
Wearable Epileptic Seizure Prediction System Based on Machine Learning Techniques Using ECG, PPG and EEG Signals

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
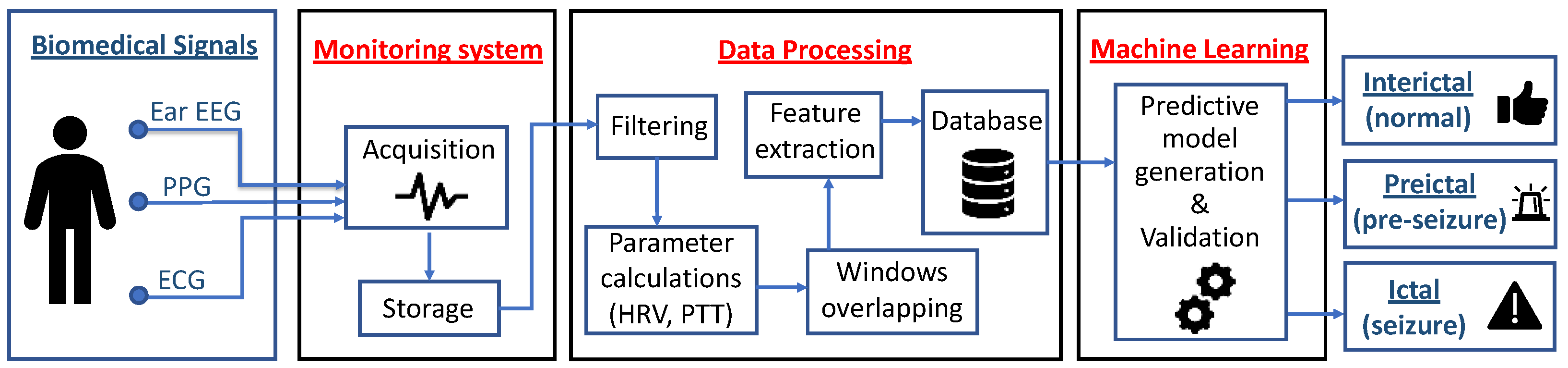
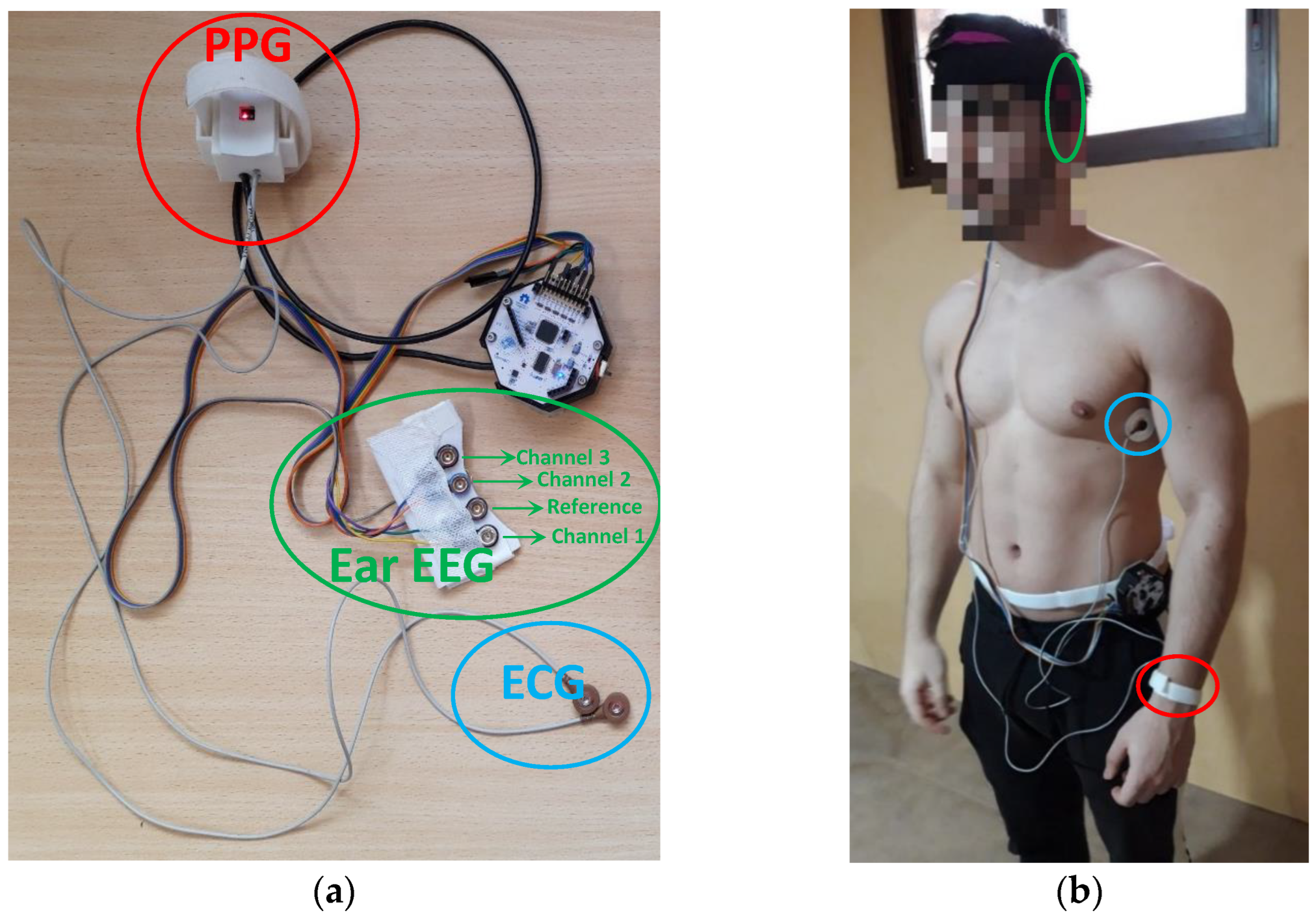
2.1. Monitoring System
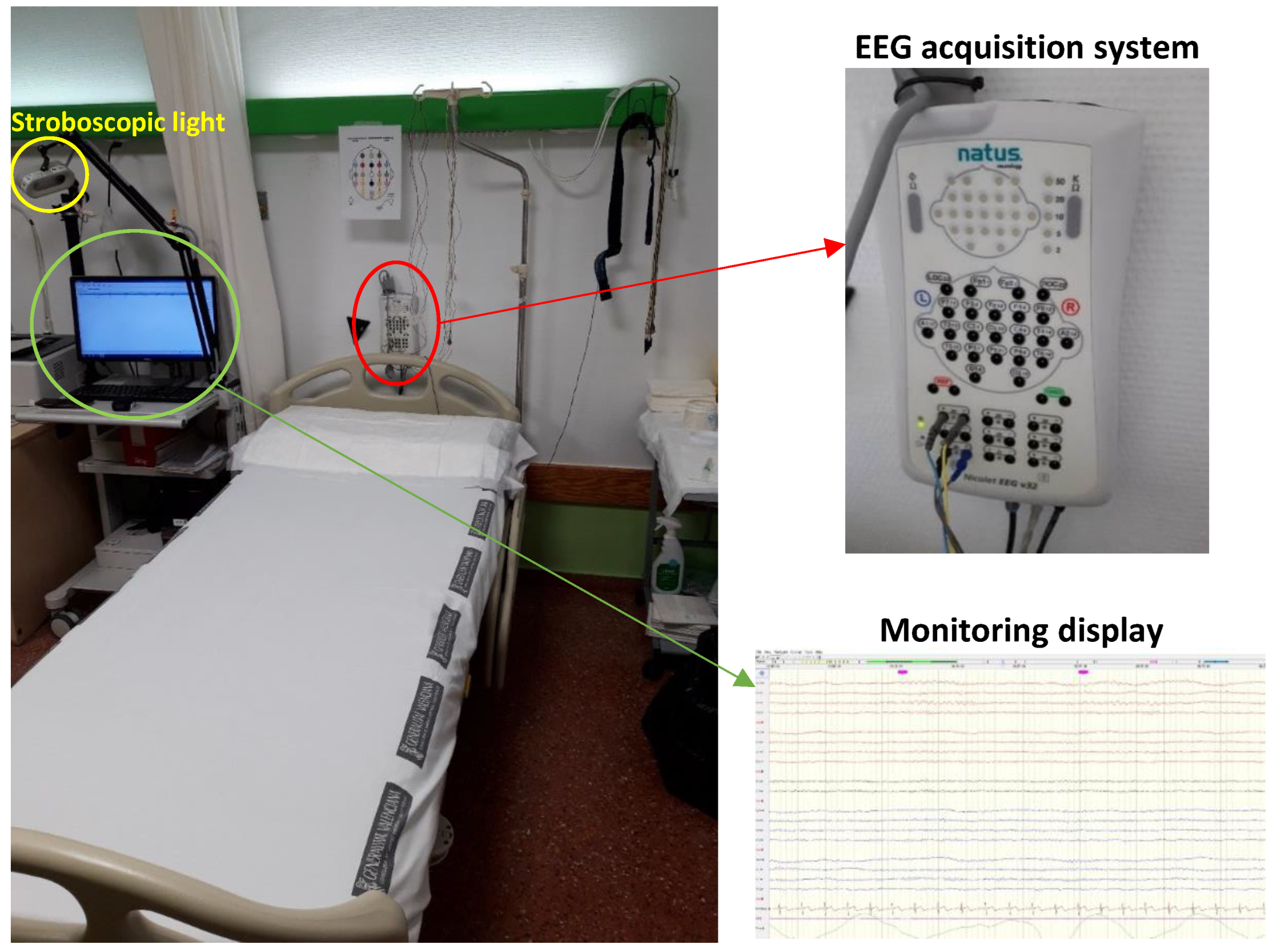
2.2. Experimentation Protocol in a Clinical Setting
- Open and close eyes (2 min): the user keeps his/her eyes open for 30 s and then closes them for 30 s. Finally, the user repeats it again.
- Strobe light (6 min): the user is subjected to 12 shots of lights flashing at a frequency of 2, 4, 6, 8, 10, 12, 14, 16, 18, 20, 25 and 30 Hz for 15 s with 15 s pauses between shots.
- Hyperventilation (1.5 min): The volunteer must hyperventilate, taking 15–20 breaths/min.
- Rest (2 min).
- Hyperventilation (1.5 min): The volunteer must hyperventilate, taking 15–20 breaths/min.
- Rest (2 min).
- Sleeping (20 min).
- Waking up (5 min).
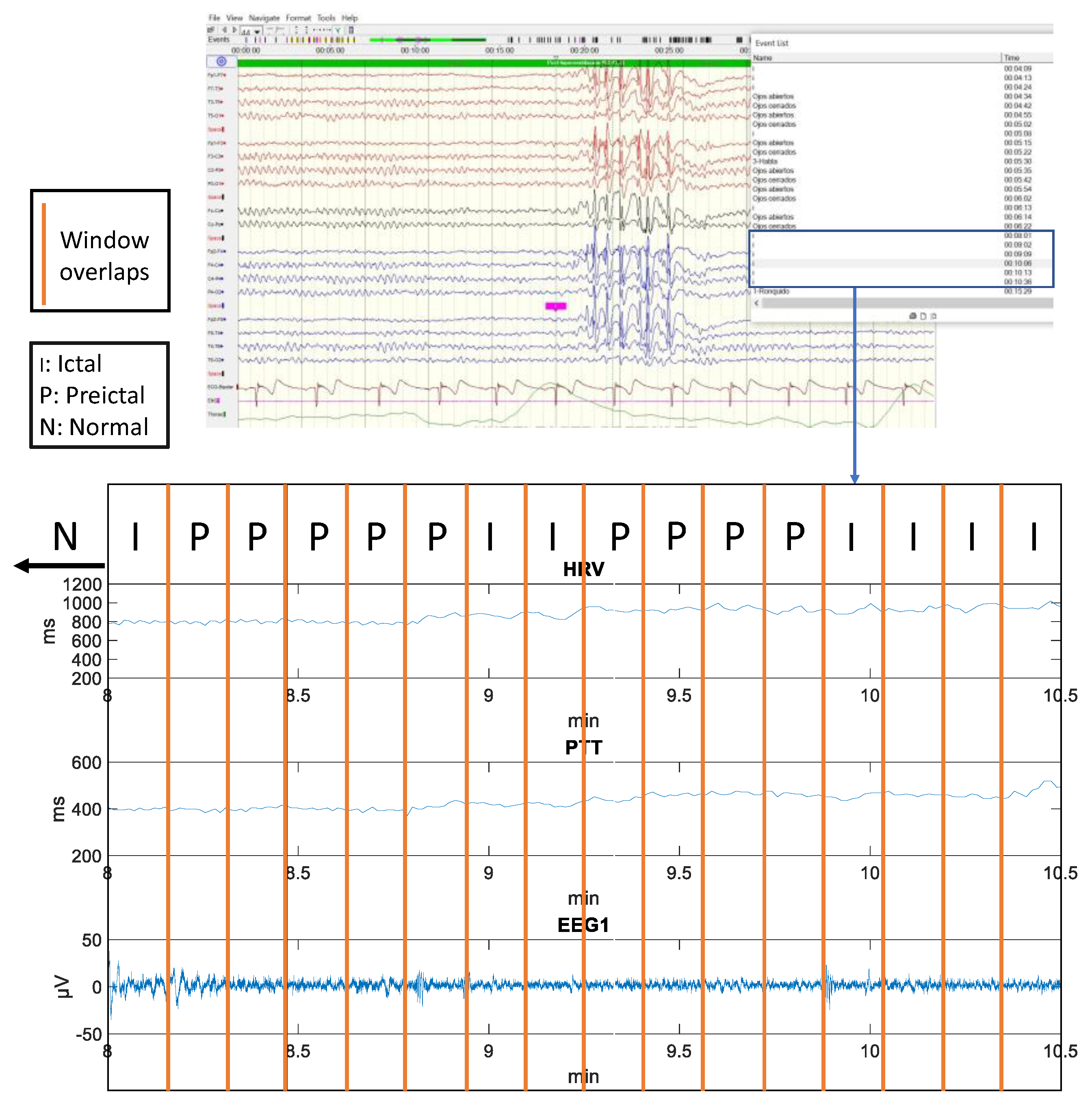
2.3. Data Processing
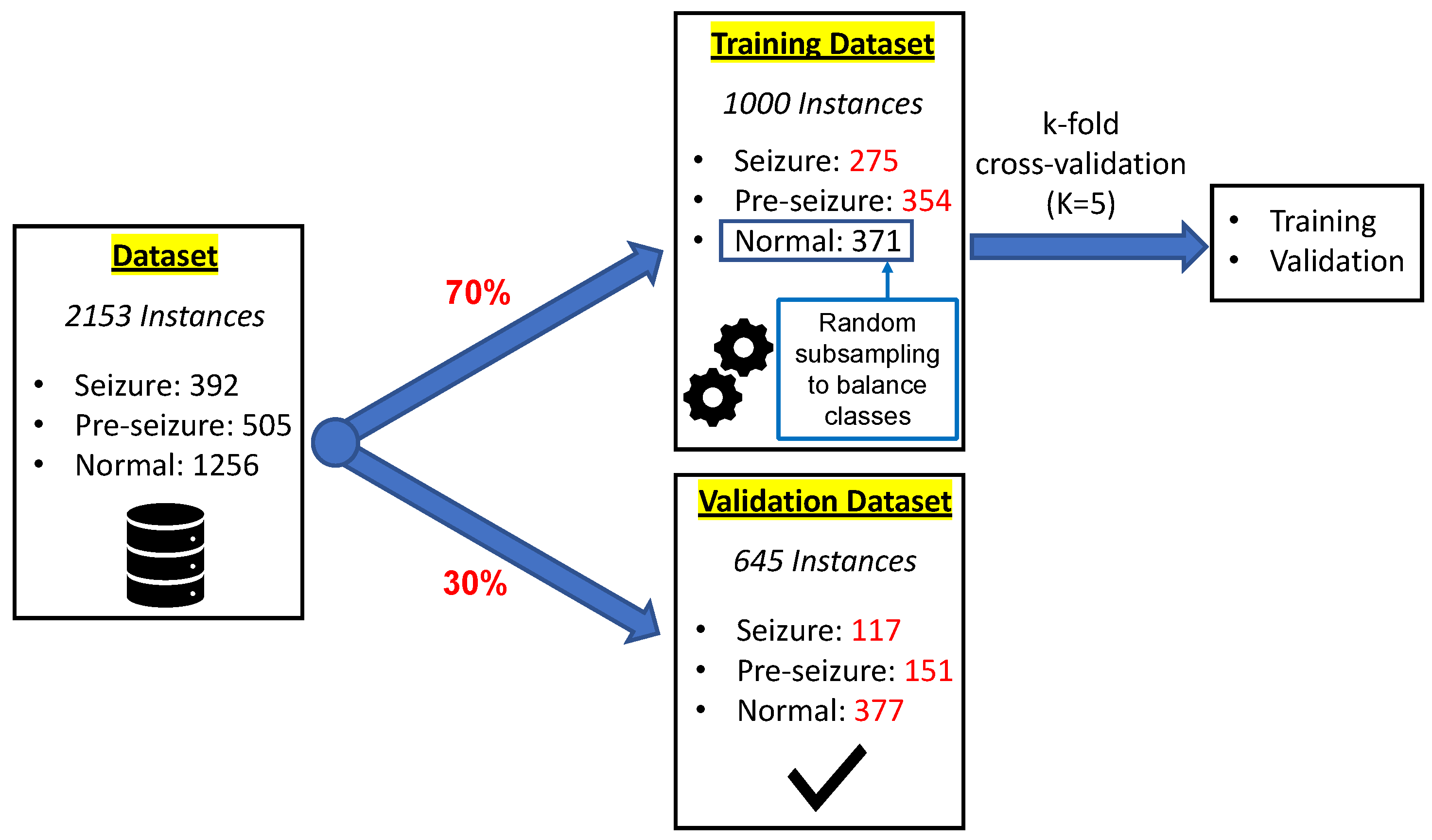
2.4. Predictive Model Generation
3. Results
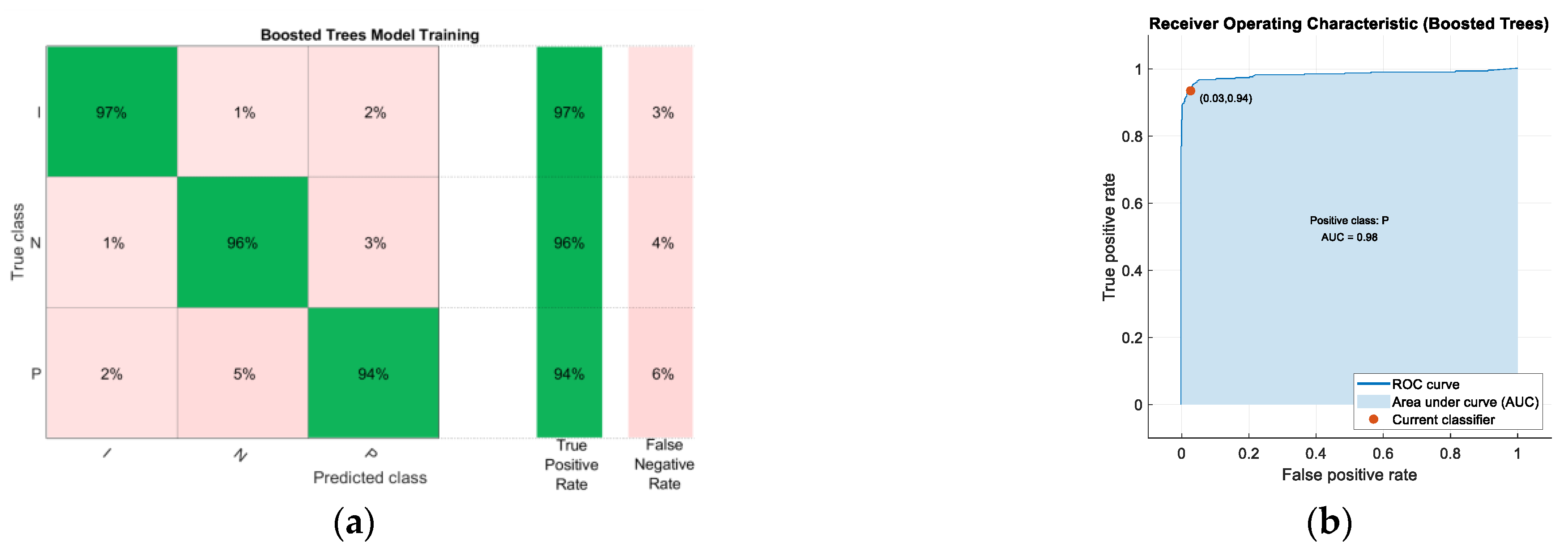
3.1. Predictive Model Training
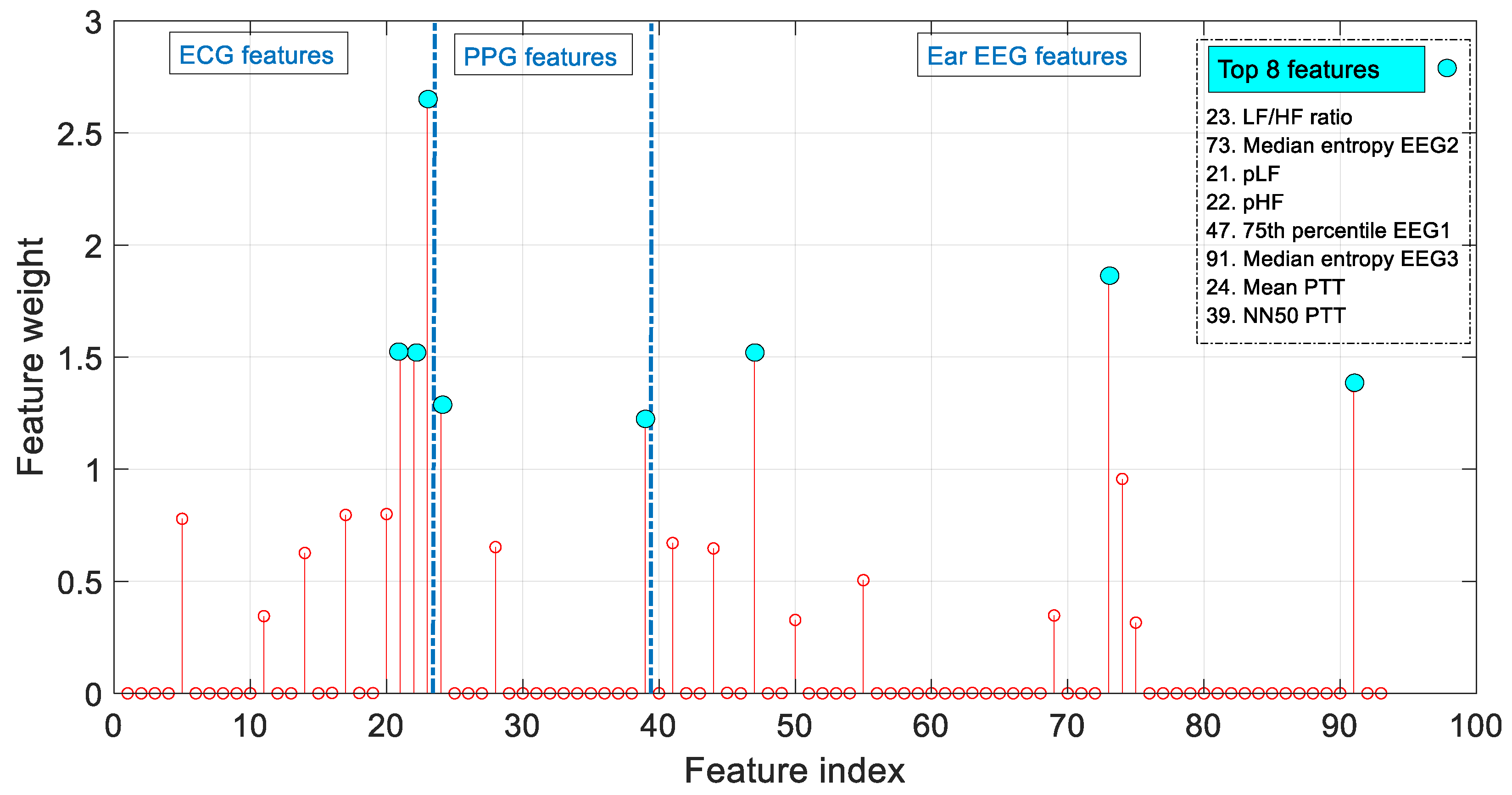
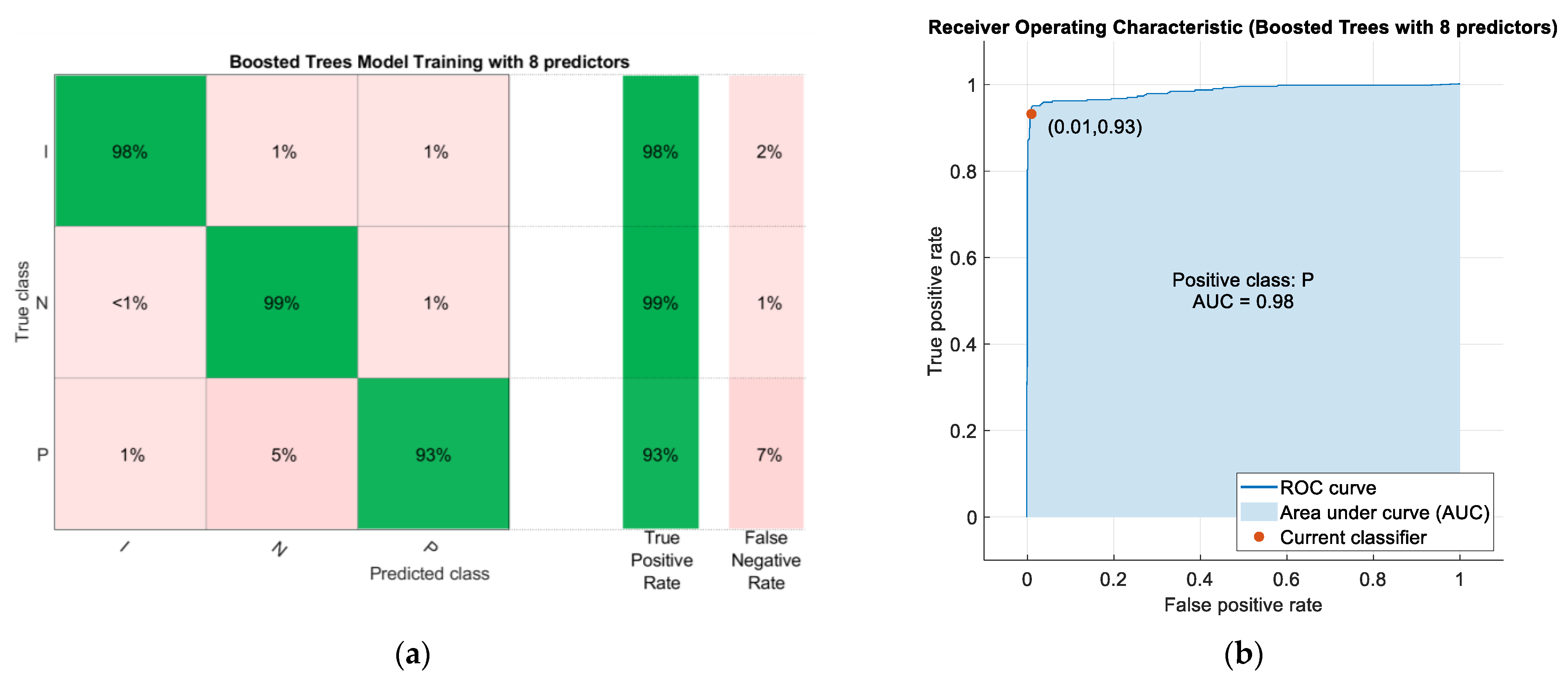
3.2. Reduced and Optimized Models
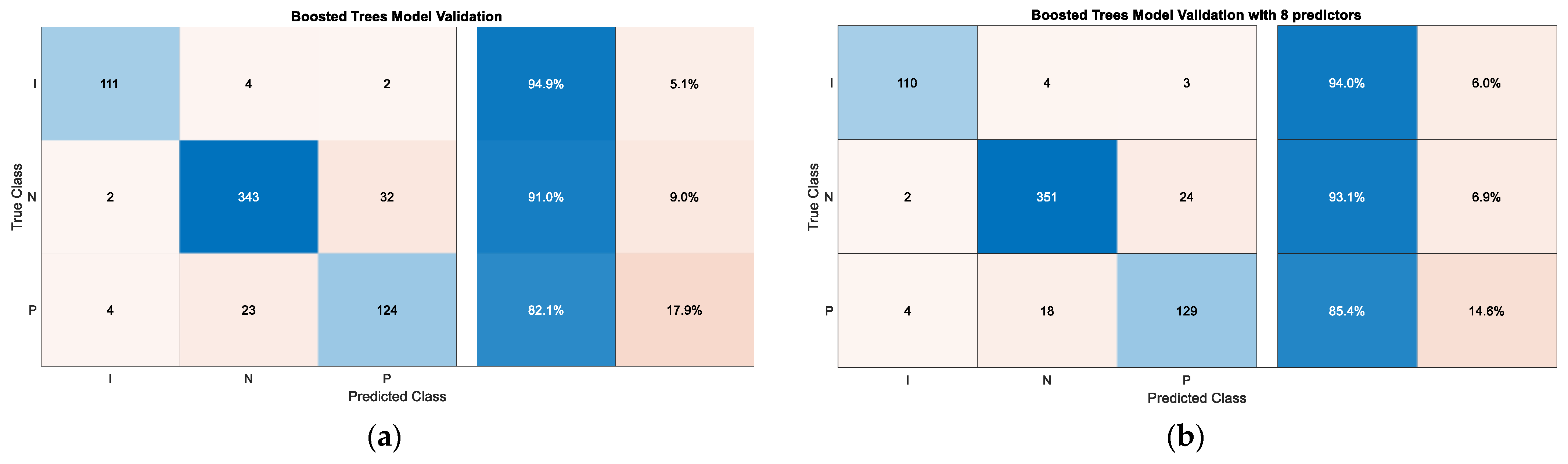
3.3. Predictive Model Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Epilepsy. Available online: https://www.who.int/news-room/fact-sheets/detail/epilepsy (accessed on 30 June 2022).
- Fisher, R.S.; Scharfman, H.E.; deCurtis, M. How can we identify ictal and interictal abnormal activity? Adv. Exp. Med. Biol. 2014, 813, 3–23. [Google Scholar]
- Nijsen, T.M.E.; Arends, J.B.A.M.; Griep, P.A.M.; Cluitmans, P.J.M. The potential value of three-dimensional accelerometry for detection of motor seizures in severe epilepsy. Epilepsy Behav. 2005, 7, 74–84. [Google Scholar] [CrossRef]
- Heldberg, B.E.; Kautz, T. Wearable sensors for semiology-independent seizure detection—Towards ambulatory monitoring of epilepsy. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015. [Google Scholar]
- Tzallas, A.T.; Tsipouras, M.G.; Fotiadis, D.I. Epileptic Seizure Detection in EEGs Using Time–Frequency Analysis. IEEE Trans. Inf. Technol. Biomed. 2009, 13, 703–710. [Google Scholar] [CrossRef]
- Acharya, U.R.; Vinitha Sree, S.; Swapna, G.; Martis, R.J.; Suri, J.S. Automated EEG analysis of epilepsy: A review. Knowl.-Based Syst. 2013, 45, 147–165. [Google Scholar] [CrossRef]
- You, S.; Cho, B.H.; Yook, S.; Kim, J.Y.; Shon, Y.M.; Seo, D.W.; Kim, I.Y. Unsupervised automatic seizure detection for focal-onset seizures recorded with behind-the-ear EEG using an anomaly-detecting generative adversarial network. Comput. Methods Programs Biomed. 2020, 193, 105472. [Google Scholar] [CrossRef]
- Gu, Y.; Cleeren, E.; Dan, J.; Claes, K.; Van Paesschen, W.; Van Huffel, S.; Hunyadi, B. Comparison between scalp EEG and behind-the-ear EEG for development of a wearable seizure detection system for patients with focal epilepsy. Sensors 2018, 18, 29. [Google Scholar] [CrossRef] [Green Version]
- Bleichner, M.G.; Debener, S. Concealed, Unobtrusive Ear-Centered EEG Acquisition: cEEGrids for Transparent EEG. Front. Hum. Neurosci. 2017, 11, 163. [Google Scholar] [CrossRef] [Green Version]
- Rafie, N.; Kashou, A.H.; Noseworthy, P.A. ECG Interpretation: Clinical Relevance, Challenges, and Advances. Hearts 2021, 2, 505–513. [Google Scholar] [CrossRef]
- Uijtdehaage, S.H.J.; Thayer, J.F. Accentuated antagonism in the control of human heart rate. Clin. Auton. Res. 2000, 10, 107–110. [Google Scholar] [CrossRef]
- Massin, M.M.; Maeyns, K.; Withofs, N.; Ravet, F.; Gérard, P. Circadian rhythm of heart rate and heart rate variability. Arch. Dis. Child 2000, 83, 179–182. [Google Scholar] [CrossRef] [Green Version]
- Myers, K.A.; Bello-Espinosa, L.E.; Symonds, J.D.; Zuberi, S.M.; Clegg, R.; Sadleir, L.G.; Buchhalter, J.; Scheffer, I.E. Heart rate variability in epilepsy: A potential biomarker of sudden unexpected death in epilepsy risk. Epilepsia 2018, 59, 1372–1380. [Google Scholar] [CrossRef]
- Block, R.C.; Yavarimanesh, M.; Natarajan, K.; Carek, A.; Mousavi, A.; Chandrasekhar, A.; Kim, C.-S.; Zhu, J.; Schifitto, G.; Mestha, L.K.; et al. Conventional pulse transit times as markers of blood pressure changes in humans. Sci. Rep. 2020, 10, 16373. [Google Scholar] [CrossRef]
- Nass, R.D.; Hampel, K.; Elger, C.E.; Surges, R. Blood Pressure in Seizures and Epilepsy. Front. Neurol. 2019, 10, 501. [Google Scholar] [CrossRef] [Green Version]
- Post-ictal Physiology: Adding Blood Pressure to the Equation. Available online: https://www.epilepsy.com/article/2016/12/post-ictal-physiology-adding-blood-pressure-equation (accessed on 30 June 2022).
- Embrace2®. Available online: https://www.empatica.com/en-eu/embrace2/ (accessed on 30 June 2022).
- MJN. Seras®. Available online: https://mjn.cat/ (accessed on 30 June 2022).
- EpiWatch®. Available online: https://www.apple.com/es/researchkit/ (accessed on 30 June 2022).
- SmartWatch by Smart Monitor®. Available online: https://www.epilepsy.com/deviceapedia/smartwatch-smart-monitor-0 (accessed on 30 June 2022).
- Patterson, A.L.; Mudigoudar, B.; Fulton, S. SmartWatch by SmartMonitor: Assessment of seizure detection efficacy for various seizure types in children: A large prospective single-center study. Pediatr. Neurol. 2015, 53, 309–311. [Google Scholar] [CrossRef]
- EpiCare@Home. Available online: https://www.epicareathome.com/ (accessed on 30 June 2022).
- Yamakawa, T.; Miyajima, M.; Fujiwara, K.; Kano, M.; Suzuki, Y.; Watanabe, Y.; Watanabe, S.; Hoshida, T.; Inaji, M.; Maehara, T. Wearable Epileptic Seizure Prediction System with Machine-Learning-Based Anomaly Detection of Heart Rate Variability. Sensors 2020, 20, 3987. [Google Scholar] [CrossRef]
- Billeci, L.; Tonacci, A.; Varanini, M.; Detti, P.; de Lara, G.Z.M.; Vatti, G. Epileptic seizures prediction based on the combination of EEG and ECG for the application in a wearable device. In Proceedings of the 2019 IEEE 23rd International Symposium on Consumer Technologies (ISCT), Ancona, Italy, 19–21 June 2019; pp. 28–33. [Google Scholar] [CrossRef]
- Nasseri, M.; Pal Attia, T.; Joseph, B.; Gregg, N.M.; Nurse, E.S. Non-invasive wearable seizure detection using long-short-term memory networks with transfer learning. J. Neural Eng. 2021, 18, 056017. [Google Scholar] [CrossRef]
- Pavei, J.; Heinzen, R.G.; Novakova, B.; Walz, R.; Serra, A.J.; Reuber, M.; Ponnusamy, A.; Marques, J.L.B. Early seizure detection based on cardiac autonomic regulation dynamics. Front. Physiol. 2017, 8, 765. [Google Scholar] [CrossRef] [Green Version]
- Zhou, M.; Tian, C.; Cao, R.; Wang, B.; Niu, Y.; Hu, T.; Guo, H.; Xiang, J. Epileptic Seizure Detection Based on EEG Signals and CNN. Front Neuroinform. 2018, 10, 12–95. [Google Scholar] [CrossRef] [Green Version]
- Kusmakar, S.; Karmakar, C.; Yan, B.; Obrien, T.; Muthuganapathy, R.; Palaniswami, M. Automated Detection of Convulsive Seizures Using a Wearable Accelerometer Device. IEEE Trans. Biomed. Eng. 2019, 66, 421–432. [Google Scholar] [CrossRef]
- Zambrana-Vinaroz, D.; Vicente-Samper, J.M.; Sabater-Navarro, J.M. Validation of Continuous Monitoring System for Epileptic Users in Outpatient Settings. Sensors 2022, 22, 2900. [Google Scholar] [CrossRef]
- EEG Nicolet V32®. Available online: https://neuro.natus.com/es-es/productos-y-servicios/sistema-de-eeg-nicoletone (accessed on 30 June 2022).
- Zambrana-Vinaroz, D.; Vicente-Samper, J.M.; Juan, C.G.; Esteve-Sala, V.; Sabater-Navarro, J.M. Non-Invasive Device for Blood Pressure Wave Acquisition by Means of Mechanical Transducer. Sensors 2022, 19, 4311. [Google Scholar] [CrossRef] [Green Version]
- Wood, C.; Cano, V.A. La Hiperventilación y el Trastorno de Angustia a la Luz de un Marco Cognitivo. Clín. Salud. 2021, 20, 57–66. [Google Scholar]
- Liu, T.; Truong, N.D.; Nikpour, A.; Zhou, L.; Kavehei, O. Epileptic Seizure Classification with Symmetric and Hybrid Bilinear Models. IEEE J. Biomed. Health Inform. 2020, 24, 2844–2851. [Google Scholar] [CrossRef] [Green Version]
- Albaqami, H.; Hassan, G.M.; Datta, A. Wavelet-Based Multi-Class Seizure Type Classification System. Appl. Sci. 2022, 12, 5702. [Google Scholar] [CrossRef]
- Esco, M.R.; Flatt, A.A. Ultra-short-term heart rate variability indexes at rest and post-exercise in athletes: Evaluating the agreement with accepted recommendations. J. Sport. Sci. Med. 2014, 13, 535–541. [Google Scholar]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- DeGiorgio, C.M.; Miller, P.; Meymandi, S. RMSSD, a measure of vagus-mediated heart rate variability, is associated with risk factors for SUDEP: The SUDEP-7 Inventory. Epilepsy Behav. 2010, 19, 78–81. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.; Koo, H.; Lee, W.; Kim, M. Application and Limitation of Frequency Domain, LF/HF Component in Heart Rate Variability as an Acute Stress Index. Age 2014, 30, 39. [Google Scholar]
- Heathers, J.A.J. Everything Hertz: Methodological issues in short-term frequency-domain HRV. Front. Physiol. 2014, 5, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Hernández, S.E.; Salido-Ruiz, R.A.; Torres-Ramos, S.; Román-Godínez, I. Evaluation of Feature Selection Methods for Classification of Epileptic Seizure EEG Signals. Sensors 2022, 22, 3066. [Google Scholar] [CrossRef]
- Boonyakitanont, P.; Lek-Uthai, A.; Chomtho, K.; Songsiri, J. A review of feature extraction and performance evaluation in epileptic seizure detection using EEG. Biomed. Signal Process. Control 2020, 57, 101702. [Google Scholar] [CrossRef] [Green Version]
- Snyder, D.E.; Echauz, J.; Grimes, D.B.; Litt, B. The statistics of a practical seizure warning system. J. Neural Eng. 2008, 5, 392–401. [Google Scholar] [CrossRef] [Green Version]
- Autoregressive Power Spectral Density Estimate—Burg’s Method. Available online: https://es.mathworks.com/help/signal/ref/pburg.html (accessed on 30 June 2022).
- Zijlmans, M.; Jacobs, J.; Kahn, Y.U.; Zelmann, R.; Dubeau, F.; Gotman, J. Ictal and interictal high frequency oscillations in patients with focal epilepsy. Clin. Neurophysiol. 2011, 122, 664–671. [Google Scholar] [CrossRef]
- Classification Learner App. Available online: https://www.mathworks.com/help/stats/classificationlearner-app.html (accessed on 30 June 2022).
- Principal Component Analysis (PCA). Available online: https://www.mathworks.com/help/stats/principal-component-analysis-pca.html (accessed on 30 June 2022).
- González-Barcenas, V.M.; Rendón, E.; Alejo, R.; Granda-Gutiérrez, E.E.; Valdovinos, R.M. Addressing the Big Data Multi-class Imbalance Problem with Oversampling and Deep Learning Neural Networks. In Pattern Recognition and Image Analysis; Morales, A., Fierrez, J., Sánchez, J.S., Ribeiro, B., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 216–224. [Google Scholar]
- Browne, M.W. Cross-Validation Methods. J. Math. Psychol. 2000, 44, 108–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neighborhood Component Analysis (NCA) Feature Selection. Available online: https://www.mathworks.com/help/stats/neighborhood-component-analysis.html (accessed on 30 June 2022).
- Billeci, L.; Marino, D.; Insana, L.; Vatti, G.; Varanini, M. Patient-specific seizure prediction based on heart rate variability and recurrence quantification analysis. PLoS ONE 2018, 13, e0204339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirzaei, A.; Ayatollahi, A.; Gifani, P.; Salehi, L. Spectral Entropy for Epileptic Seizures Detection. In Proceedings of the 2010 2nd International Conference on Computational Intelligence, Communication Systems and Networks, Liverpool, UK, 28–30 July 2010; pp. 301–307. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Age (Years) |
|---|---|
| Female | 45 |
| Male | 18 |
| Female | 32 |
| Male | 45 |
| Male | 39 |
| Male | 42 |
| Female | 47 |
| Male | 26 |
| Female | 35 |
| Male | 39 |
| Machine Learning Algorithm | Accuracy (%) ECG, PPG, Ear EEG | Accuracy (%) Ear EEG |
|---|---|---|
| Fine Tree | 92.3 | 84.2% |
| Linear discriminant | 78.2 | 78.8% |
| Kernel Naive Bayes | 83.1 | 78.4% |
| Linear SVM | 75.1 | 78.3% |
| Quadratic SVM | 83.7 | 84.0% |
| Cubic SVM | 86.4 | 84.3% |
| Cosine KNN | 78.2 | 83.9% |
| Weighted KNN | 80.3 | 82.1% |
| Boosted Trees | 95.5 | 86.9% |
| Bagged Trees | 86.2 | 86.6% |
| Subspace KNN | 93.2 | 87.9% |
| RUSBoosted Trees | 93.8 | 87.0% |
| Number of Principal Components | Explained Variance |
|---|---|
| 10 | 75% |
| 23 | 90% |
| 31 | 95% |
| 72 | 99.99% |
| 89 | 100% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zambrana-Vinaroz, D.; Vicente-Samper, J.M.; Manrique-Cordoba, J.; Sabater-Navarro, J.M. Wearable Epileptic Seizure Prediction System Based on Machine Learning Techniques Using ECG, PPG and EEG Signals. Sensors 2022, 22, 9372. https://doi.org/10.3390/s22239372
Zambrana-Vinaroz D, Vicente-Samper JM, Manrique-Cordoba J, Sabater-Navarro JM. Wearable Epileptic Seizure Prediction System Based on Machine Learning Techniques Using ECG, PPG and EEG Signals. Sensors. 2022; 22(23):9372. https://doi.org/10.3390/s22239372
Chicago/Turabian StyleZambrana-Vinaroz, David, Jose Maria Vicente-Samper, Juliana Manrique-Cordoba, and Jose Maria Sabater-Navarro. 2022. "Wearable Epileptic Seizure Prediction System Based on Machine Learning Techniques Using ECG, PPG and EEG Signals" Sensors 22, no. 23: 9372. https://doi.org/10.3390/s22239372