

Preventative Sensor-Based Remote Monitoring of the Diabetic Foot in Clinical Practice
 , ,
, ,
Abstract
:1. Introduction
2. Technology Architecture and Implementation
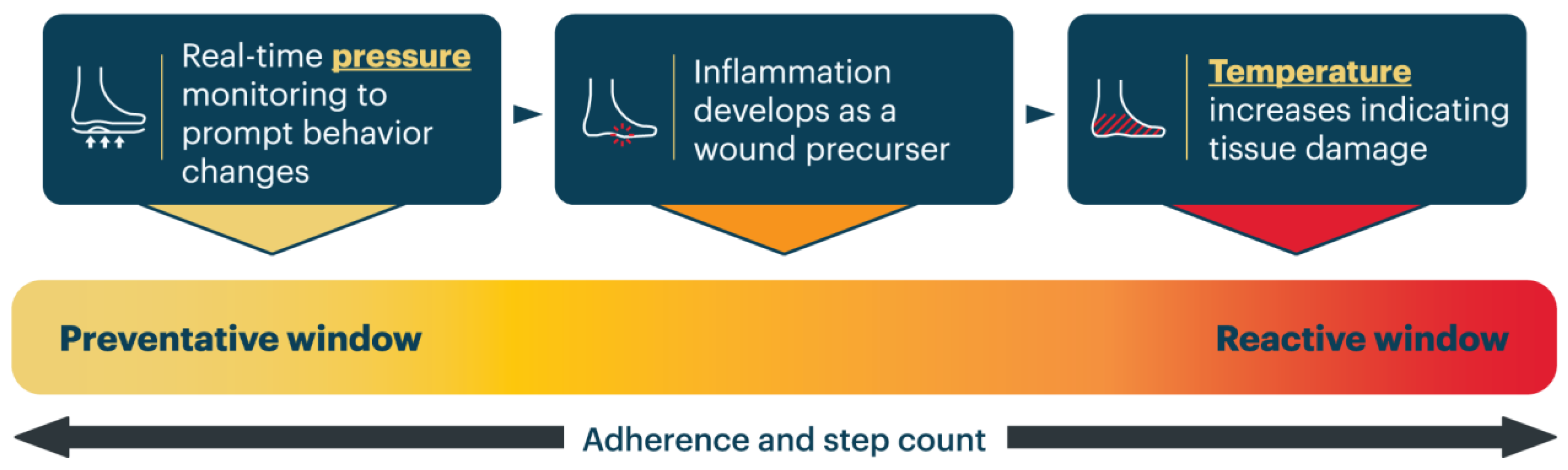
2.1. Temperature Monitoring
2.2. Pressure Monitoring
2.3. Activity Monitoring
3. Patient Selection
- Patients with Type 1 or Type 2 Diabetes with established peripheral neuropathy (PN) and loss of protective sensation (LOPS) as established by the Semmes–Weinstein monofilament test;
- Patients who are willing and open to engaging in their diabetic foot health through digital prevention and an RPM service;
- Patients with the cognitive capacity and technological fluency to understand the digital device and its operation;
- A supportive care environment is also an asset but does not preclude the possibility of benefit from RPM.
4. Clinical Assessment and Data Collection
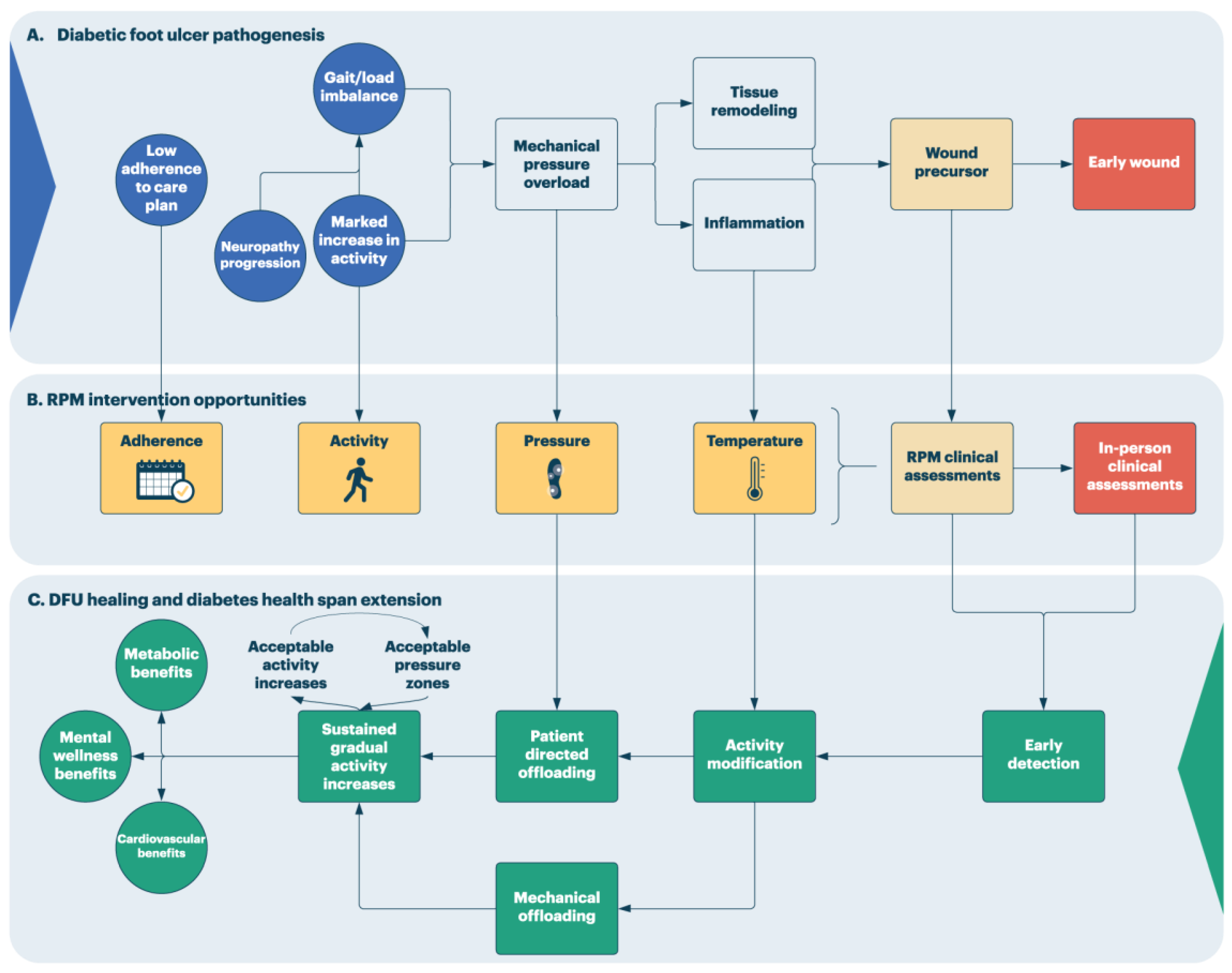
5. Remote Patient Monitoring for Diabetic Foot Ulcer Prevention: Overview
6. Prediction System Quality Management in Remote Patient Monitoring Systems
“False positives are one of the worst things you can do to an early warning system” (Chesley Sullenberger, Captain of US Airways Flight 1549, “Miracle on the Hudson”)[67]
7. Implementation, Opportunities, and Limitations of Sensor-Based RPM in Clinical Practice
- Patient selection
- ○
- Patient selection plays a key role in the success of any RPM program. Patients should be identified and reviewed against patient selection characteristics, such as those outlined in this perspective, prior to patient enrollment in the RPM program. The goals of the program should be discussed with the patient, along with the responsibilities of the patient, clinician, and RPM service provider.
- Escalation and communication
- ○
- RPM escalation protocols should be reviewed and agreed upon by the treating clinician and should clearly establish and outline communication methods and response timelines.
- ○
- Training of relevant personnel on the sensor-based technology and associated RPM protocols is an important step in the implementation of an RPM program. Training should be provided not only to the patient but also to those involved in the patient’s care, including the treating clinician, clinic staff, and the patient’s support system.
- Technology selection
- ○
- The specific hardware and software deployed to collect the remotely monitored data may differ based on patient-specific requirements and needs. In the context of DFU prevention, this may take the form of sensor-embedded wearables such as insoles or socks that can be used throughout daily activities or non-wearable sensor-embedded technology such as a mat or recording device that can be used at home [30,31,35,71].
- ○
- The RPM technology should ultimately be selected based on factors that consider the patient’s underlying disease state, lifestyle goals and constraints, technological fluency, and engagement with their overall health. The technology selection will also be influenced by the care providers’ familiarity with the technology and whether the technology is covered by insurance [24].
- Technological learning curve
- ○
- Due to the nature of sensor-based RPM, there is a technological learning curve that patients and clinicians face. Patients that have some experience with technology-based solutions may find it easier to participate in such programs. Patients that are not comfortable with technology or that do not have the appropriate support system to help learn a new technology may face additional barriers to success in a digital-based RPM program and require additional support.
- ○
- Other patient factors, such as dexterity and visual impairment, should be acknowledged, depending on the form factor of the technology.
- Patient acceptance and engagement
- ○
- Success in a digital, sensor-based RPM program relies heavily on patient engagement with the technology and remote monitoring nurse. It is also helpful for the treating clinician to provide support and encouragement to both the patient and RPM nurse, facilitating a team approach to patient care.
- Data privacy
- ○
- It is of the utmost importance that digital, sensor-based RPM providers adhere to standards of digital health information storage. This includes, but is not limited to, the Health Insurance Portability and Accountability Act (HIPAA) in the United States and equivalent provisions in other jurisdictions.
8. Patient Assessment through RPM Services
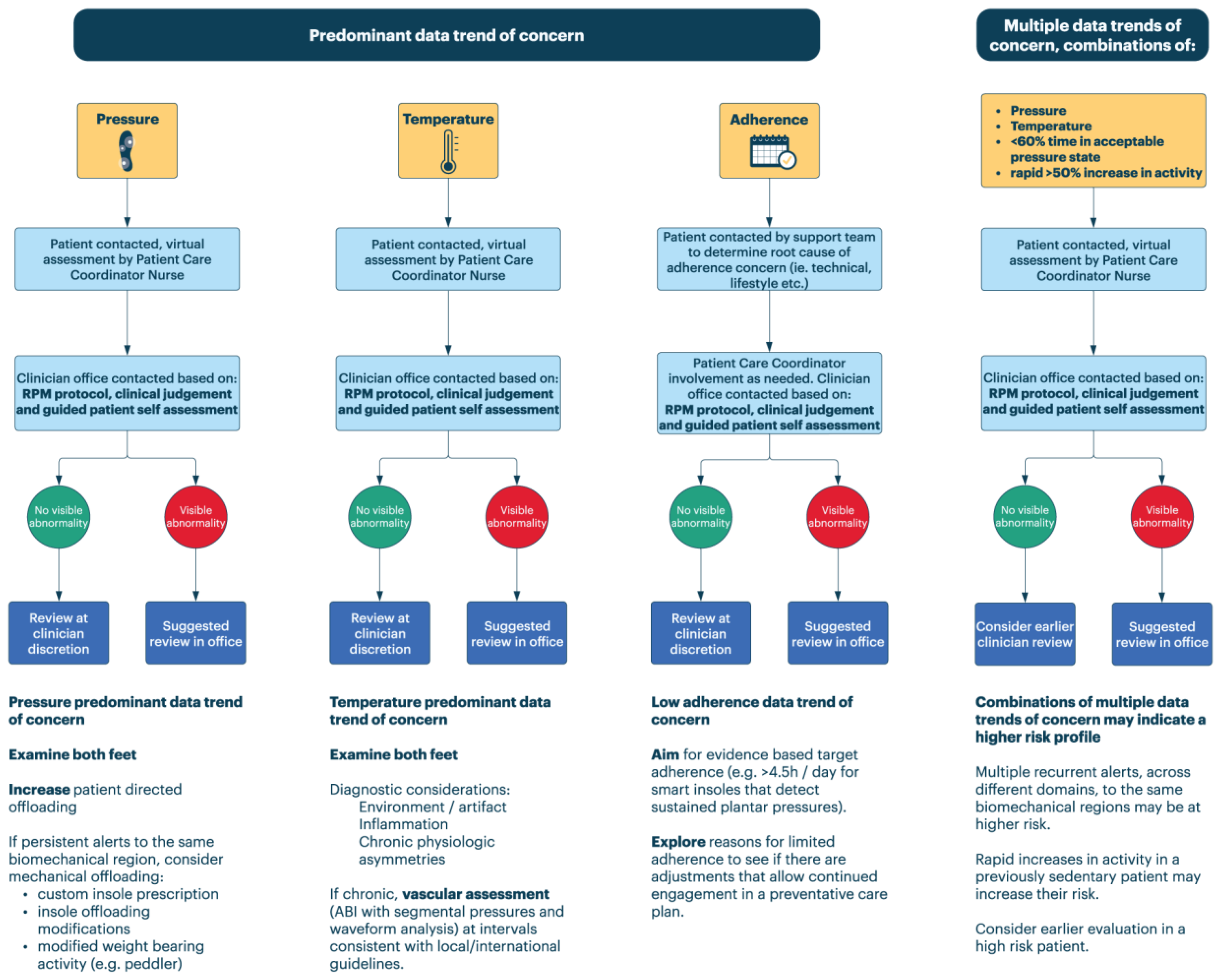
- When data trends of concern are noted, patients are contacted in accordance with clinical guidelines internal to the RPM service provider. This clinical guidance should be re-evaluated at regular intervals and serves to create predictable care processes and reduce unnecessary care variation within the RPM service.
- When patient contact is initiated, it should include an assessment of the physiologic data generating the concerning trend and the clinical context by a licensed healthcare professional.
- Patient contact includes a remote assessment of the patients’ feet (self-guided exam) when possible and reinforces best practices in integrative foot care [13].
- In cases where that assessment reveals visible abnormalities or other signs of clinical concern, the clinician’s office is notified directly.
- In cases where there are no such concerns identified, communication of the data triggering the concern, clinical context, and interaction with the patient proceeds via documentation in the legal record of care shared between the RPM provider and the treating team or through some other reporting mechanism. These cases, as well as true positives, should inform further refinement of the prediction system.
9. Clinical Response to RPM Escalation
9.1. Pressure Predominant Data Trend of Concern
- Clinicians may be tempted to focus an exam on a particular region that is generating data trends of concern. While that may indeed be an area of pressure overload, anchoring in a particular region should be avoided. It is important that both feet are assessed.
- ○
- Early experience suggests pre-ulcerative pathogenesis might see pressure warnings preceding dermal changes in the same region or in different regions.
- ○
- This may proceed through known biomechanical mechanisms (e.g., load switching between metatarsal heads 1 and 5), through patient offloading to a contralateral limb, or simply due to a change in activity that causes a broader alert pattern.
- Higher risk situations may involve recurrent data trends of concern to the same biomechanical regions.
- ○
- Consider mechanical adjustment if this is persistent.
- Changes in activity levels may generate more cumulative load on the foot tissues and more pressure-related data trends of concern [74]. Some research also suggests that high day-to-day variability in activity, regardless of activity volume, may put individuals at higher risk of ulceration [75]. However, risk in such situations must be balanced against established cardiovascular, metabolic, and mental benefits of increasing mobility in high-risk populations. Digital therapeutics and RPM services need to be aligned with broader goals for healthy living.
- In keeping with those goals, the following clinical actions are suggested:
- ○
- In cases of a recent, abrupt increase in activity (absent any evidence as to what is definitively unsafe, a definition of >50% of monthly baseline over a few days is used), consider counselling towards gradual increases instead, if possible [63].
- ○
- If patient-facing alerts are provided by the digital prevention device, counsel towards higher interaction so that risks of increases in the activity to the diabetic foot can be more effectively managed through patient offloading [30].
- ○
- Through health coaching and techniques in motivational interviewing, and in the absence of pressure data trends of concern or in a setting where they are reliably offloaded, aim for monthly increases in activity of 10% [13].
9.2. Temperature Predominant Data Trend of Concern
- Pre-enrollment vascular assessment (preferably through ABI with segmental pressures and Doppler waveform analysis) at an interval appropriate to local guidelines can be helpful in contextualizing possible perfusion differences [58].
- Clinicians may be tempted to focus an exam on a particular region that is generating temperature data trends of concern. While that may be a focal area of inflammation, anchoring on a particular region should be avoided. It is important that both feet are assessed.
- Temperature asymmetry may be driven by areas of relative warmth or coolness.
- ○
- ○
- Relative temperature differences have low specificity in DFU prediction and may be driven by [54]:
- ○
- A meta-analysis of five temperature monitoring RCTs including 772 patients has recently provided low certainty evidence suggesting a risk reduction is associated with home skin temperature monitoring when ambulatory activity is reduced (e.g., by greater than 50% [59]) in response to detected hot spots [16]. Given the prevalence of false positives in the temperature domain [54], the potential impact of such a recommendation on the need for activity promotion in diabetic patients merits some consideration [65]. In view of this, some providers may want to consider other forms of activity modification (e.g., non-weight-bearing exercise). The safety of such approaches should be further studied, and providers should exercise their clinical judgment in balancing foot health concerns against activity promotion goals.
9.3. Adherence Predominant Data Trend of Concern
- Aim for an evidence-based adherence target (e.g., >4.5 h per day (for insoles that deliver alerts in response to sustained elevated plantar pressure [30]));
- Explore reasons for limited adherence to see if there are adjustments that can be made to allow for continued engagement in a preventative care plan.
9.4. Multiple Data Trends of Concern
10. Sensor-Based Preventative Care Will Enhance Our Understanding of DFU Pathogenesis and Promote a Systems-Based Approach to Prevention
“Everything should be made as simple as possible, but not simpler” (Possibly Albert Einstein, as paraphrased by L. Zukofsky and then R. Sessions).[81]
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas Tenth Edition 2021. Available online: https://diabetesatlas.org/ (accessed on 25 April 2023).
- Armstrong, D.G.; Tan, T.-W.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers: A Review. JAMA 2023, 330, 62–75. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef]
- Singh, N.; Armstrong, D.G.; Lipsky, B.A. Preventing Foot Ulcers in Patients with Diabetes. JAMA 2005, 293, 217–228. [Google Scholar] [CrossRef]
- Yazdanpanah, L. Literature review on the management of diabetic foot ulcer. World J. Diabetes 2015, 6, 37. [Google Scholar] [CrossRef] [PubMed]
- Brennan, M.B.; Powell, W.R.; Kaiksow, F.; Kramer, J.; Liu, Y.; Kind, A.J.H.; Bartels, C.M. Association of Race, Ethnicity, and Rurality with Major Leg Amputation or Death among Medicare Beneficiaries Hospitalized with Diabetic Foot Ulcers. JAMA Netw. Open 2022, 5, e228399. [Google Scholar] [CrossRef] [PubMed]
- Rowe, V.L. Diabetic Foot Ulcers: Practice Essentials, Pathophysiology, Etiology. January 2023. Available online: https://emedicine.medscape.com/article/460282-overview#a7 (accessed on 31 March 2023).
- Simón-Pérez, E.; Simón-Pérez, C.; Alonso-Peña, D.; Pontón-Cortina, A.; Chicharro-Luna, E.; Martínez-Nova, A.; Navarro-Flores, E. Stiffness degree of ankle range of motion in diabetic patients with atypical amputation. Rev. Assoc. Med. Bras. 2020, 66, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Mishra, R. Harnessing Digital Health Technologies to Remotely Manage Diabetic Foot Syndrome: A Narrative Review. Medicina 2021, 57, 377. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Swerdlow, M.A.; Armstrong, A.A.; Conte, M.S.; Padula, W.V.; Bus, S.A. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J. Foot Ankle Res. 2020, 13, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Margolis, D. Data Points #3: Economic Burden of Diabetic Foot Ulcers and Amputations | Effective Health Care (EHC) Program. 2011. Available online: https://effectivehealthcare.ahrq.gov/products/diabetes-foot-ulcer-amputation-economics/research (accessed on 31 March 2023).
- Ahmad, A.; Abujbara, M.; Jaddou, H.; Younes, N.A.; Ajlouni, K. Anxiety and Depression Among Adult Patients with Diabetic Foot: Prevalence and Associated Factors. J. Clin. Med. Res. 2018, 10, 411–418. [Google Scholar] [CrossRef] [Green Version]
- Bus, S.A.; Lavery, L.A.; Monteiro-Soares, M.; Rasmussen, A.; Raspovic, A.; Sacco, I.C.; van Netten, J.J.; on behalf of the International Working Group on the Diabetic Foot. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2019 update). Diabetes/Metab. Res. Rev. 2020, 36, e3269. [Google Scholar] [CrossRef] [Green Version]
- Lipsky, B.A.; Senneville, É.; Abbas, Z.G.; Aragón-Sánchez, J.; Diggle, M.; Embil, J.M.; Kono, S.; Lavery, L.A.; Malone, M.; van Asten, S.A.; et al. Guidelines on the diagnosis and treatment of foot infection in persons with diabetes (IWGDF 2019 update). Diabetes/Metab. Res. Rev. 2020, 36 (Suppl. 1), e3280. [Google Scholar] [CrossRef] [Green Version]
- A Mayfield, J.; E Reiber, G.; Sanders, L.J.; Janisse, D.; Pogach, L.M. Preventive Foot Care in People with Diabetes. Diabetes Care 1998, 21, 2161–2177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golledge, J.; E Fernando, M.; Alahakoon, C.; Lazzarini, P.A.; de Stegge, W.B.A.; van Netten, J.J.; Bus, S.A. Efficacy of at home monitoring of foot temperature for risk reduction of diabetes-related foot ulcer: A meta-analysis. Diabetes/Metabol. Res. Rev. 2022, 38, e3549. [Google Scholar] [CrossRef]
- Smith-Strøm, H.; Iversen, M.M.; Graue, M.; Skeie, S.; Kirkevold, M. An integrated wound-care pathway, supported by telemedicine, and competent wound management—Essential in follow-up care of adults with diabetic foot ulcers. Int. J. Med. Inform. 2016, 94, 59–66. [Google Scholar] [CrossRef]
- Golledge, J.; Fernando, M.; Lazzarini, P.; Najafi, B.; Armstrong, D.G. The Potential Role of Sensors, Wearables and Telehealth in the Remote Management of Diabetes-Related Foot Disease. Sensors 2020, 20, 4527. [Google Scholar] [CrossRef] [PubMed]
- De Guzman, K.R.; Snoswell, C.L.; Taylor, M.L.; Gray, L.C.; Caffery, L.J. Economic Evaluations of Remote Patient Monitoring for Chronic Disease: A Systematic Review. Value Health 2022, 25, 897–913. [Google Scholar] [CrossRef]
- Malasinghe, L.P.; Ramzan, N.; Dahal, K. Remote patient monitoring: A comprehensive study. J. Ambient. Intell. Humaniz. Comput. 2019, 10, 57–76. [Google Scholar] [CrossRef] [Green Version]
- Peyroteo, M.; Ferreira, I.A.; Elvas, L.B.; Ferreira, J.C.; Lapão, L.V. Remote Monitoring Systems for Patients with Chronic Diseases in Primary Health Care: Systematic Review. JMIR mHealth uHealth 2021, 9, e28285. [Google Scholar] [CrossRef]
- Richardson, S.; Lawrence, K.; Schoenthaler, A.M.; Mann, D. A framework for digital health equity. NPJ Digit. Med. 2022, 5, 119. [Google Scholar] [CrossRef] [PubMed]
- Søndergaard, S.F.; Vestergaard, E.G.; Andersen, A.B.; Kolbæk, R.; Dahl, M.; Høgh, A. How patients with diabetic foot ulcers experience telemedicine solutions: A scoping review. Int. Wound J. 2022, 20, 1796–1810. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.L.; Miller, E. Remote Patient Monitoring in Diabetes: How to Acquire, Manage, and Use All of the Data. Diabetes Spectr. 2022, 35, 43–56. [Google Scholar] [CrossRef]
- Taylor, M.L.; E Thomas, E.; Snoswell, C.L.; Smith, A.C.; Caffery, L.J. Does remote patient monitoring reduce acute care use? A systematic review. BMJ Open 2021, 11, e040232. [Google Scholar] [CrossRef] [PubMed]
- Noah, B.; Keller, M.S.; Mosadeghi, S.; Stein, L.; Johl, S.; Delshad, S.; Tashjian, V.C.; Lew, D.; Kwan, J.T.; Jusufagic, A.; et al. Impact of remote patient monitoring on clinical outcomes: An updated meta-analysis of randomized controlled trials. NPJ Digit. Med. 2018, 1, 20172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Peña, M.T.; Fletcher, L.M.; Lal, L.; Swint, J.M.; Reneker, J.C. Economic evaluation and costs of remote patient monitoring for cardiovascular disease in the United States: A systematic review. Int. J. Technol. Assess. Health Care 2023, 39, e25. [Google Scholar] [CrossRef] [PubMed]
- American Heart Association. Using Remote Patient Monitoring Technologies for Better Cardiovascular Disease Outcomes: Guidance. American Heart Association. 2019. Available online: https://www.heart.org/-/media/files/about-us/policy-research/policy-positions/clinical-care/remote-patient-monitoring-guidance-2019.pdf (accessed on 18 June 2023).
- Najafi, B.; Chalifoux, C.B.; Everett, J.B.; Razjouyan, J.; A Brooks, E.; Armstrong, D.G. Cost effectiveness of smart insoles in preventing ulcer recurrence for people in diabetic foot remission. Wound Care Manag. 2018, 1, 1. [Google Scholar] [CrossRef] [Green Version]
- Abbott, C.A.; Chatwin, K.E.; Foden, P.; Hasan, A.N.; Sange, C.; Rajbhandari, S.M.; Reddy, P.N.; Vileikyte, L.; Bowling, F.L.; Boulton, A.J.M.; et al. Innovative intelligent insole system reduces diabetic foot ulcer recurrence at plantar sites: A prospective, randomised, proof-of-concept study. Lancet Digit. Health 2019, 1, e308–e318. [Google Scholar] [CrossRef] [PubMed]
- Brooks, E.; Burns, M.; Ma, R.; Scholten, H.J.; Becker, S.H. Remote Diabetic Foot Temperature Monitoring for Early Detection of Diabetic Foot Ulcers: A Cost-Effectiveness Analysis. Clin. Outcomes Res. 2021, 13, 873–881. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Holtz-Neiderer, K.; Wendel, C.; Mohler, M.J.; Kimbriel, H.R.; Lavery, L.A. Skin Temperature Monitoring Reduces the Risk for Diabetic Foot Ulceration in High-risk Patients. Am. J. Med. 2007, 120, 1042–1046. [Google Scholar] [CrossRef]
- Prevention of Amputation in Veterans Everywhere Program. 2022. Available online: https://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=9852#:~:text=PURPOSE-,This%20Veterans%20Health%20Administration%20(VHA)%20directive%20states%20policy%20and%20requirements,%C2%A7%207301(b) (accessed on 10 June 2023).
- Schaper, N.C.; Van Netten, J.J.; Apelqvist, J.; Bus, S.A.; Hinchliffe, R.J.; Lipsky, B.A.; IWGDF Editorial Board. Practical Guidelines on the prevention and management of diabetic foot disease (IWGDF 2019 update). Diabetes Metab. Res. Rev. 2020, 36 (Suppl. S1), e3266. [Google Scholar] [CrossRef] [Green Version]
- Frykberg, R.G.; Gordon, I.L.; Reyzelman, A.M.; Cazzell, S.M.; Fitzgerald, R.H.; Rothenberg, G.M.; Bloom, J.D.; Petersen, B.J.; Linders, D.R.; Nouvong, A.; et al. Feasibility and Efficacy of a Smart Mat Technology to Predict Development of Diabetic Plantar Ulcers. Diabetes Care 2017, 40, 973–980. [Google Scholar] [CrossRef] [Green Version]
- Gordon, I.L.; Rothenberg, G.M.; Lepow, B.D.; Petersen, B.J.; Linders, D.R.; Bloom, J.D.; Armstrong, D.G. Accuracy of a foot temperature monitoring mat for predicting diabetic foot ulcers in patients with recent wounds or partial foot amputation. Diabetes Res. Clin. Pract. 2020, 161, 108074. [Google Scholar] [CrossRef] [Green Version]
- Reyzelman, A.M.; Koelewyn, K.; Murphy, M.; Shen, X.; Yu, E.; Pillai, R.; Fu, J.; Scholten, H.J.; Ma, R. Continuous Temperature-Monitoring Socks for Home Use in Patients with Diabetes: Observational Study. J. Med. Internet Res. 2018, 20, e12460. [Google Scholar] [CrossRef] [Green Version]
- Reyzelman, A.M.; Shih, C.-D.; Tovmassian, G.; Nathan, M.; Ma, R.; Scholten, H.J.; Malhotra, K.; Armstrong, D.G. An Evaluation of Real-world Smart Sock–Based Temperature Monitoring Data as a Physiological Indicator of Early Diabetic Foot Injury: Case-Control Study. JMIR Form. Res. 2022, 6, e31870. [Google Scholar] [CrossRef] [PubMed]
- Lavery, L.A.; Petersen, B.J.; Linders, D.R.; Bloom, J.D.; Rothenberg, G.M.; Armstrong, D.G. Unilateral remote temperature monitoring to predict future ulceration for the diabetic foot in remission. BMJ Open Diabetes Res. Care 2019, 7, e000696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavery, L.A.; Higgins, K.R.; Lanctot, D.R.; Constantinides, G.P.; Zamorano, R.G.; Armstrong, D.G.; Athanasiou, K.A.; Agrawal, C.M. Home Monitoring of Foot Skin Temperatures to Prevent Ulceration. Diabetes Care 2004, 27, 2642–2647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavery, L.A.; Higgins, K.R.; Lanctot, D.R.; Constantinides, G.P.; Zamorano, R.G.; Athanasiou, K.A.; Armstrong, D.G.; Agrawal, C.M. Preventing Diabetic Foot Ulcer Recurrence in High-Risk Patients: Use of temperature monitoring as a self-assessment tool. Diabetes Care 2007, 30, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Scholten, H.J.; Shih, C.-D.; Ma, R.; Malhotra, K.; Reyzelman, A.M. Utilization of a Smart Sock for the Remote Monitoring of Patients with Peripheral Neuropathy: Cross-sectional Study of a Real-world Registry. JMIR Form. Res. 2022, 6, e32934. [Google Scholar] [CrossRef]
- Podimetrics—Revolutionize Diabetic Foot Care for Your Patients. Podimetrics. Available online: https://podimetrics.com/ (accessed on 26 June 2023).
- Isaac, A.L.; Swartz, T.D.; Miller, M.L.; Short, D.J.; Wilson, E.A.; Chaffo, J.L.; Watson, E.S.; Hu, H.; Petersen, B.J.; Bloom, J.D.; et al. Lower resource utilization for patients with healed diabetic foot ulcers during participation in a prevention program with foot temperature monitoring. BMJ Open Diabetes Res. Care 2020, 8, e001440. [Google Scholar] [CrossRef]
- Armstrong, D.G.; A Lavery, L.; Liswood, P.J.; Todd, W.F.; A Tredwell, J. Infrared Dermal Thermometry for the High-Risk Diabetic Foot. Phys. Ther. 1997, 77, 169–175. [Google Scholar] [CrossRef]
- Bus, S.A.; van Netten, J.J. A shift in priority in diabetic foot care and research: 75% of foot ulcers are preventable. Diabetes/Metabolism Res. Rev. 2016, 32, 195–200. [Google Scholar] [CrossRef] [Green Version]
- Chatwin, K.E.; Abbott, C.A.; Boulton, A.J.; Bowling, F.L.; Reeves, N. The role of foot pressure measurement in the prediction and prevention of diabetic foot ulceration—A comprehensive review. Diabetes/Metabolism Res. Rev. 2020, 36, e3258. [Google Scholar] [CrossRef] [PubMed]
- de Graaff, J.C.; Ubbink, D.T.; Van Der Spruit, J.A.; Lagarde, S.M.; Jacobs, M.J. Influence of peripheral arterial disease on capillary pressure in the foot. J. Vasc. Surg. 2003, 38, 1067–1074. [Google Scholar] [CrossRef]
- Najafi, B.; Ron, E.; Enriquez, A.; Marin, I.; Razjouyan, J.; Armstrong, D.G. Smarter Sole Survival: Will Neuropathic Patients at High Risk for Ulceration Use a Smart Insole-Based Foot Protection System? J. Diabetes Sci. Technol. 2017, 11, 702–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, J.D.; Salloum, M.; Button, A.; Giovinco, N.A.; Armstrong, D.G. How Can I Maintain My Patient with Diabetes and History of Foot Ulcer in Remission? Int. J. Low. Extremity Wounds 2014, 13, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Mills, J.L. Toward a Change in Syntax in Diabetic Foot Care: Prevention Equals Remission. J. Am. Podiatr. Med Assoc. 2013, 103, 161–162. [Google Scholar] [CrossRef] [Green Version]
- Zenunaj, G.; Lamberti, N.; Manfredini, F.; Traina, L.; Acciarri, P.; Bisogno, F.; Scian, S.; Serra, R.; Abatangelo, G.; Gasbarro, V. Infrared Thermography as a Diagnostic Tool for the Assessment of Patients with Symptomatic Peripheral Arterial Disease Undergoing Infrafemoral Endovascular Revascularisations. Diagnostics 2021, 11, 1701. [Google Scholar] [CrossRef]
- Papanas, N.; Papatheodorou, K.; Papazoglou, D.; Kotsiou, S.; Maltezos, E. Association between Foot Temperature and Sudomotor Dysfunction in Type 2 Diabetes. J. Diabetes Sci. Technol. 2010, 4, 803–807. [Google Scholar] [CrossRef] [Green Version]
- van Netten, J.J.; Prijs, M.; van Baal, J.G.; Liu, C.; van der Heijden, F.; Bus, S.A. Diagnostic Values for Skin Temperature Assessment to Detect Diabetes-Related Foot Complications. Diabetes Technol. Ther. 2014, 16, 714–721. [Google Scholar] [CrossRef] [Green Version]
- Kato, S.; Chmielewski, M.; Honda, H.; Pecoits-Filho, R.; Matsuo, S.; Yuzawa, Y.; Tranaeus, A.; Stenvinkel, P.; Lindholm, B. Aspects of Immune Dysfunction in End-stage Renal Disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1526–1533. [Google Scholar] [CrossRef] [Green Version]
- Liden, B.A.; Hartman, J.F.; Wright, M.L. An Algorithm for the Management of Lower Extremity Diabetic Wounds Based on UT Wound Classification Using a Human Acellular Dermal Regenerative Tissue Matrix. Presented at Sheridan Memorial Hospital, Sheridan, WY, USA, 2015. Available online: https://www.yumpu.com/en/document/view/41177341/brock-linden-sheridan-memorial-hospital (accessed on 16 July 2023).
- Moon, D.; Cao, N.; Martinez, B. Shoe and Bracing Considerations for the Insensate Foot: Shoe Considerations for Diabetic. Foot Phys. Med. Rehabilitation Clin. North Am. 2022, 33, 845–856. [Google Scholar] [CrossRef] [PubMed]
- Forsythe, R.O.; Apelqvist, J.; Boyko, E.J.; Fitridge, R.; Hong, J.P.; Katsanos, K.; Mills, J.L.; Nikol, S.; Reekers, J.; Venermo, M.; et al. Effectiveness of bedside investigations to diagnose peripheral artery disease among people with diabetes mellitus: A systematic review. Diabetes/Metabol. Res. Rev. 2020, 36, e3277. [Google Scholar] [CrossRef]
- A Bus, S.; de Stegge, W.B.A.; van Baal, J.G.; E Busch-Westbroek, T.; Nollet, F.; van Netten, J.J. Effectiveness of at-home skin temperature monitoring in reducing the incidence of foot ulcer recurrence in people with diabetes: A multicenter randomized controlled trial (DIATEMP). BMJ Open Diabetes Res. Care 2021, 9, e002392. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee 6. Glycemic Targets: Standards of Medical Care in Diabetes—2022. Diabetes Care 2022, 45 (Suppl. 1), S83–S96. [Google Scholar] [CrossRef] [PubMed]
- Bus, S.A. The Role of Pressure Offloading on Diabetic Foot Ulcer Healing and Prevention of Recurrence. Plast. Reconstr. Surg. 2016, 138, 179S–187S. [Google Scholar] [CrossRef]
- Wu, S.C.; Driver, V.R.; Wrobel, J.S.; Armstrong, D. G Foot ulcers in the diabetic patient, prevention and treatment. Vasc. Health Risk. Manag. 2007, 3, 65–76. [Google Scholar]
- Crews, R.T.; Shen, B.-J.; Campbell, L.; Lamont, P.J.; Boulton, A.J.; Peyrot, M.; Kirsner, R.S.; Vileikyte, L. Role and Determinants of Adherence to Off-loading in Diabetic Foot Ulcer Healing: A Prospective Investigation. Diabetes Care 2016, 39, 1371–1377. [Google Scholar] [CrossRef] [Green Version]
- Francia, P.; De Bellis, A.; Seghieri, G.; Tedeschi, A.; Iannone, G.; Anichini, R.; Gulisano, M. Continuous Movement Monitoring of Daily Living Activities for Prevention of Diabetic Foot Ulcer: A Review of Literature. Int. J. Prev. Med. 2019, 10, 22. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [Green Version]
- Cannata, F.; Vadalà, G.; Russo, F.; Papalia, R.; Napoli, N.; Pozzilli, P. Beneficial Effects of Physical Activity in Diabetic Patients. J. Funct. Morphol. Kinesiol. 2020, 5, 70. [Google Scholar] [CrossRef]
- Wachter, R. Should Hospitals Be More Like Airplanes? Backchannel 3 April 2015. Available online: https://medium.com/backchannel/should-hospitals-be-more-like-airplanes-5d6b9e2067ae (accessed on 31 March 2023).
- Shivers, J.P.; Mackowiak, L.; Anhalt, H.; Zisser, H. Turn It Off!: Diabetes Device Alarm Fatigue Considerations for the Present and the Future. J. Diabetes Sci. Technol. 2013, 7, 789–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ancker, J.S.; Edwards, A.; Nosal, S.; Hauser, D.; Mauer, E.; Kaushal, R.; the HITEC Investigators. Effects of workload, work complexity, and repeated alerts on alert fatigue in a clinical decision support system. BMC Med. Inform. Decis. Mak. 2017, 17, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreuzberger, D.; Kühl, N.; Hirschl, S. Machine Learning Operations (MLOps): Overview, Definition, and Architecture. arXiv 2022, arXiv:2205.02302. [Google Scholar] [CrossRef]
- Najafi, B.; Reeves, N.D.; Armstrong, D.G. Leveraging smart technologies to improve the management of diabetic foot ulcers and extend ulcer-free days in remission. Diabetes Metab. Res. Rev. 2020, 36, e3239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaly, I.; Iyengar, K.; Bahl, S.; Hughes, T.; Vaishya, R. Redefining diabetic foot disease management service during COVID-19 pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 833–838. [Google Scholar] [CrossRef]
- Mcguire, L.C. Remembering what the doctor said: Organization and adults’ memory for medical information. Exp. Aging Res. 1996, 22, 403–428. [Google Scholar] [CrossRef]
- Maluf, K.; Mueller, M. Comparison of physical activity and cumulative plantar tissue stress among subjects with and without diabetes mellitus and a history of recurrent plantar ulcers. Clin. Biomech. 2003, 18, 567–575. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Lavery, L.A.; Holtz-Neiderer, K.; Mohler, M.J.; Wendel, C.S.; Nixon, B.P.; Boulton, A.J. Variability in Activity May Precede Diabetic Foot Ulceration. Diabetes Care 2004, 27, 1980–1984. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.T.; Price, P.; Harding, K.G. The influence of diabetes and lower limb arterial disease on cutaneous foot perfusion. J. Vasc. Surg. 2006, 44, 770–775. [Google Scholar] [CrossRef] [Green Version]
- Ivey, F.M.; Hafer-Macko, C.E.; Ryan, A.S.; Macko, R.F. Impaired Leg Vasodilatory Function after Stroke: Impaired Leg Vasodilatory Function after Stroke: Adaptations with Treadmill Exercise Training. Stroke 2010, 41, 2913–2917. [Google Scholar] [CrossRef] [Green Version]
- Niemann, U.; Spiliopoulou, M.; Malanowski, J.; Kellersmann, J.; Szczepanski, T.; Klose, S.; Dedonaki, E.; Walter, I.; Ming, A.; Mertens, P.R. Plantar temperatures in stance position: A comparative study with healthy volunteers and diabetes patients diagnosed with sensoric neuropathy. Ebiomedicine 2020, 54, 102712. [Google Scholar] [CrossRef] [PubMed]
- Kessels, R.P. Patients’ memory for medical information. J. R. Soc. Med. 2003, 96, 219–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemaster, J.W.; Reiber, G.E.; Smith, D.G.; Heagerty, P.J.; Wallace, C. Daily weight-bearing activity does not increase the risk of diabetic foot ulcers. Med. Sci. Sports Exerc. 2003, 35, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Everything Should Be Made as Simple as Possible, But Not Simpler—Quote Investigator®. 13 May 2011. Available online: https://quoteinvestigator.com/2011/05/13/einstein-simple/ (accessed on 19 May 2023).
- E Reiber, G.; Vileikyte, L.; Boyko, E.J.; del Aguila, M.; Smith, D.G.; A Lavery, L.; Boulton, A.J. Causal pathways for incident lower-extremity ulcers in patients with diabetes from two settings. Diabetes Care 1999, 22, 157–162. [Google Scholar] [CrossRef]
- Ling, E.; Lepow, B.; Zhou, H.; Enriquez, A.; Mullen, A.; Najafi, B. The impact of diabetic foot ulcers and unilateral offloading footwear on gait in people with diabetes. Clin. Biomech. 2020, 73, 157–161. [Google Scholar] [CrossRef]
- Bus, S.A.; Maas, J.C.; Otterman, N.M. Lower-extremity dynamics of walking in neuropathic diabetic patients who wear a forefoot-offloading shoe. Clin. Biomech. 2017, 50, 21–26. [Google Scholar] [CrossRef]
- Wendland, D.; Kline, P.; Simmons, L.; Sinacore, D. The effect of exercise, physical activity, stepping characteristics, and loading on diabetic foot ulcer healing: A systematic review. Index Wounds 2023, 35, 9–17. [Google Scholar] [CrossRef]
- Rao, P.V.; Reddy, A.P.; Lu, X.; Dasari, S.; Krishnaprasad, A.; Biggs, E.; Roberts, C.T.; Nagalla, S.R. Proteomic Identification of Salivary Biomarkers of Type-2 Diabetes. J. Proteome Res. 2009, 8, 239–245. [Google Scholar] [CrossRef]
- Petersen, B.J.; Rothenberg, G.M.; Lakhani, P.J.; Zhou, M.; Linders, D.R.; Bloom, J.D.; Wood, K.A.; Armstrong, D.G. Ulcer metastasis? Anatomical locations of recurrence for patients in diabetic foot remission. J. Foot Ankle Res. 2020, 13, 1. [Google Scholar] [CrossRef]
- Csete, M.E.; Doyle, J.C. Reverse Engineering of Biological Complexity. Science 2002, 295, 1664–1669. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Solution | Podimetrics SmartMat™ | Siren Socks | Orpyx SI® Sensory Insole System |
|---|---|---|---|
| Form factor | Mat | Socks | Insole: custom or prefabricated |
| Data sampling | Once per day | All day | All day |
| Temperature monitoring | Yes | Yes | Yes |
| Pressure monitoring | No | No | Yes |
| Activity monitoring | No | No | Yes |
| Group | Definition | Risk Level | RPM Recommendation |
|---|---|---|---|
| IWGDF Patient Risk Levels | |||
| 0 | No LOPS *, no PAD *, no FD * | Very low | Not required |
| 1 | LOPS + PAD | Low | In the presence of LOPS |
| 2 | LOPS + PAD, or LOPS + FD, or PAD + FD | Moderate | With history of previous (re-epithelialized) foot ulcer |
| 3 | LOPS or PAD with one or more of: (1) History of foot ulcer; (2) major or minor LEA *; and (3) ESRD * | High | With history of previous (re-epithelialized) foot ulcer |
| PAVE Patient Risk Levels | |||
| 0 | No sensory loss, diminished circulation, ulceration, or amputation | Normal | Not required |
| 1 | No sensory loss, diminished circulation, ulceration, or amputation, but any of the following: (1) FD; (2) Minor foot infection; (3) Minor diminution of circulation | Low | Not required |
| 2 | Sensory loss and may have: (1) Diminished circulation (absent or loss of protective sensation); (2) FD or minor foot infection and diagnosis of diabetes | Medium | With findings suggestive of LOPS, especially if concurrent foot deformity or poor circulation |
| 3 | PN + sensory loss and may have diminished circulation, FD, minor foot infection and any of: (1) ulcer or history of prior ulcer; (2) Severe PAD; (3) Charcot + FD; and (4) chronic kidney disease | High | With history of previous (re-epithelialized) foot ulcer |
| Patient History/Clinical Presentation | Physical Examination |
|---|---|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minty, E.; Bray, E.; Bachus, C.B.; Everett, B.; Smith, K.M.; Matijevich, E.; Hajizadeh, M.; Armstrong, D.G.; Liden, B. Preventative Sensor-Based Remote Monitoring of the Diabetic Foot in Clinical Practice. Sensors 2023, 23, 6712. https://doi.org/10.3390/s23156712
Minty E, Bray E, Bachus CB, Everett B, Smith KM, Matijevich E, Hajizadeh M, Armstrong DG, Liden B. Preventative Sensor-Based Remote Monitoring of the Diabetic Foot in Clinical Practice. Sensors. 2023; 23(15):6712. https://doi.org/10.3390/s23156712
Chicago/Turabian StyleMinty, Evan, Emily Bray, Courtney B. Bachus, Breanne Everett, Karen M. Smith, Emily Matijevich, Maryam Hajizadeh, David G. Armstrong, and Brock Liden. 2023. "Preventative Sensor-Based Remote Monitoring of the Diabetic Foot in Clinical Practice" Sensors 23, no. 15: 6712. https://doi.org/10.3390/s23156712