (L.) (Asteraceae)/10136 | bhangra | H | Wp | 116 | HC:21 (hair tonic) LP:47 (liver problems) RSD: 69 (asthma, cough) DID:27 (skin disorders) | powder | N |
| Euphorbia helioscopia L. (Euphorbiaceae)/10139 | dudhal-patal | H | La | 12 | DID:12 (abscess) | paste | E |
| Euphorbia hirta L. (Euphorbiaceae)/1006 | dudii | H | Wp | 115 | GIA:13 (piles) RSD:77 (cough, bronchitis, asthma) GIA:26 (dysentery, digestive disorders) | powder | N |
| Evolvulus alsinoides L. (Convolvulaceae)/10146 | neeli Santh | H | Wp | 23 | GHC:23 (brain tonic) | powder | N |
| Ficus hispida L.f. (Moraceae)/10148 | kharkhumbal | T | F | 13 | GUA:13 (galactagogue, venereal disease) | powder | N |
| Ficus palmata Forsk. (Moraceae)/10154 | phagara | T | F | 15 | GIA:7 (constipation) SMSD:8 (bone inflammation) | powder | N |
| Ficus racemosa L. (Moraceae)/10151 | rumbal | T | F | 36 | GIA:28 (kidney problems) SMSD:8 (bone inflammation) | powder | N |
| Ficus religiosa L. (Moraceae)/10144 | bar, peepal | T | S | 44 | GIA:29 (piles) SMSD:17 (bone inflammation) | decoction | N |
| Galium aparine L. (Rubiaceae)/10143 | khorti | H | Wp | 33 | GIA:33 (laxative properties) | juice | N |
| Geranium wallichianum Sweet. (Geraniaceae)/10152 | laal jehari | H | Lv | 29 | GIA:29 (diarrhea, dysentery) | decoction | N |
| Hedera nepalensis K.Koch (Araliaceae)/10135 | bano | H | Lv | 23 | SMSD:13 (arthralgia) RSD:7 (bronchitis) GUA:4 (diuretic) | juice | N |
| Hibiscus rosa-sinensis L. (Malvaceae)/10147 | gudaal | S | Fl | 47 | HC:27 (alopecia) GUA:14 (diuretic) | paste | N |
| Holarrhena antidysenterica Wall. ex A.DC. (Apocynaceae)/10142 | kagar | T | B | 44 | GIA:35 (dysentery) SMSD:14 (anti-spasmodic) | decoction | N |
| Ipomoea carnea Jacq. (Convolvuaceae)/10145 | bilaitti Aak | S | Lv | 51 | SMSD:51 (joint pain) | paste | E |
| Jasminum humile L. (Oleaceae)/10141 | sanairad | L | R | 23 | DID:13 (ring worm) ESD:10 (reduce blood sugar) | decoction | E |
| Justicia adhatoda L. (Acanthaceae)/10031 | brenkar | S | R | 104 | RSD:77 (cough, asthma, bronchitis) CC:1 (cancer) As additive: 26 (UR) | juice | N |
| Lannea coromandelica (Houtt.) Merr. (Anacardiaceae)/10150 | kamble | T | Lv | 41 | DID:24 (skin disease) MD:15 (mouth ulcer) DC:13 (toothache) | chew | N |
| Lantana camara L. (Verbenaceae)/1002 | panjphulli | S | La | 43 | HC:10 (promote hair growth) RSD:33 (asthma, bronchitis) DID:13 (skin itching) | decoction | E |
| Lawsonia inermis L. (Lythraceae)/10145 | mahendi | S | Lv | 38 | GIA:23 (stomachache) DID:17 (leukoderma, skin care) | juice | E |
| Linum usitatissimum L. (Linaceae)/10153 | alsi | H | S | 47 | DID:16 (abscess) GIA:29 (constipation) | paste | E |
| Lotus corniculatus L. (Fabaceae)/10158 | sadai | H | Wp | 39 | GHC:15 (tonic) GIA:27 (nauseaand vomiting) | juice | E |
| Mallotus philippensis Muell.Arg. (Eurphorbiaceae)/1005 | kamala | T | F | 36 | GIA:23 (killing worms instomach; constipation) CC:25 (cancer) | powder | N |
| Malvastrum cormandelianum (L.) Garcke (Malvaceae)/10161 | baddi Bareaar | H | Lv | 39 | DID:39 (styptic, skin infections) | paste | E |
| Medicago lupulina L.(Fabaceae)/10159 | sareri | H | Lv | 17 | GIA:17 (constipation) | powder | E |
| Melilotus indica All. (Fabaceae)/10063 | pili senji | H | Lv | 67 | GIA:22 (aperient) DID:47 (skin aching) | decoction | E |
| Mentha arvensis L. (Lamiaceae)/10155 | pootna | H | Lv | 106 | GIA:66 (flatulence, aperients, indigestion, acidity) SMSD:45 (abdominal spasms, joint pain, rheumatism) | decoction | E |
| Mentha longifolia (L) Huds (Lamiaceae)/10164 | jangali pootna | H | Lv | 119 | GIA:36 (flatulence, aperients) SMSD:84 (abdominalspasms, rheumatism) | decoction | N |
| Millingtonia hortensis L.f. (Bignoniaceae)/1007 | buchade jhad | T | Lv | 19 | FVR:7 (antipyretic) DID:3 (sinusitis) GIA:5 (cholagogue) GHC:7 (tonic) | juice | N |
| Morus alba L. (Moraceae)/10157 | toot | T | Lv | 38 | GIA:14 (aperients) LP:32 (jaundice) | juice | E |
| Murraya koenigii (L.) Spreng. (Rutaceae)/10163 | karuveppilai | T | Lv | 28 | ENT:8 (eye pain) GIA:27 (dysentery, vomiting) | decoction | N |
| Nerium indicum Mill. (Apocynaceae)/10166 | lal kaneer | S | Lv | 13 | RSD:13 (heart ailments) CC:1 (cancer) | juice | E |
| Nicotiana plumbaginifolia Viv. (Solanaceae)/10160 | desi Tamakoo | H | Wp | 48 | GIA:48 (external parasites) | paste | E |
| Nyctanthes arbor-tristis L. (Oleaceae)/10156 | haar-shringaar | S | Lv | 13 | GIA:13 (intestinal worms) | juice | N |
| Oenothera rosea Soland (Onagraceae)/10162 | darraati | H | Lv | 44 | GUA:44 (renal colic) | decoction | E |
| Oxalis corniculata L. (Oxalidaceae)/10187 | khattibooti | H | Lv | 48 | DC:33 (toothache) GIA:15 (halitosis) | chew | E |
| Phoenix sylvestris (L.) Roxb.(Areaceae)/10066 | khaajuri | T | Lv | 6 | RSD:2 (heart complaints) FVR:1 (fever) GIA:3 (vomiting, loss of consciousness) | juice | E |
| Phyllanthus amarus Schum & Thonn. (Euphorbiaceae)/10191 | keelanelli | H | Wp | 87 | GIA:83 (jaundice, diarrhea, dysentery) MD:7 (peptic ulcer) | decoction | N |
| Phyllanthus emblica L. (Euphorbiaceae)/10195 | aamla | T | B | 90 | GIA:35 (constipation) HC:13 (hair loss) GHC:48 (tonic as rejuvenator) | powder | N |
| Physalis minima L. (Solanaceae)/10189 | pataka | H | Lv | 23 | ENT:23 (otalgia) | juice | E |
| Pinus roxburghii Roxb. (Pinaceae)/10064 | chir-pine | T | Re | 19 | DID:19 (boils, cuts, wounds) | paste | N |
| Pogostemon benghalensis (Burm.f.) Ktze. (Lamiaceae)/10194 | kali Suaali | S | Lv | 25 | GIA:14 (dyspepsia) RSD:11 (cold, cough) | decoction | N |
| Pogostemon plectranthoids Desf. (Lamiaceae)/10004 | thekkali | S | Lv | 32 | GIA:19 (vomiting, diarrhea) RSD:13 (cold) SMSD:5 (headache) | decoction | N |
| Polygonum amplexicaule D.Don. (Polygonaceae)/10193 | masloon | H | R | 13 | RSD:13 (cold, cough) | chew | N |
| Polygonum hydropiper L. (Polygonaceae)/10192 | pipli | H | Wp | 28 | GIA:19 (diarrhea, piles) GUA:11 (painful menstruation, over bleeding) | decoction | N |
| Prunus persica (L.) (Rosaceae)/10188 | aru | T | Lv | 33 | DID:33 (cut, wound, burns, boils to soothe inflammation) | paste | E |
| Punica granatum L. (Punicaceae)/10190 | darunni | T | F | 47 | LP:46 (jaundice) GHC:7 (tonic) | powder | N |
| Pyrus pashia Buch.-Ham. ex D.Don (Rosaceae)/10051 | batangi | T | F | 26 | ENT:26 (eye infection) | juice | E |
| Ranunculus arvensis L. (Ranunculaceae)/10165 | charmula | H | Wp | 24 | GIA:14 (diarrhea) FVR:7 (fever) RSD:3 (asthma) | juice | N |
| Ranunculus laetus Wall. (Ranunculaceae)/10172 | darrili | H | La | 6 | HC:6 (hair growth) | juice | E |
| Ranunculus muricatus L. (Ranunculaceae)/10037 | korkhand | H | Wp | 26 | FVR:15 (periodic fever) SMSD:1 (arthralgia) RSD:13 (asthma) | juice | N |
| Ricinus communis L. (Euphorbiaceae)/10174 | arandi | S | Lv | 42 | SMSD:42 (headache) | paste | E |
| Robinia pseudoacacia L. (Fabaceae)/10176 | kikkar | T | Lv | 27 | GIA:27 (acidity, indigestion) | juice | E |
| Rosa indica L. (Rosaceae)/10178 | gulab | S | Fl | 19 | GIA:19 (indigestion, flatulence) | decoction | N |
| Rubus ellipticus Sm. (Rosaceae)/10061 | aakhey | S | Fr | 31 | GIA:15 (aperients) MD:17 (oral ulcer) | juice | N |
| Salvia moorcroftiana Wallich ex Benth. (Lamiaceae)/10180 | kali jadi | H | R | 19 | RSD:5 (cold) GIA:10 (stomachache and dysentery) FVR:5 (fever) | powder | N |
| Sida cordifolia L. (Malvaceae)/10042 | vandhamni | H | Wp | 11 | GIA:11 (stomachache) | decoction | N |
| Sida spinosa L. (Malvaceae)/10168 | gulsakari | H | Lv | 37 | SMSD:37 (demulcent, irritation) | decoction | E |
| Solanum nigrum L. (Solanaceae)/10173 | kaayankothi | H | Lv | 18 | FVR:5 (antiphlogistic) GIA:3 (stomach ulcer) DID:17 (wound) | paste | E |
| Stellaria media (L.) Vill. (Caryophyllaceae)/10062 | marmiri | H | Wp | 9 | SMSD:9 (swelling, bone fracture) | paste | E |
| Synedrella nodiflora (L.) Garetn. (Asteraceae)/10167 | jari | H | Lv | 11 | DID:11 (styptic) | decoction | E |
| Syzygium cumini (L.) Skeels (Myrtaceae)/10030 | jaamnoo | T | Lv | 26 | ESD: 24 (diabetes) CC:3 (cancer) | decoction | N |
| Tamarindus indica L. (Caesalpinaceae)/10175 | Lmli | T | F | 29 | PB:29 (anorexia, poisonous weed intake) | decoction | N |
| Taxodium distichum (L.) Rich (Cupressaceae)/10171 | - | T | Re | 6 | DID:6 (analgesic for wounds) | paste | E |
| Tephrosia purpurea (L.) Pers (Fabaceae)/10181 | sarphank | H | R | 43 | FVR:43 (typhoidfever) | powder | N |
| Tinospora cordifolia (Wild.) Hook.f. & Thomson (Memispermaceae)/10185 | Gloe | L | R | 105 | FVR:27 (hay fever) ESD:69 (diabetes) LP:12 (hepatitis) SMSD:33 (joint pain, rheumatism) | powder | N |
| Toona ciliata M.Roem (Meliaceae)/10170 | Toon | T | Lv | 9 | DID:5 (astringent) GHC:7 (tonic) | decoction | N |
| Tribulus terrestris L. (Zygophyllaceae)/10184 | pakhra, | H | F | 56 | GUA:37 (impotency) SMSD:21 (bone swelling) | powder | N |
| Trifolium pratense L. (Fabaceae)/10186 | gagar luth | H | Wp | 37 | SMDS:37 (anti-spasmodic) | decoction | N |
| Verbascum thapsus L. (Scrophulariceae)/10179 | soottamakoo | H | F | 38 | RSD:38 (cough, asthma, pneumonia) | juice | N |
| Vernonia arborea Buch.Ham (Asteraceae)/10012 | vernonia | T | B | 14 | MD:14 (mouth, tongue ulcers) | paste | N |
| Viola odorata L. (Violaceae)/10169 | banaksha | H | Fl | 67 | RDS:67 (cough, bronchitis, cold) | decoction | N |
| Vitex negundo L. (Verbenaceae)/10182 | Bana | S | Fl | 88 | GIA:27 (diarrhea, anthelminthic) RDS:57 (cough) SMSD:21 (bone pain, rheumatism) | juice | N |
| Woodfordia fruticosa Kurz (Lythraceae)/10177 | Dhai | S | Fl | 49 | DID:24 (skin disease) SMSD:5 (headache) GIA:29 (diarrhea, dysentery) | decoction | N |
| Xanthium strumarium L. (Asteraceae)/10044 | Jojra | S | Lv | 17 | SMSD:17 (headache) | decoction | E |
| Ziziphus nummularia (Burm.f) Wight & Arn. (Rhamnaceae)/10183 | jhar beri | S | F | 57 | GIA:57 (diarrhea, dysentery, colic) | powder | N |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singh, B.; Singh, B.; Kishor, A.; Singh, S.; Bhat, M.N.; Surmal, O.; Musarella, C.M. Exploring Plant-Based Ethnomedicine and Quantitative Ethnopharmacology: Medicinal Plants Utilized by the Population of Jasrota Hill in Western Himalaya. Sustainability 2020, 12, 7526. https://doi.org/10.3390/su12187526
Singh B, Singh B, Kishor A, Singh S, Bhat MN, Surmal O, Musarella CM. Exploring Plant-Based Ethnomedicine and Quantitative Ethnopharmacology: Medicinal Plants Utilized by the Population of Jasrota Hill in Western Himalaya. Sustainability. 2020; 12(18):7526. https://doi.org/10.3390/su12187526
Chicago/Turabian StyleSingh, Bishander, Bikarma Singh, Anand Kishor, Sumit Singh, Mudasir Nazir Bhat, Opender Surmal, and Carmelo Maria Musarella. 2020. "Exploring Plant-Based Ethnomedicine and Quantitative Ethnopharmacology: Medicinal Plants Utilized by the Population of Jasrota Hill in Western Himalaya" Sustainability 12, no. 18: 7526. https://doi.org/10.3390/su12187526