
Correlates of Person-Specific Rates of Change in Sensor-Derived Physical Activity Metrics of Daily Living in the Rush Memory and Aging Project
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessment of Total Daily Physical Activity
2.3. Other Covariates
2.3.1. Demographics
2.3.2. Sensor Metrics
2.3.3. Motor Function
2.3.4. Self-Reported Activities
2.3.5. Cognitive Function
2.3.6. Chronic Health Conditions
2.3.7. Psychosocial Factors
2.4. Statistical Analysis
3. Results
3.1. Baseline Description of the Analytic Cohort
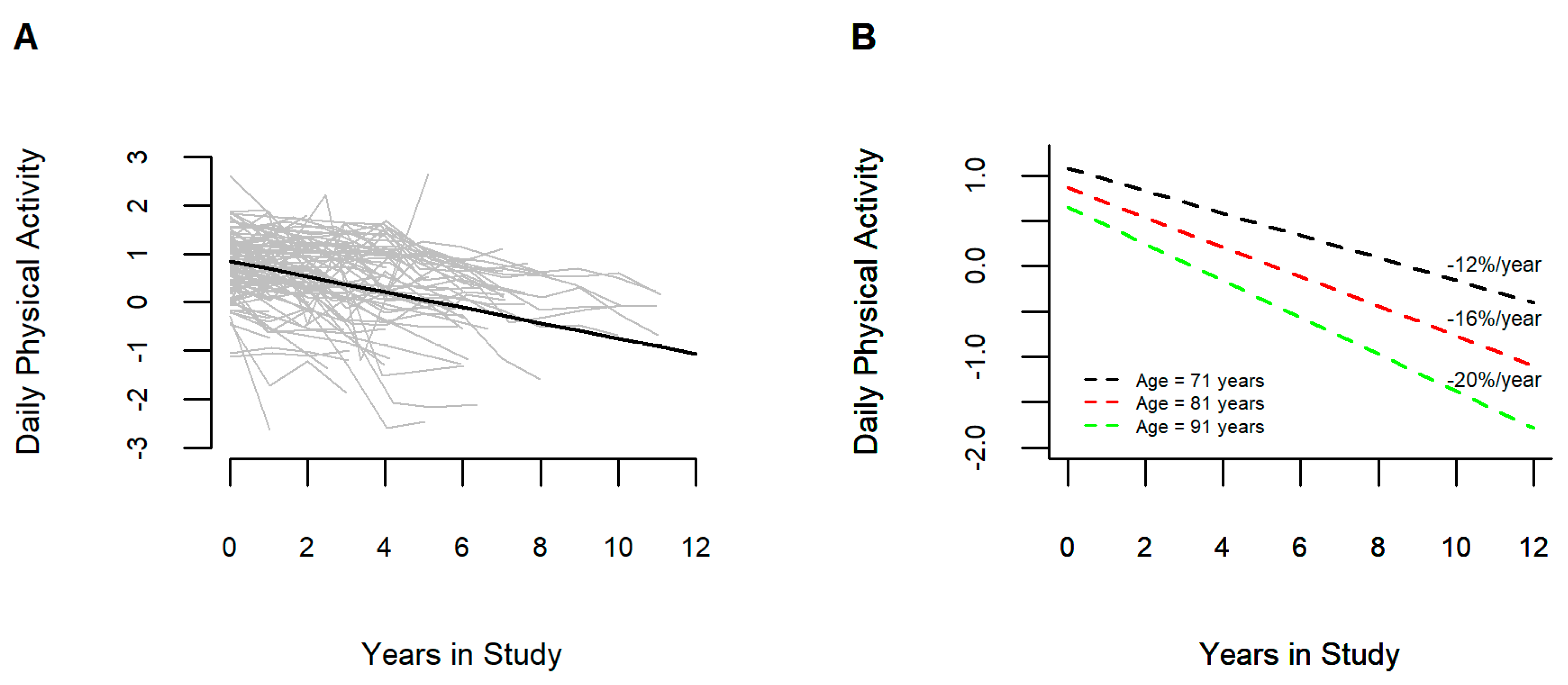
3.2. Annual Rate of Change in Total Daily Physical Activity
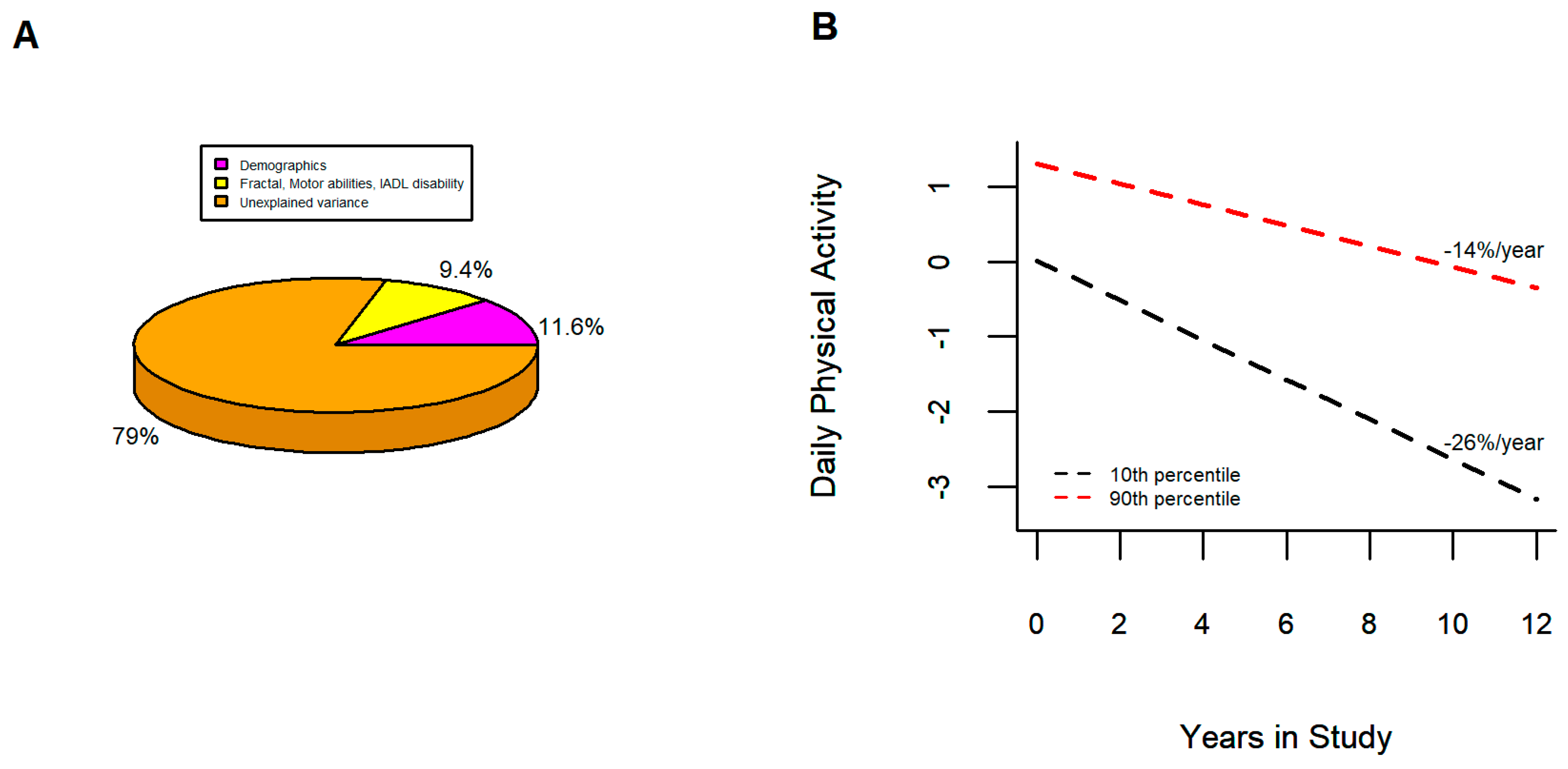
3.3. Correlates of Annual Rate of Change in Total Daily Physical Activity
4. Discussion
4.1. Novel Features of the Current Study
4.2. Person-Specific Decline of Total Daily Physical Activity
4.3. Correlates of Declining of Total Daily Physical Activity
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Administration on Aging. Administration on Aging. A profile of older Americans: 2016. In Services USDoHaH; Department of Health and Human Services: Washington, DC, USA, 2016. [Google Scholar]
- López-Ortiz, S.; Lista, S.; Valenzuela, P.L.; Pinto-Fraga, J.; Carmona, R.; Caraci, F.; Caruso, G.; Toschi, N.; Emanuele, E.; Gabelle, A.; et al. Effects of physical activity and exercise interventions on Alzheimer’s disease: An umbrella review of existing meta-analyses. J. Neurol. 2023, 270, 711–725. [Google Scholar] [CrossRef]
- Physical Activity Guidelines Advisory Committee. 2018 Physical activity guidelines advisory committee scientific report. In Services DoHaH; Department of Health and Human Services: Washington, DC, USA, 2018. [Google Scholar]
- Dong, L.; Block, G.; Mandel, S. Activities Contributing to Total Energy Expenditure in the United States: Results from the NHAPS Study. Int. J. Behav. Nutr. Phys. Act. 2004, 1, 4. [Google Scholar] [CrossRef] [PubMed]
- Uddin, M.Z.; Khaksar, W.; Torresen, J. Ambient Sensors for Elderly Care and Independent Living: A Survey. Sensors 2018, 18, 2027. [Google Scholar] [CrossRef] [PubMed]
- Lowe, S.A.; Ólaighin, G. Monitoring human health behaviour in one’s living environment: A technological review. Med. Eng. Phys. 2014, 36, 147–168. [Google Scholar] [CrossRef] [PubMed]
- Rast, F.M.; Labruyère, R. Systematic review on the application of wearable inertial sensors to quantify everyday life motor activity in people with mobility impairments. J. Neuroeng. Rehabil. 2020, 17, 148. [Google Scholar] [CrossRef]
- Buchman, A.S.; Wilson, R.S.; Yu, L.; James, B.D.; Boyle, P.A.; Bennett, D.A. Total daily activity declines more rapidly with increasing age in older adults. Arch. Gerontol. Geriatr. 2014, 58, 74–79. [Google Scholar] [CrossRef]
- Smith, L.; Gardner, B.; Fisher, A.; Hamer, M. Patterns and correlates of physical activity behaviour over 10 years in older adults: Prospective analyses from the English Longitudinal Study of Ageing. BMJ Open 2015, 5, e007423. [Google Scholar] [CrossRef]
- Clarke, C.L.; Sniehotta, F.F.; Vadiveloo, T.; Argo, I.S.; Donnan, P.T.; McMurdo, M.E.T.; Witham, M.D. Factors associated with change in objectively measured physical activity in older people—Data from the physical activity cohort Scotland study. BMC Geriatr. 2017, 17, 180. [Google Scholar] [CrossRef]
- Boyle, P.A.; Yu, L.; Wilson, R.S.; Leurgans, S.E.; Schneider, J.A.; Bennett, D.A. Person-specific contribution of neuropathologies to cognitive loss in old age. Ann. Neurol. 2018, 83, 74–83. [Google Scholar] [CrossRef]
- Buchman, A.S.; Yu, L.; Oveisgharan, S.; Farfel, J.M.; Schneider, J.A.; Bennett, D.A.A. Person-specific contributions of brain pathologies to progressive parkinsonism in older adults. J. Gerontol. Biol. Sci. Med. Sci. 2020, 76, 615–621. [Google Scholar] [CrossRef]
- Volders, E.; de Groot, R.H.M.; Bolman, C.A.W.; Lechner, L. The longitudinal associations between change in physical activity and cognitive functioning in older adults with chronic illness(es). BMC Geriatr. 2021, 21, 478. [Google Scholar] [CrossRef] [PubMed]
- Funaki, K.; Adachi, T.; Kameshima, M.; Fujiyama, H.; Iritani, N.; Tanaka, C.; Sakui, D.; Hara, Y.; Sugiura, H.; Yamada, S. Factors Associated with Changes in Objectively Measured Moderate to Vigorous Physical Activity in Patients after Percutaneous Coronary Intervention: A Prospective Cohort Study. J. Phys. Act. Health 2023, 20, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.A.; Buchman, A.S.; Boyle, P.A.; Barnes, L.L.; Wilson, R.S.; Schneider, J.A. Religious Orders Study and Rush Memory and Aging Project. J. Alzheimer’s Dis. 2018, 64, S161–S189. [Google Scholar] [CrossRef] [PubMed]
- Dawe, R.J.; Leurgans, S.E.; Yang, J.; Bennett, J.M.; Hausdorff, J.M.; Lim, A.S.; Gaiteri, C.; Bennett, D.A.; Buchman, A.S. Association between Quantitative Gait and Balance Measures and Total Daily Physical Activity in Community-Dwelling Older Adults. J. Gerontol. Biol. Sci. Med. Sci. 2017, 73, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Lim, A.; Yu, L.; Costa, M.D.; Buchman, A.S.; Bennett, D.A.; Leurgans, S.E.; Saper, C.B. Quantification of the Fragmentation of Rest-Activity Patterns in Elderly Individuals using a State Transition Analysis. Sleep 2011, 34, 1569–1581. [Google Scholar] [CrossRef]
- Li, P.; Lim, A.S.P.; Gao, L.; Hu, C.; Yu, L.; Bennett, D.A.; Buchman, A.S.; Hu, K. More random motor activity fluctuations predict incident frailty, disability, and mortality. Sci. Transl. Med. 2019, 11, 1977. [Google Scholar] [CrossRef]
- Li, P.; Yu, L.; Yang, J.; Lo, M.-T.; Hu, C.; Buchman, A.S.; Bennett, D.A.; Hu, K. Interaction between the progression of Alzheimer’s disease and fractal degradation. Neurobiol. Aging 2019, 83, 21–30. [Google Scholar] [CrossRef]
- Li, P.; Yu, L.; Lim, A.S.; Buchman, A.S.; Scheer, F.A.; Shea, S.A.; Schneider, J.A.; Bennett, D.A.; Hu, K. Fractal regulation and incident Alzheimer’s disease in elderly individuals. Alzheimer’s Dement. 2018, 14, 1114–1125. [Google Scholar] [CrossRef]
- Hausdorff, J.M. Gait dynamics in Parkinson’s disease: Common and distinct behavior among stride length, gait variability, and fractal-like scaling. Chaos 2009, 19, 026113. [Google Scholar] [CrossRef]
- Peng, C.K.; Havlin, S.; Stanley, H.E.; Goldberger, A.L. Quantification of scaling exponents and crossover phenomena in nonstationary heartbeat time series. Chaos 1995, 5, 82–87. [Google Scholar] [CrossRef]
- Herman, T.; Giladi, N.; Gurevich, T.; Hausdorff, J.M. Gait instability and fractal dynamics of older adults with a “cautious” gait: Why do certain older adults walk fearfully? Gait Posture 2005, 21, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.S.; Wang, T.; Yu, L.; Leurgans, S.E.; Schneider, J.A.; Bennett, D.A. Brain pathologies are associated with both the rate and variability of declining motor function in older adults. Acta Neuropathol. 2020, 140, 587–589. [Google Scholar] [CrossRef] [PubMed]
- Zammit, A.R.; Yu, L.; Petyuk, V.; Schneider, J.A.; De Jager, P.L.; Klein, H.-U.; Bennett, D.A.; Buchman, A.S. Cortical Proteins and Individual Differences in Cognitive Resilience in Older Adults. Neurology 2022, 98, e1304–e1314. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.S.; Wilson, R.S.; Shulman, J.M.; Leurgans, S.E.; Schneider, J.A.; Bennett, D.A. Parkinsonism in Older Adults and Its Association with Adverse Health Outcomes and Neuropathology. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 549–556. [Google Scholar] [CrossRef]
- Bennett, D.A.; Shannon, K.M.; Beckett, L.A.; Goetz, C.G.; Wilson, R.S. Metric properties of nurses’ ratings of parkinsonian signs with a modified Unified Parkinson’s Disease Rating Scale. Neurology 1997, 49, 1580–1587. [Google Scholar] [CrossRef]
- Buchman, A.S.; Boyle, P.A.; Wilson, R.S.; Bienias, J.L.; Bennett, D.A. Physical activity and motor decline in older persons. Muscle Nerve 2007, 35, 354–362. [Google Scholar] [CrossRef]
- Buchman, A.S.; Boyle, P.A.; Wilson, R.S.; Fleischman, D.A.; Leurgans, S.; Bennett, D.A. Association between late-life social activity and motor decline in older adults. Arch. Intern. Med. 2009, 169, 1139–1146. [Google Scholar] [CrossRef]
- Wilson, R.S.; Barnes, L.L.; Krueger, K.R.; Hoganson, G.; Bienias, J.L.; Bennett, D.A. Early and late life cognitive activity and cognitive systems in old age. J. Int. Neuropsychol. Soc. 2005, 11, 400–407. [Google Scholar] [CrossRef]
- Bennett, D.A.; Schneider, J.A.; Buchman, A.S.; Mendes de Leon, C.; Bienias, J.L.; Wilson, R.S. The Rush Memory and Aging Project: Study design and baseline characteristics of the study cohort. Neuroepidemiology 2005, 25, 163–175. [Google Scholar] [CrossRef]
- Rosow, I.; Breslau, N. A Guttman health scale for the aged. J. Gerontol. 1966, 21, 556–559. [Google Scholar] [CrossRef]
- Katz, S.; Akpom, C.A. A measure of primary sociobiological functions. Int. J. Health Serv. 1976, 6, 493–508. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S.; Boyle, P.A.; Yu, L.; Segawa, E.; Sytsma, J.; Bennett, D.A. Conscientiousness, dementia related pathology, and trajectories of cognitive aging. Psychol. Aging 2015, 30, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S.; Beckett, L.A.; Barnes, L.L.; Schneider, J.A.; Bach, J.; Evans, D.A.; Bennett, D.A. Individual differences in rates of change in cognitive abilities of older persons. Psychol. Aging 2002, 17, 179–193. [Google Scholar] [CrossRef]
- Buchman, A.S.; Wilson, R.S.; Bienias, J.L.; Shah, R.C.; Evans, D.A.; Bennett, D.A. Change in body mass index and risk of incident Alzheimer disease. Neurology 2005, 65, 892–897. [Google Scholar] [CrossRef]
- Boyle, P.A.; Wilson, R.S.; Aggarwal, N.T.; Arvanitakis, Z.; Kelly, J.; Bienias, J.L.; Bennett, D.A. Parkinsonian signs in subjects with mild cognitive impairment. Neurology 2005, 65, 1901–1906. [Google Scholar] [CrossRef]
- Wilson, R.S.; Schneider, J.A.; Boyle, P.A.; Arnold, S.E.; Tang, Y.; Bennett, D.A. Chronic distress and incidence of mild cognitive impairment. Neurology 2007, 68, 2085–2092. [Google Scholar] [CrossRef]
- Wilson, R.S.; Krueger, K.R.; Arnold, S.E.; Schneider, J.A.; Kelly, J.F.; Barnes, L.L.; Tang, Y.; Bennett, D.A. Loneliness and risk of Alzheimer disease. Arch. Gen. Psychiatry 2007, 64, 234–240. [Google Scholar] [CrossRef]
- Buchman, A.S.; Boyle, P.A.; Wilson, R.S.; Leurgans, S.E.; Arnold, S.E.; Bennett, D.A. Neuroticism, extraversion, and motor function in community-dwelling older persons. Am. J. Geriatr. Psychiatry 2013, 21, 145–154. [Google Scholar] [CrossRef]
- Boyle, P.A.; Buchman, A.S.; Wilson, R.S.; Yu, L.; Schneider, J.A.; Bennett, D.A. Effect of purpose in life on the relation between Alzheimer disease pathologic changes on cognitive function in advanced age. Arch. Gen. Psychiatry 2012, 69, 499–505. [Google Scholar] [CrossRef]
- Boyle, P.A.; Wang, T.; Yu, L.; Wilson, R.S.; Dawe, R.; Arfanakis, K.; Schneider, J.A.; Bennett, D.A. To what degree is late life cognitive decline driven by age-related neuropathologies? Brain 2021, 144, 2166–2175. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.S.; Dawe, R.J.; Leurgans, S.E.; A Curran, T.; Truty, T.; Yu, L.; Barnes, L.L.; Hausdorff, J.M.; Bennett, D.A. Different combinations of mobility metrics derived from a wearable sensor are associated with distinct health outcomes in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 75, 1176–1183. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.M.; Baker, K.; Jones, D.; Burn, D.; Granat, M.H.; Rochester, L. The pattern of habitual sedentary behavior is different in advanced Parkinson’s disease. Mov. Disord. 2010, 25, 2114–2120. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.S.; Dawe, R.J.; Yu, L.; Lim, A.; Wilson, R.S.; Schneider, J.A.; Bennett, D.A. Brain Pathology Is Related to Total Daily Physical Activity in Older Adults. Neurology 2018, 90, e1911–e1919. [Google Scholar] [CrossRef]
- Wilson, R.S.; Wang, T.; Yu, L.; Bennett, D.A.; Boyle, P.A. Normative Cognitive Decline in Old Age. Ann. Neurol. 2020, 87, 816–829. [Google Scholar] [CrossRef]
- Oveisgharan, S.; Dawe, R.J.; Leurgans, S.E.; Yu, L.; Schneider, J.A.; Bennett, D.A.; Buchman, A.S. Total daily physical activity, brain pathologies, and parkinsonism in older adults. PLoS ONE 2020, 15, e0232404. [Google Scholar] [CrossRef]
- Buchman, A.S.; Yu, L.; Wilson, R.S.; Lim, A.; Dawe, R.J.; Gaiteri, C.; Leurgans, S.E.; Schneider, J.A.; Bennett, D.A. Physical activity, common brain pathologies, and cognition in community-dwelling older adults. Neurology 2019, 92, e811–e822. [Google Scholar] [CrossRef]
- Fleischman, D.A.; Yang, J.; Arfanakis, K.; Arvanitakis, Z.; Leurgans, S.E.; Turner, A.D.; Barnes, L.L.; Bennett, D.A.; Buchman, A.S. Physical activity, motor function, and white matter hyperintensity burden in healthy older adults. Neurology 2015, 84, 1294–1300. [Google Scholar] [CrossRef]
- Buchman, A.S.; Yu, L.; Boyle, P.A.; Shah, R.C.; Bennett, D.A. Total Daily Physical Activity and Longevity in Old Age. Arch. Intern Med. 2012, 172, 444–446. [Google Scholar] [CrossRef]
- Shah, R.; Buchman, A.; Leurgans, S.; Boyle, P.; Bennett, D. Association of total daily physical activity with disability in community-dwelling older persons: A prospective cohort study. BMC Geriatr. 2012, 12, 63. [Google Scholar] [CrossRef]
- Buchman, A.S.; Boyle, P.A.; Yu, L.; Shah, R.C.; Wilson, R.S.; Bennett, D.A. Total daily physical activity and the risk of AD and cognitive decline in older adults. Neurology 2012, 78, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Brand, Y.E.; Schwartz, D.; Gazit, E.; Buchman, A.S.; Gilad-Bachrach, R.; Hausdorff, J.M. Gait Detection from a Wrist-Worn Sensor Using Machine Learning Methods: A Daily Living Study in Older Adults and People with Parkinson’s Disease. Sensors 2022, 22, 7094. [Google Scholar] [CrossRef] [PubMed]
- West, B.J. The Fractal Tapestry of Life: A Review of Fractal Physiology. Nonlinear Dyn. Psychol. Life Sci. 2021, 25, 261–296. [Google Scholar]
- Gow, B.J.; Hausdorff, J.M.; Manor, B.; Lipsitz, L.A.; Macklin, E.A.; Bonato, P.; Novak, V.; Peng, C.-K.; Ahn, A.C.; Wayne, P.M. Can Tai Chi training impact fractal stride time dynamics, an index of gait health, in older adults? Cross-sectional and randomized trial studies. PLoS ONE 2017, 12, e0186212. [Google Scholar] [CrossRef] [PubMed]
- Giraldo, B.F.; Pericas, M.F.; Schroeder, R.; Voss, A. Respiratory Sinus Arrhythmia Quantified with Linear and Non-Linear Techniques to Classify Dilated and Ischemic Cardiomyopathy. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2018, 2018, 4860–4863. [Google Scholar] [CrossRef]
- Yineng, Z.; Xingming, G. Identification of chronic heart failure using linear and nonlinear analysis of heart sound. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2017, 2017, 4586–4589. [Google Scholar] [CrossRef]
- Lau, Z.J.; Pham, T.; Chen, S.H.A.; Makowski, D. Brain entropy, fractal dimensions and predictability: A review of complexity measures for EEG in healthy and neuropsychiatric populations. Eur. J. Neurosci. 2022, 56, 5047–5069. [Google Scholar] [CrossRef]
- Hausdorff, J.M. Gait dynamics, fractals and falls: Finding meaning in the stride-to-stride fluctuations of human walking. Hum. Mov. Sci. 2007, 26, 555–589. [Google Scholar] [CrossRef]
- Valenza, G.; Wendt, H.; Kiyono, K.; Hayano, J.; Watanabe, E.; Yamamoto, Y.; Abry, P.; Barbieri, R. Mortality Prediction in Severe Congestive Heart Failure Patients with Multifractal Point-Process Modeling of Heartbeat Dynamics. IEEE Trans. Biomed. Eng. 2018, 65, 2345–2354. [Google Scholar] [CrossRef]
- Peng, C.-K.; Mietus, J.E.; Liu, Y.; Lee, C.; Hausdorff, J.M.; Stanley, H.; Goldberger, A.L.; Lipsitz, L.A. Quantifying fractal dynamics of human respiration: Age and gender effects. Ann. Biomed. Eng. 2002, 30, 683–692. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.; Hausdorff, J.M.; Ivanov, P.; Peng, C.K.; Stanley, H.E. Fractal dynamics in physiology: Alterations with disease and aging. Proc. Natl. Acad. Sci. USA 2002, 99 (Suppl. S1), 2466–2472. [Google Scholar] [CrossRef] [PubMed]
- Echeverría, J.C.; Infante, O.; Pérez-Grovas, H.; González, H.; José, M.V.; Lerma, C. Effects of Orthostatism and Hemodialysis on Mean Heart Period and Fractal Heart Rate Properties of Chronic Renal Failure Patients. Artif. Organs 2017, 41, 1026–1034. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.; Ivanov, P.; Chen, Z.; Hilton, M.F.; Stanley, H.E.; Shea, S.A. Non-random fluctuations and multi-scale dynamics regulation of human activity. Physica A 2004, 337, 307–318. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.; Scheer, F.A.; Ivanov, P.; Buijs, R.M.; Shea, S.A. The suprachiasmatic nucleus functions beyond circadian rhythm generation. Neuroscience 2007, 149, 508–517. [Google Scholar] [CrossRef]
- Li, P.; To, T.; Chiang, W.Y.; Escobar, C.; Buijs, R.M.; Hu, K. Fractal Regulation in Temporal Activity Fluctuations: A Biomarker for Circadian Control and Beyond. JSM Biomark. 2017, 3, 1008. [Google Scholar]
- Buchman, A.S.; Bennett, D.A. Mixed Neuropathologies, Neural Motor Resilience and Target Discovery for Therapies of Late-Life Motor Impairment. Front. Hum. Neurosci. 2022, 16, 853330. [Google Scholar] [CrossRef]
- Bennett, D.A. Mixed pathologies and neural reserve: Implications of complexity for Alzheimer disease drug discovery. PLoS Med. 2017, 14, e1002256. [Google Scholar] [CrossRef]
- Mostafavi, S.; Gaiteri, C.; Sullivan, S.E.; White, C.C.; Tasaki, S.; Xu, J.; Taga, M.; Klein, H.-U.; Patrick, E.; Komashko, V.; et al. A molecular network of the aging human brain provides insights into the pathology and cognitive decline of Alzheimer’s disease. Nat. Neurosci. 2018, 21, 811–819. [Google Scholar] [CrossRef]
- Yu, L.; Tasaki, S.; Schneider, J.A.; Arfanakis, K.; Duong, D.M.; Wingo, A.P.; Wingo, T.S.; Kearns, N.; Thatcher, G.R.J.; Seyfried, N.T.; et al. Cortical Proteins Associated with Cognitive Resilience in Community-Dwelling Older Persons. JAMA Psychiatry 2020, 77, 1172–1180. [Google Scholar] [CrossRef]
- Yu, L.; Petyuk, V.A.; Gaiteri, C.; Mostafavi, S.; Young-Pearse, T.; Shah, R.C.; Buchman, A.S.; Schneider, J.A.; Piehowski, P.D.; Sontag, R.L.; et al. Targeted brain proteomics uncover multiple pathways to Alzheimer’s dementia. Ann. Neurol. 2018, 84, 78–88. [Google Scholar] [CrossRef]
- Buchman, A.S.; Yu, L.; Oveisgharan, S.; Petyuk, V.A.; Tasaki, S.; Gaiteri, C.; Wilson, R.S.; Grodstein, F.; Schneider, J.A.; Klein, H.-U.; et al. Cortical proteins may provide motor resilience in older adults. Sci. Rep. 2021, 11, 11311. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.H. The limitations of risk factors as prognostic tools. N. Engl. J. Med. 2006, 355, 2615–2617. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Covariate Groups | Variable at Baseline | Mean (SD) Median (IQR) |
|---|---|---|
| Demographics | Age (years) | 80.9 (7.31) |
| Female sex | 76% | |
| Education (years) | 15.1 (3.00) | |
| Race | 5% | |
| Income (median level) | 8 (5, 9) | |
| Sensor metrics | Sleep fragmentation (0–1) | 0.03 (0.01) |
| Interdaily stability (0–1) | 0.52 (0.12) | |
| Intradaily variability (0–2) | 0.71 (0.19) | |
| Fractal alpha1 | 0.92 (0.06) | |
| Fractal alpha2 | 0.82 (0.10) | |
| Motor function | Motor abilities (scaled) | 1.02 (0.23) |
| Parkinsonism (0–100) | 7.00 (7.02) | |
| Self-report | Physical activities (h/week) | 2.7 (1, 4.8) |
| Social activities (0–5) | 2.7 (2.2, 3.0) | |
| Cognitive activities (0–5) | 3.1 (2.9, 3.6) | |
| Mobility disability (0–3) | 0 (0, 1) | |
| ADL disability (0–6) | 0 (0, 0) | |
| IADL disability (0–8) | 0 (0, 1) | |
| Cognitive function | Episodic memory (z-score) | 0.16 (0.74) |
| Visuospatial abilities (z-score) | 0.08 (0.84) | |
| Perceptual speed (z-score) | 0.05 (0.80) | |
| Semantic memory (z-score) | 0.13 (0.66) | |
| Working memory (z-score) | 0.03 (0.74) | |
| Chronic health | Body mass index | 27.3 (5.39) |
| Chronic medical conditions (0–7) | 1.0 (0, 2) | |
| Vascular risk factors (0–3) | 1 (1, 2) | |
| Vascular diseases (0–4) | 0 (0, 1) | |
| Psychosocial factors | Depressive symptoms (0–10) | 0 (0, 1) |
| Social network (0–9) | 6 (3, 9) | |
| Social isolation (1–5) | 2.0 (2.0, 2.4) | |
| Neuroticism (0–12) | 7 (5, 9) | |
| Purpose in life average score (1–5) | 3.7 (3.4, 4.0) |
| Group | Baseline Covariate × Time | Stage 1 Covariates Alone Estimate (S.E., p-Value) | Stage 2 Groups Covariates Together Estimate (S.E., p-Value) |
|---|---|---|---|
| Demographics | lag × age | −0.004 (0.001, <0.001) | −0.004 (0.001, <0.001) |
| lag × sex | 0.006 (0.010, 0.529) | 0.006 (0.010, 0.567) | |
| lag × education | 0.003 (0.001, 0.038) | 0.003 (0.002, 0.079) | |
| lag × race | −0.005 (0.020, 0.782) | −0.004 (0.020, 0.825) | |
| lag × income | 0.001 (0.002, 0.641) | 0.001 (0.002, 0.666) | |
| Sensor metrics | lag × sleep fragmentation | −0.899 (0.621, 0.148) | −1.049 (0.62, 0.095) |
| lag × interdaily stability | 0.041 (0.035, 0.243) | 0.065 (0.037, 0.078) | |
| lag × interdaily variability | 0.049 (0.023, 0.031) | −0.011 (0.056, 0.839) | |
| lag × alpha1 | −0.176 (0.075, 0.019) | −0.225 (0.174, 0.198) | |
| lag × alpha2 | −0.097 (0.046, 0.035) | −0.107 (0.052, 0.040) | |
| Motor function | lag × motor abilities | 0.092 (0.022, <0.001) | 0.077 (0.026, 0.003) |
| lag × global parkinsonism score | −0.003 (0.001, 0.002) | −0.001 (0.001, 0.284) | |
| Self-report activities | lag × physical activities | 0.001 (0.001, 0.587) | −0.001 (0.001, 0.571) |
| lag × social activities | 0.013 (0.008, 0.089) | −0.001 (0.008, 0.922) | |
| lag × cognitive activities | 0.025 (0.007, <0.001) | 0.021 (0.007, 0.004) | |
| lag × mobility disability | −0.014 (0.005, 0.002) | −0.005 (0.006, 0.349) | |
| lag × ADL disability | −0.012 (0.007, 0.101) | 0.006 (0.008, 0.452) | |
| lag × IADL disability | −0.016 (0.003, <0.001) | −0.014 (0.004, 0.002) | |
| Cognition | lag × episodic memory | 0.024 (0.007, <0.001) | 0.017 (0.008, 0.028) |
| lag × visuospatial ability | 0.006 (0.006, 0.271) | −0.005 (0.006, 0.447) | |
| lag × perceptual speed | 0.021 (0.006, <0.001) | 0.014 (0.008, 0.071) | |
| lag × semantic memory | 0.022 (0.008, 0.004) | 0.004 (0.010, 0.692) | |
| lag × working memory | 0.016 (0.006, 0.009) | 0.006 (0.007, 0.415) | |
| Chronic health | lag × BMI | 0.002 (0.001, 0.009) | −0.002 (0.001, 0.013) |
| lag × chronic medical | −0.011 (0.004, 0.011) | −0.012 (0.005, 0.014) | |
| lag × vascular diseases | 0.004 (0.007, 0.601) | 0.006 (0.007, 0.388) | |
| lag × vascular risk factors | −0.004 (0.005, 0.489) | 0.005 (0.006, 0.392) | |
| Psychosocial factors | lag × depressive symptoms | 0.000 (0.003, 0.987) | 0.001 (0.003, 0.742) |
| lag × social network | 0.000 (0.001, 0.897) | −0.000 (0.001, 0.945) | |
| lag × social isolation | 0.001 (0.007, 0.909) | 0.007 (0.009, 0.444) | |
| lag × neuroticism | 0.000 (0.001, 0.754) | 0.001 (0.001, 0.5529) | |
| lag × purpose in life | 0.021 (0.010, 0.044) | 0.029 (0.012, 0.016) |
| Model Term | Stage 3 Final Model | Only Independent Covariates + Demographics | ||
|---|---|---|---|---|
| Estimate | S.E., p-Value | Estimate | S.E., p-Value | |
| Time | −0.052 | 0.077, 0.495 | −0.129 | 0.047, 0.006 |
| Age | −0.008 | 0.003, 0.008 | −0.006 | 0.003, 0.031 |
| Sex | −0.064 | 0.041, 0.117 | −0.059 | 0.041, 0.152 |
| Education | −0.019 | 0.006, 0.002 | −0.021 | 0.006, <0.001 |
| Episodic memory | −0.006 | 0.027, 0.814 | ||
| Perceptual speed | 0.048 | 0.027, 0.081 | ||
| Sleep fragmentation | 15.013 | 2.524, <0.001 | ||
| Interdaily stability | 1.168 | 0.138, <0.001 | ||
| Fractal alpha2 | 1.641 | 0.176, <0.001 | 1.746 | 0.186, <0.001 |
| Motor abilities | 0.316 | 0.101, <0.002 | 0.413 | 0.103, <0.001 |
| Late life cognitive activities | −0.011 | 0.029, 0.699 | ||
| IADL disability | −0.052 | 0.016, 0.001 | −0.074 | 0.017, <0.001 |
| BMI | −0.000 | 0.003, 0.998 | ||
| Medical conditions | −0.069 | 0.017, 0.0000 | ||
| Purpose in life | 0.007 | 0.040, 0.867 | ||
| Lag× Age | −0.002 | 0.001, 0.002 | −0.002 | 0.001, 0.008 |
| Lag× Sex | 0.004 | 0.011, 0.698 | −0.004 | 0.010, 0.726 |
| Lag× Education | 0.001 | 0.002, 0.530 | 0.002 | 0.001, 0.111 |
| Lag× Episodic memory | 0.013 | 0.007, 0.071 | ||
| Lag× Perceptual speed | −0.003 | 0.007, 0.720 | ||
| Lag× Sleep fragmentation | −0.893 | 0.612, 0.145 | ||
| Lag× Interdaily stability | −0.034 | 0.036, 0.338 | ||
| Lag× Fractal alpha2 | −0.123 | 0.046, 0.008 | −0.123 | 0.046, 0.007 |
| Lag× Motor abilities | 0.063 | 0.026, 0.014 | 0.084 | 0.024, <0.001 |
| Lag× Late life cognitive activities | 0.011 | 0.008, 0.164 | ||
| Lag× IADL disability | −0.013 | 0.005, 0.008 | −0.013 | 0.005, 0.004 |
| Lag× BMI | −0.002 | 0.001, 0.077 | ||
| Lag× Medical conditions | −0.008 | 0.005, 0.066 | ||
| Lag× Purpose in life | −0.001 | 0.011, 0.941 | ||
| Covariates | Percentage of Variance | |
|---|---|---|
| All demographics | 11.6% | |
| All non-demographic | 9.4% | |
| Individual non-demographic | Minimum % | Maximum % |
| Fractal alpha 2 | 0.6% | 1.5% |
| Motor abilities | 3.8% | 8.9% |
| IADL disability | 1.8% | 6.2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buchman, A.S.; Wang, T.; Oveisgharan, S.; Zammit, A.R.; Yu, L.; Li, P.; Hu, K.; Hausdorff, J.M.; Lim, A.S.P.; Bennett, D.A. Correlates of Person-Specific Rates of Change in Sensor-Derived Physical Activity Metrics of Daily Living in the Rush Memory and Aging Project. Sensors 2023, 23, 4152. https://doi.org/10.3390/s23084152
Buchman AS, Wang T, Oveisgharan S, Zammit AR, Yu L, Li P, Hu K, Hausdorff JM, Lim ASP, Bennett DA. Correlates of Person-Specific Rates of Change in Sensor-Derived Physical Activity Metrics of Daily Living in the Rush Memory and Aging Project. Sensors. 2023; 23(8):4152. https://doi.org/10.3390/s23084152
Chicago/Turabian StyleBuchman, Aron S., Tianhao Wang, Shahram Oveisgharan, Andrea R. Zammit, Lei Yu, Peng Li, Kun Hu, Jeffrey M. Hausdorff, Andrew S. P. Lim, and David A. Bennett. 2023. "Correlates of Person-Specific Rates of Change in Sensor-Derived Physical Activity Metrics of Daily Living in the Rush Memory and Aging Project" Sensors 23, no. 8: 4152. https://doi.org/10.3390/s23084152