

Evaluation of Error-State Kalman Filter Method for Estimating Human Lower-Limb Kinematics during Various Walking Gaits
 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. ErKF Method for Seven-Body Lower-Limb Model
2.1.1. ErKF States
2.1.2. Process Model
2.1.3. Measurement Model
2.1.4. Details of ErKF Method Specific to Human Subjects
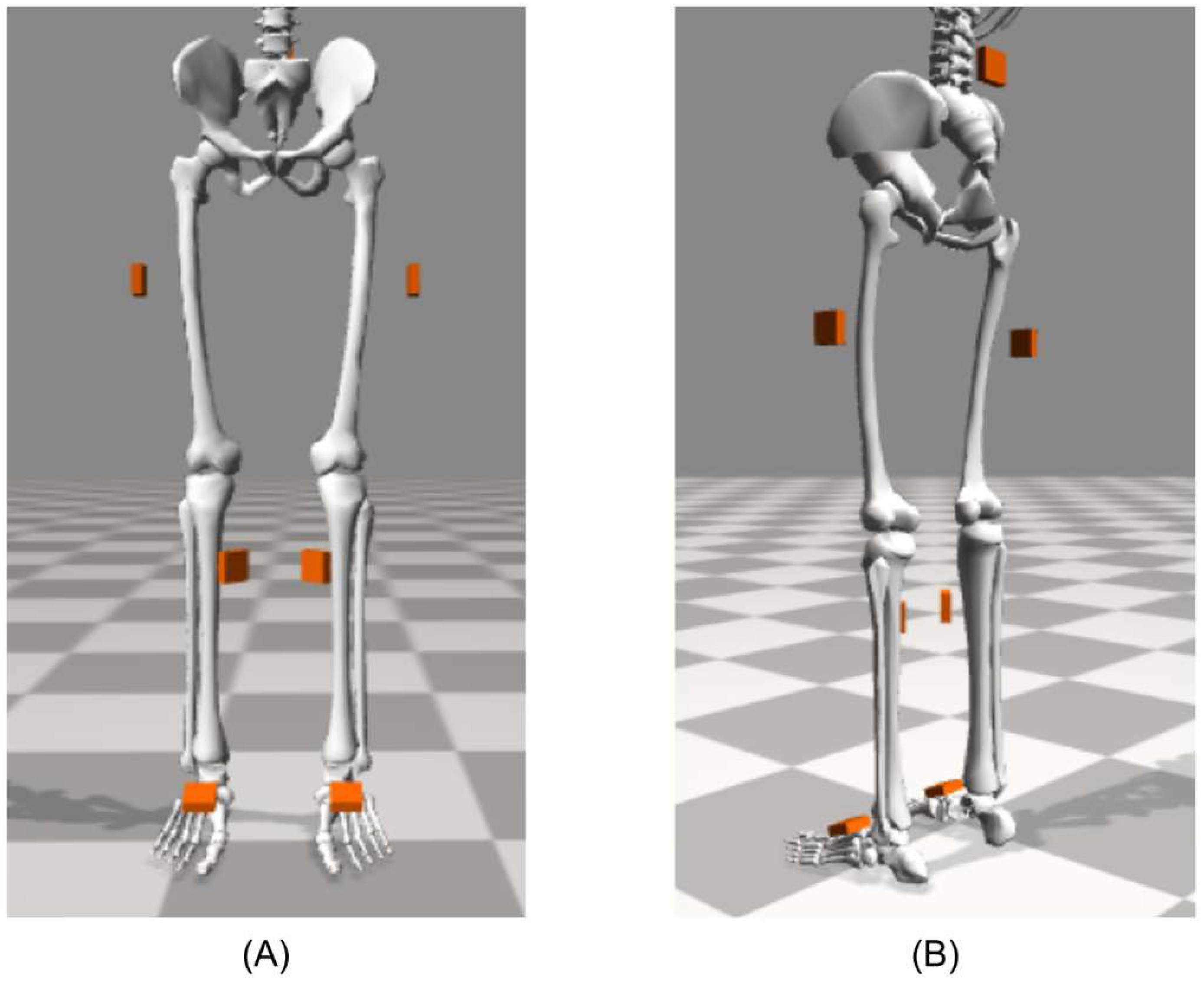
2.2. Human Subject Experiment
2.3. Kinematic Comparisons
2.4. Calibration of ErKF and MOCAP Models
2.5. Estimated Kinematics from the ErKF Method
2.6. Estimated Kinematics from Two MOCAP Methods
2.6.1. Cluster Method (Clust)
2.6.2. Inverse Kinematics Method (IK)
3. Results
3.1. Results across All Twenty Human Subjects
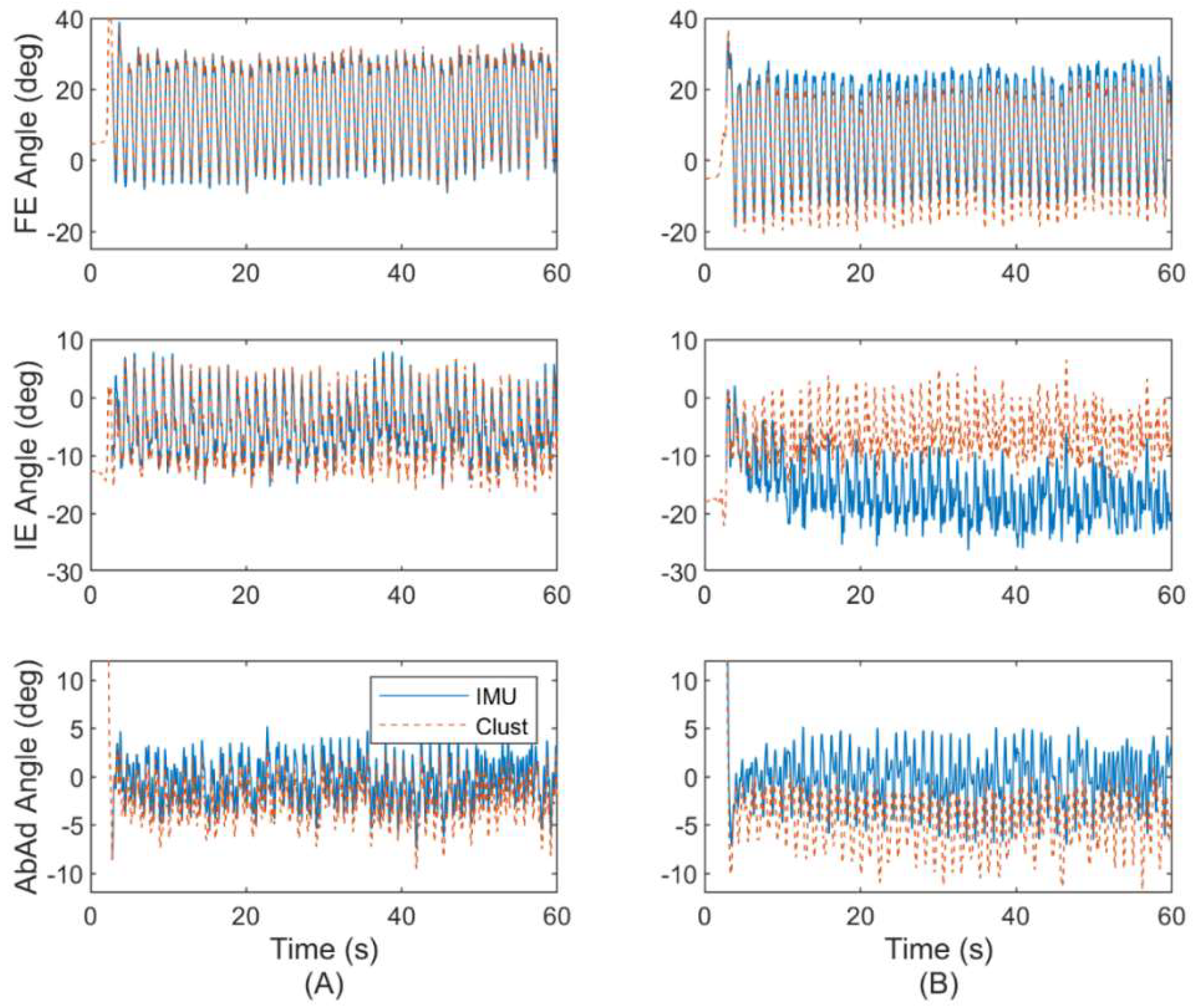
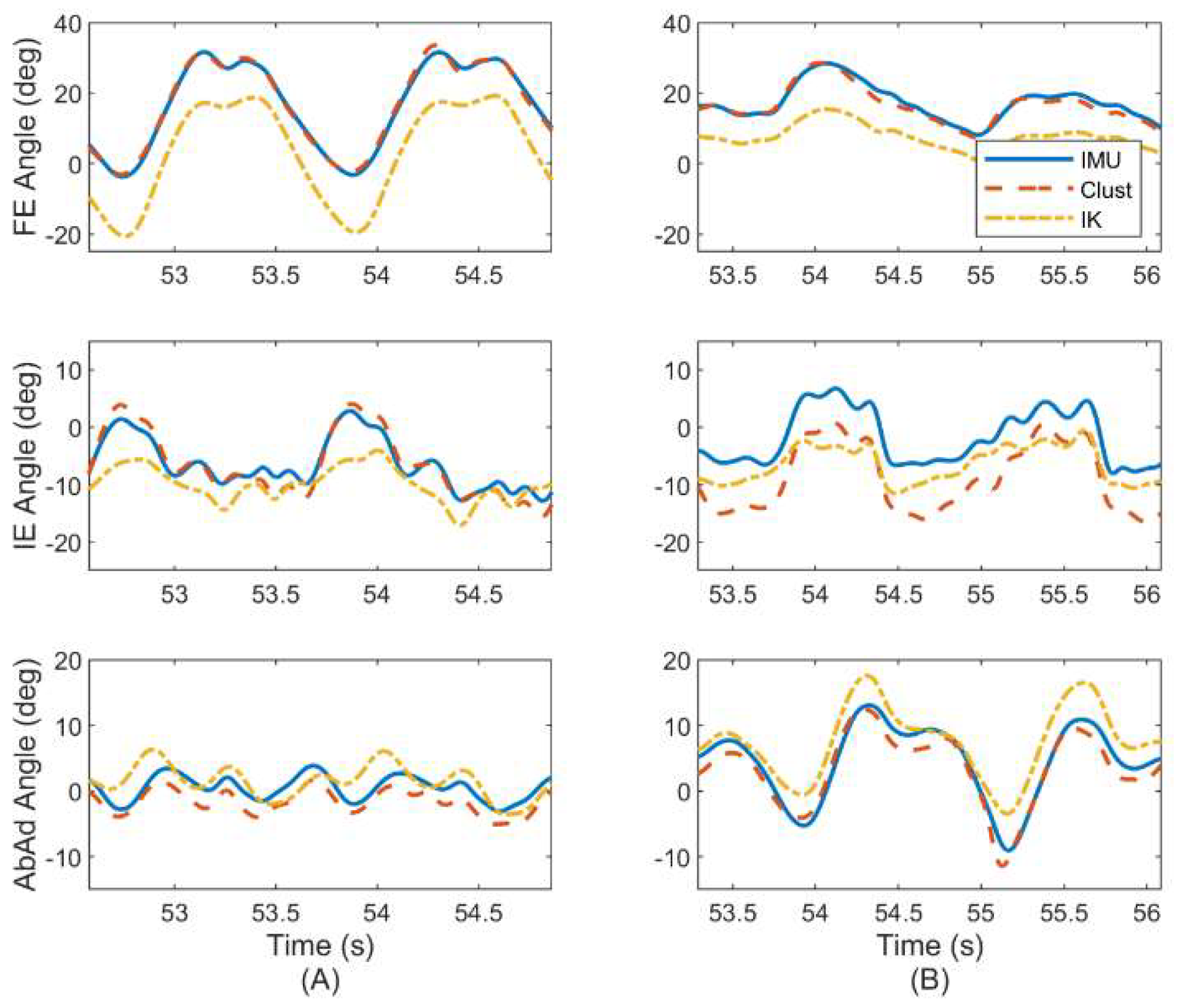
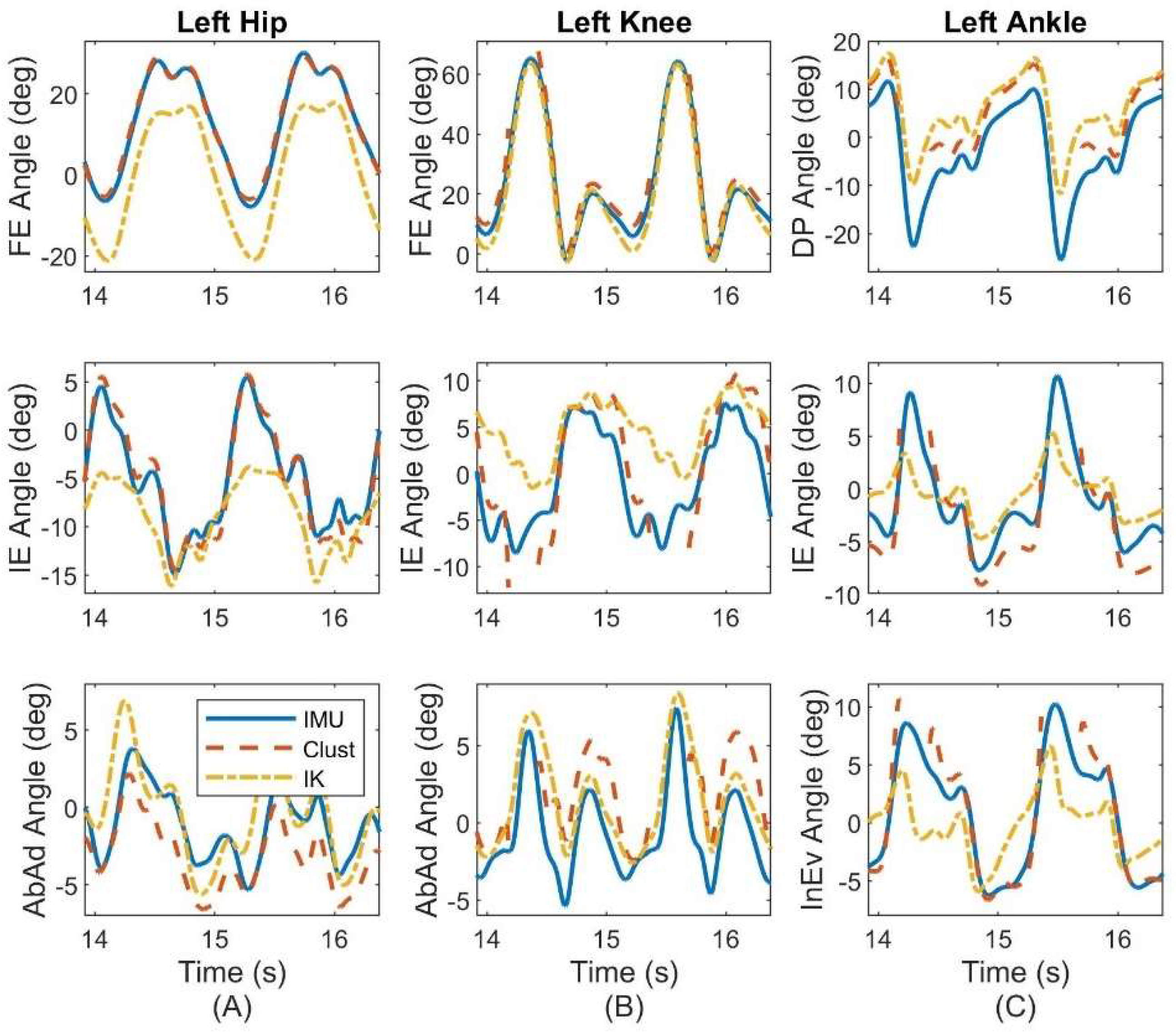
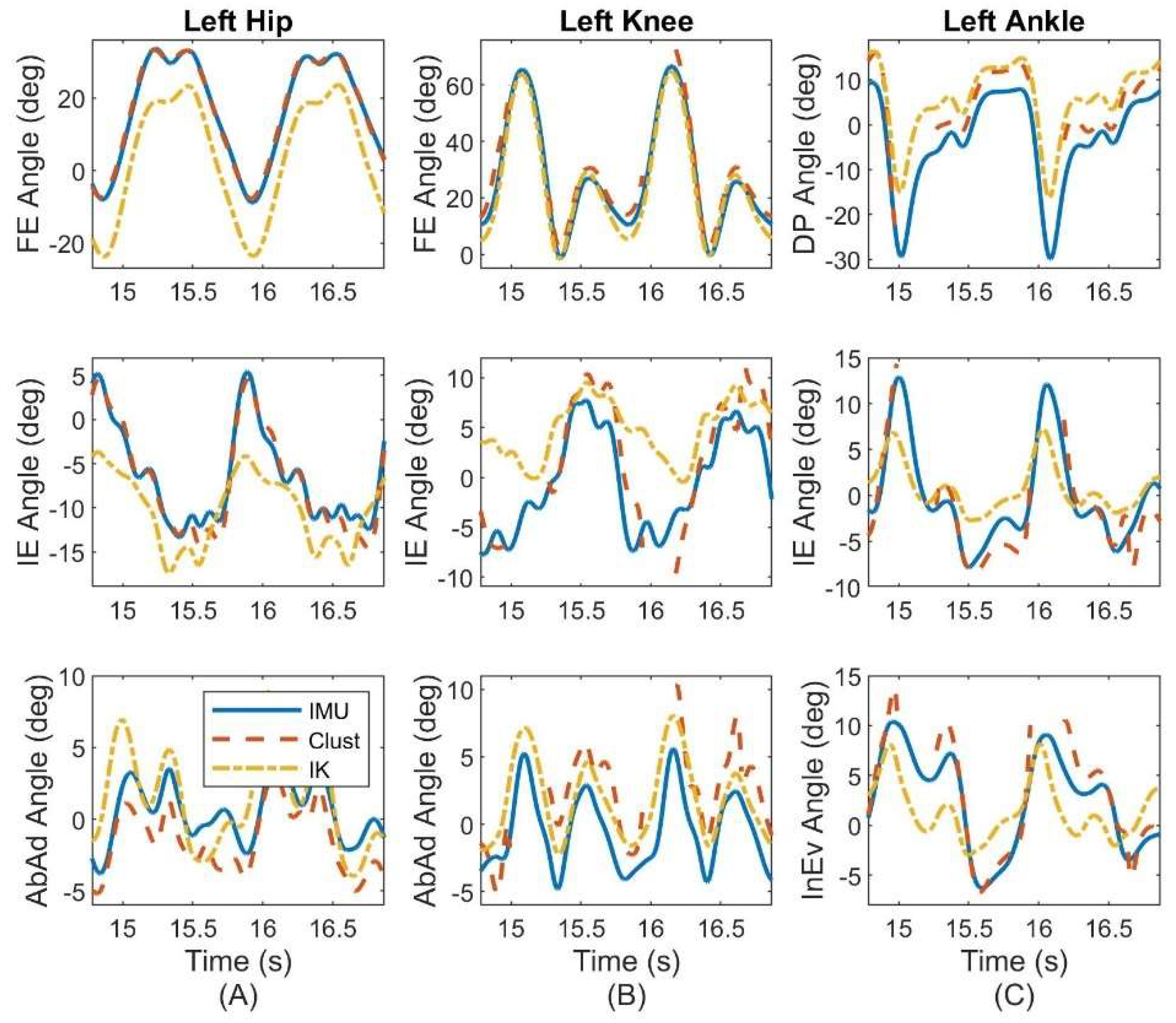
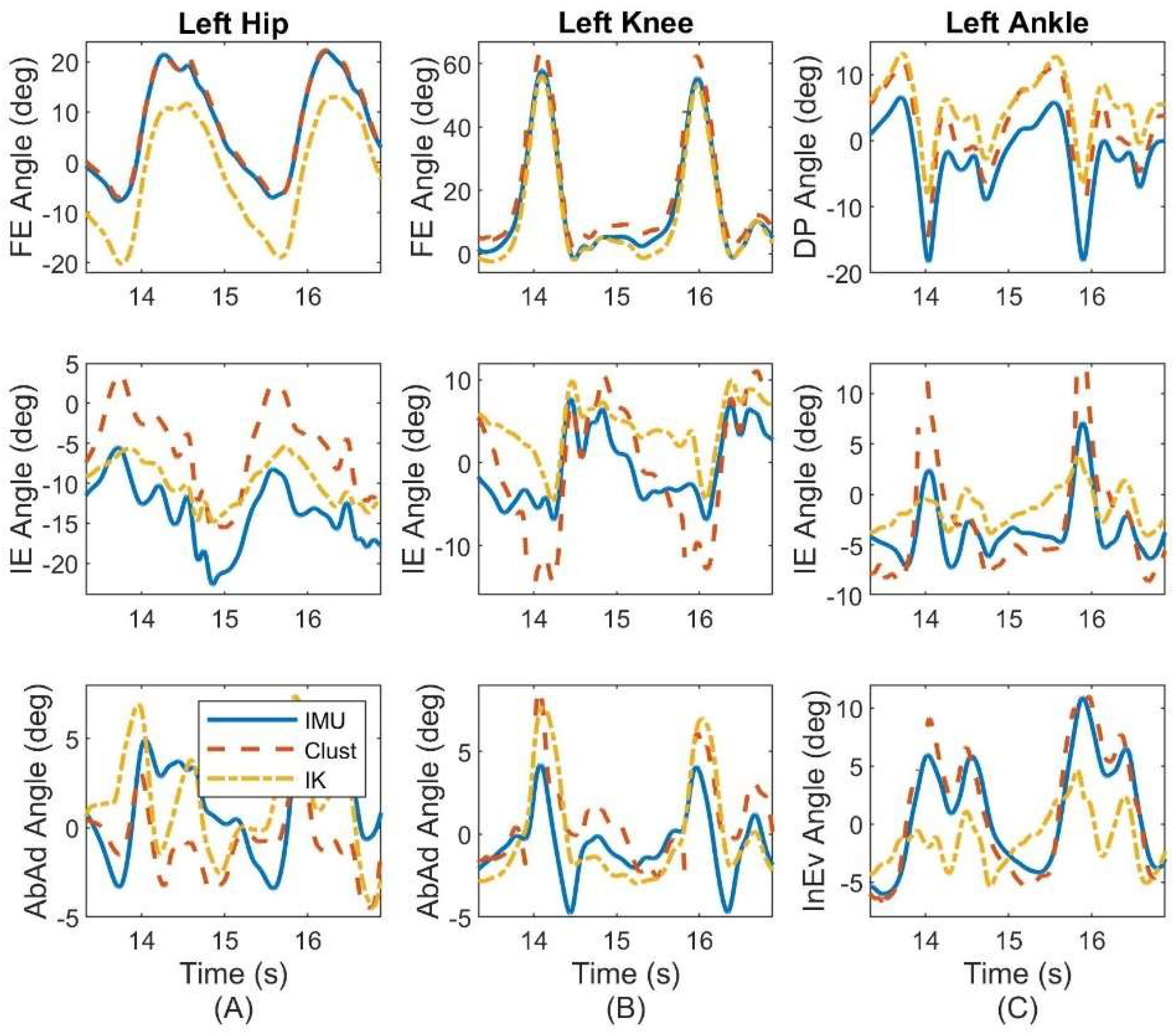
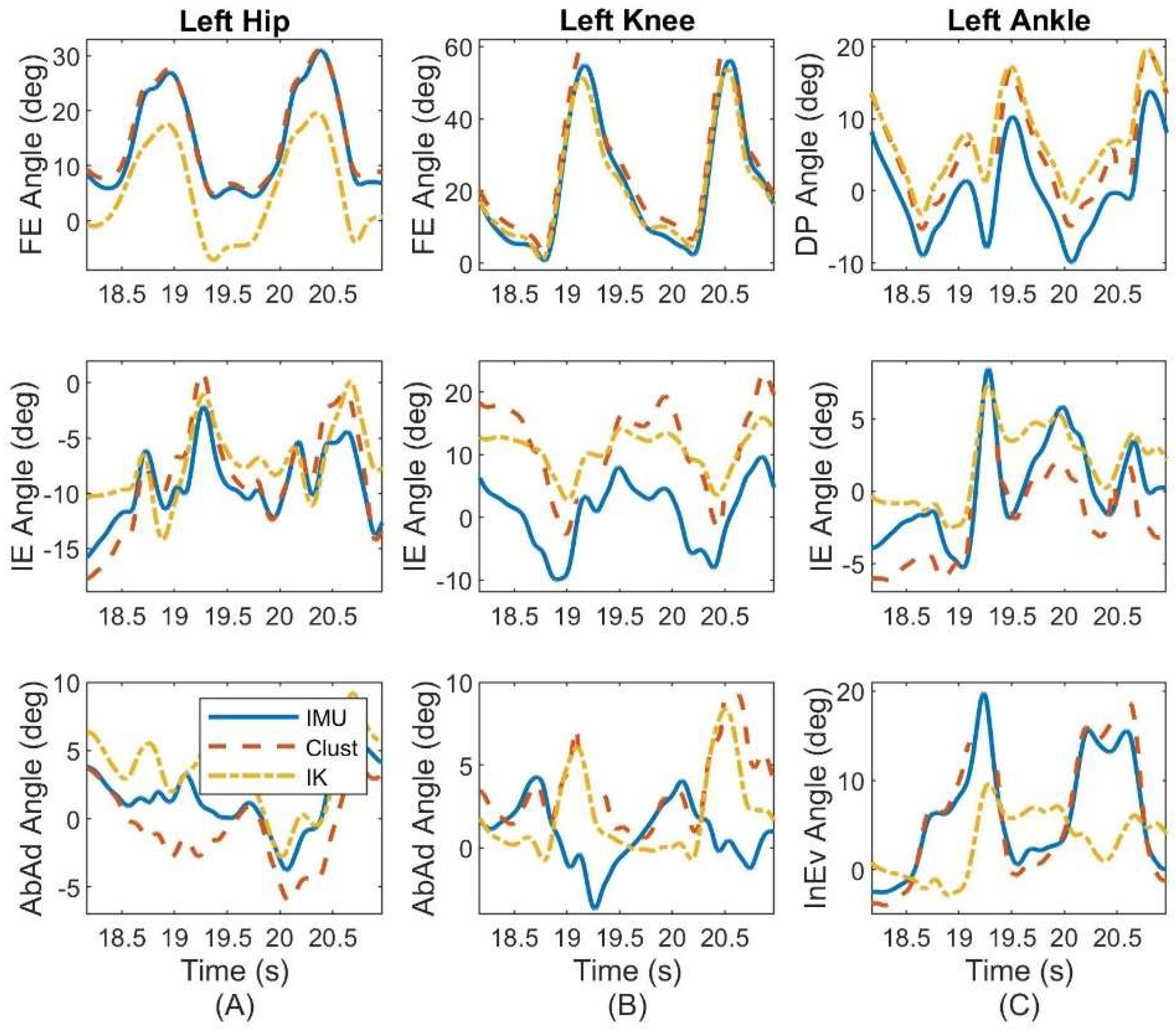
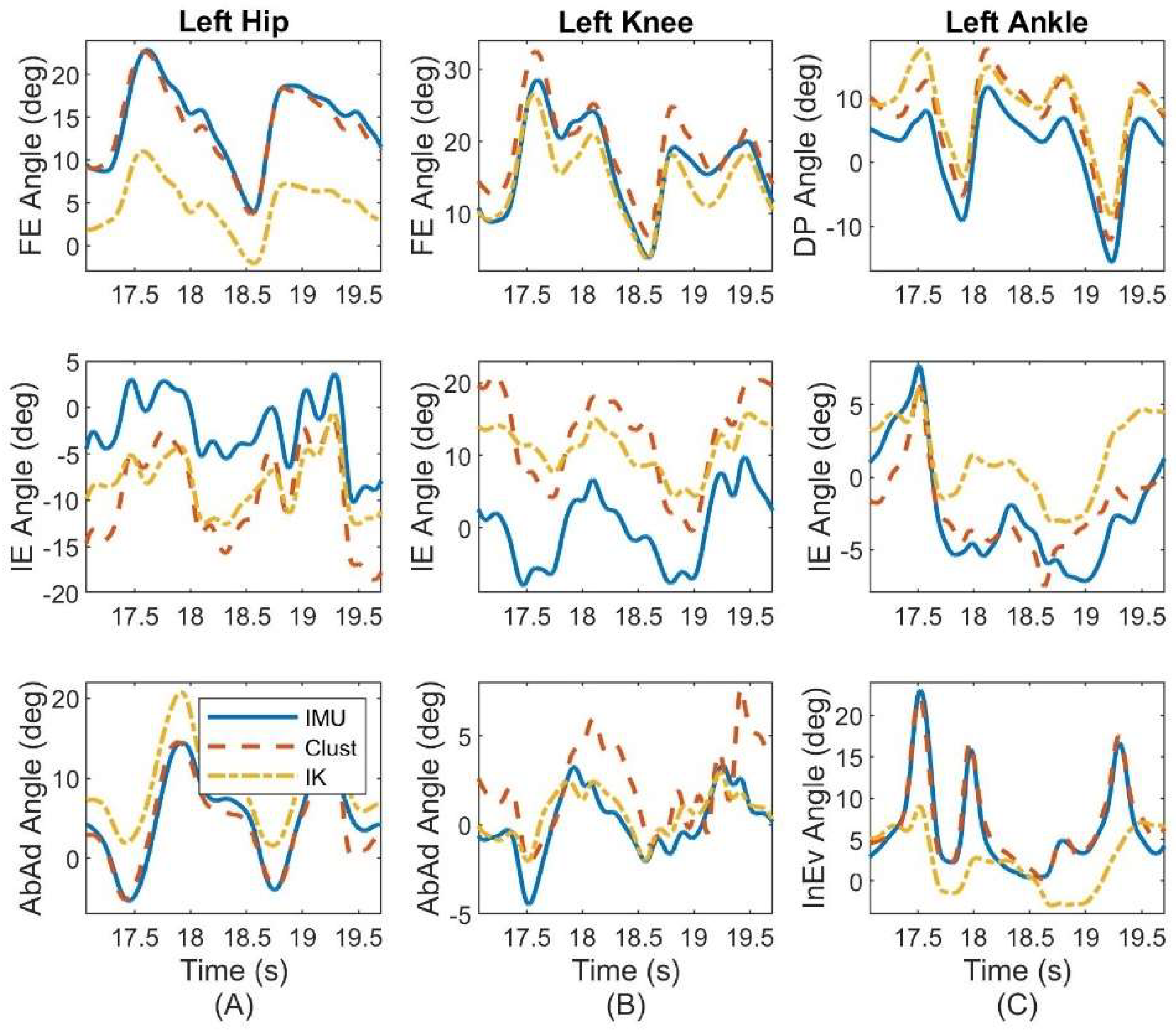
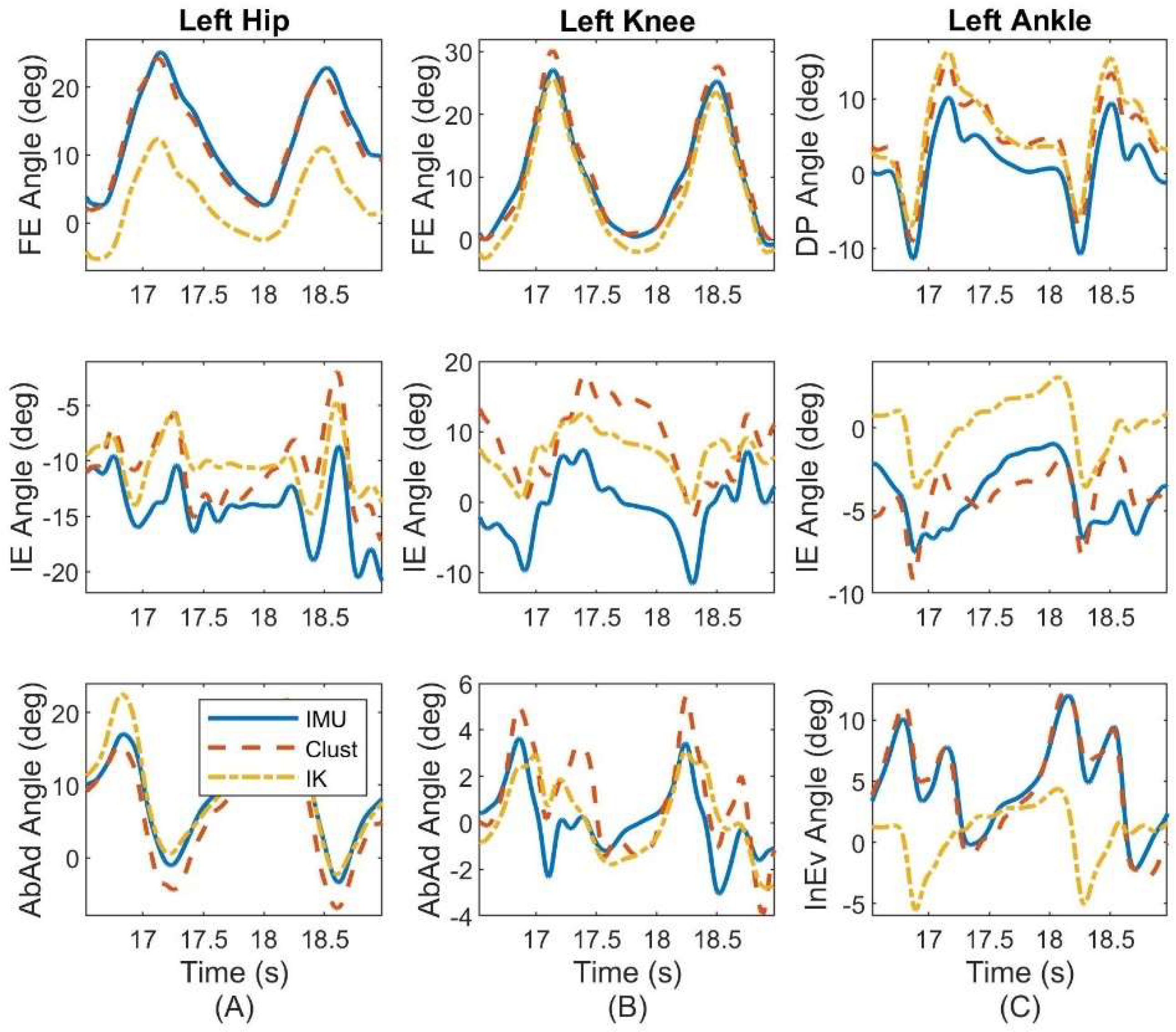
3.2. Representative Results on a Single Subject
4. Discussion
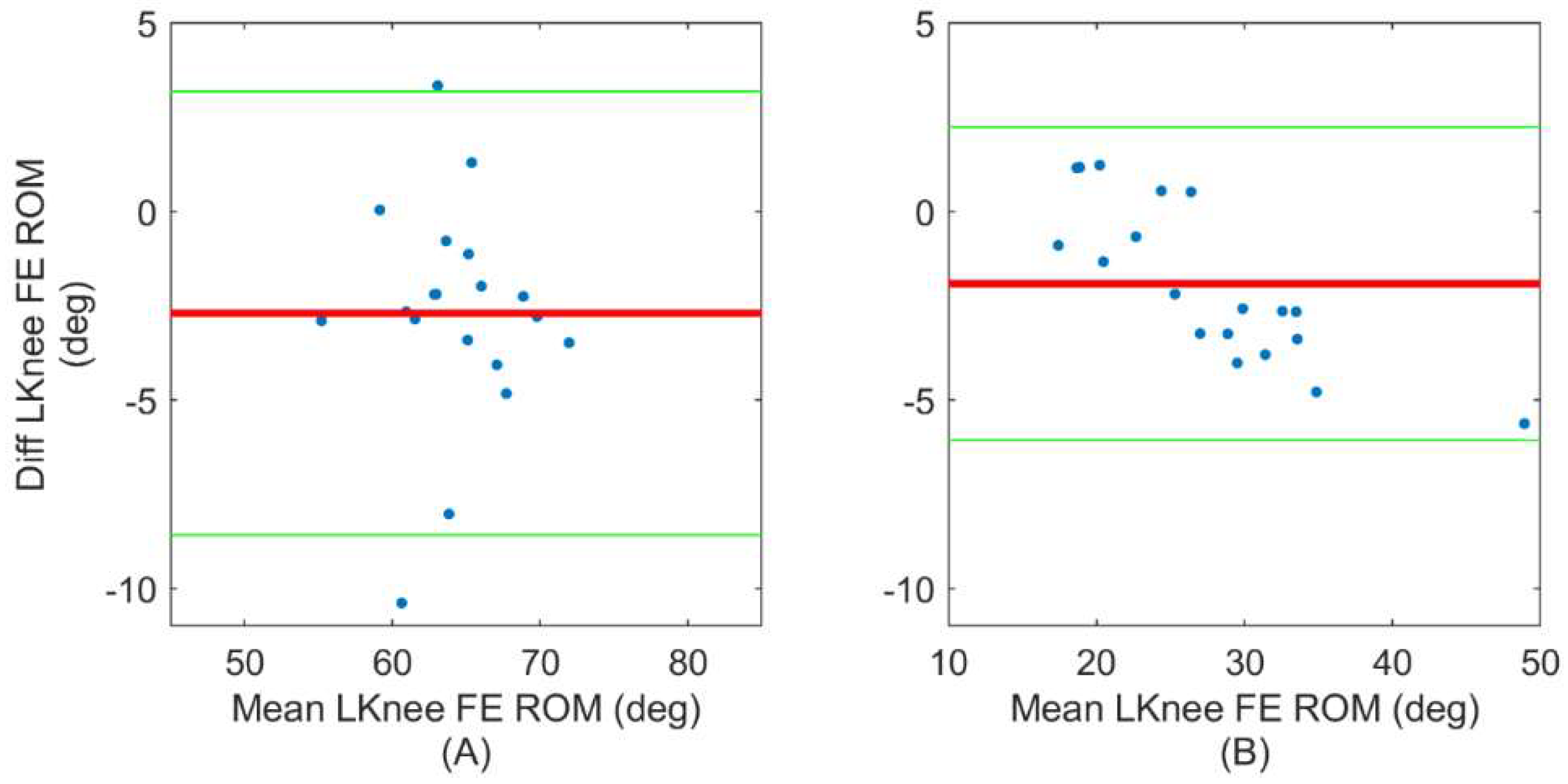
4.1. ErKF Estimates of Instantaneous Joint Angles
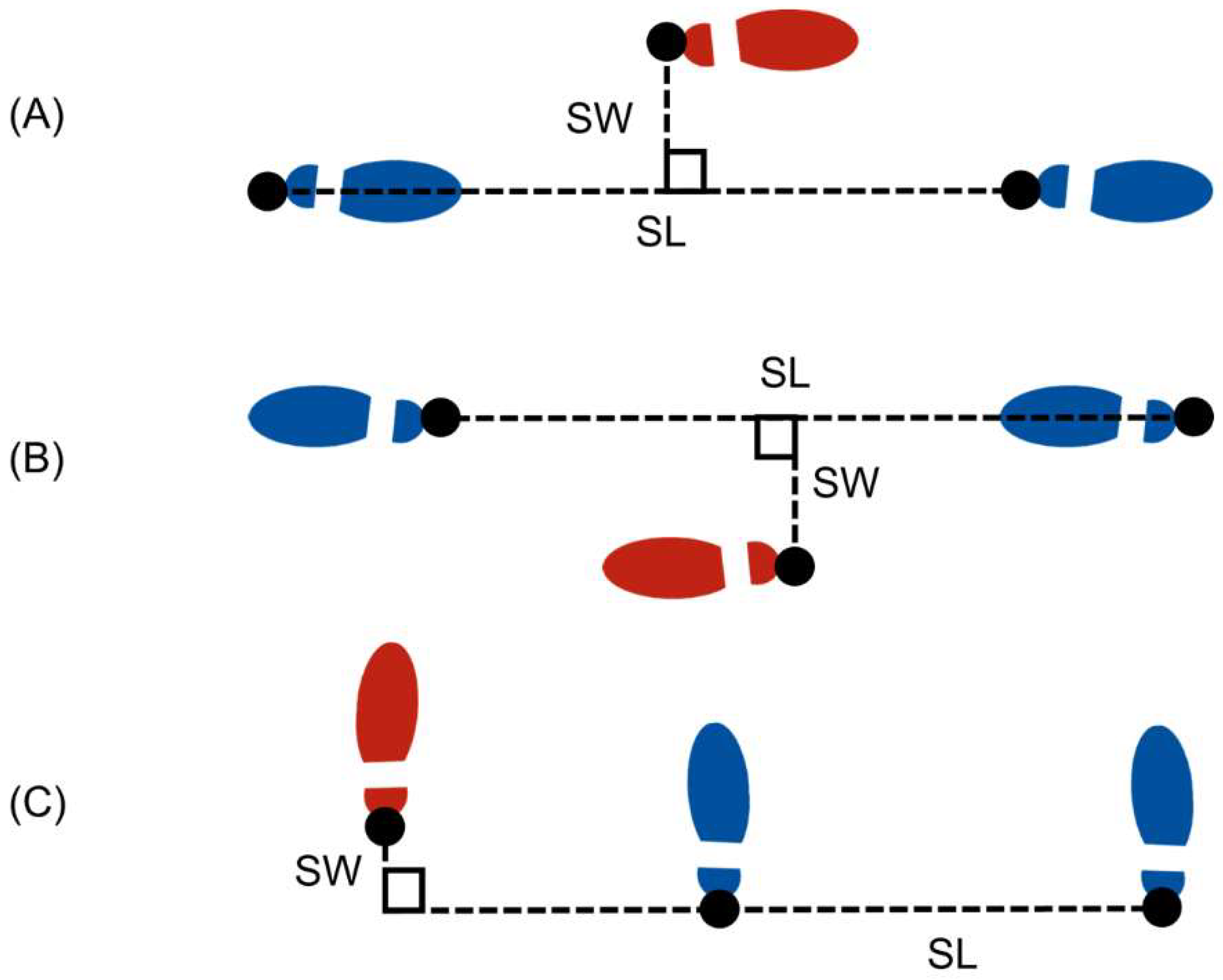
4.2. ErKF Estimates of Stride Parameters
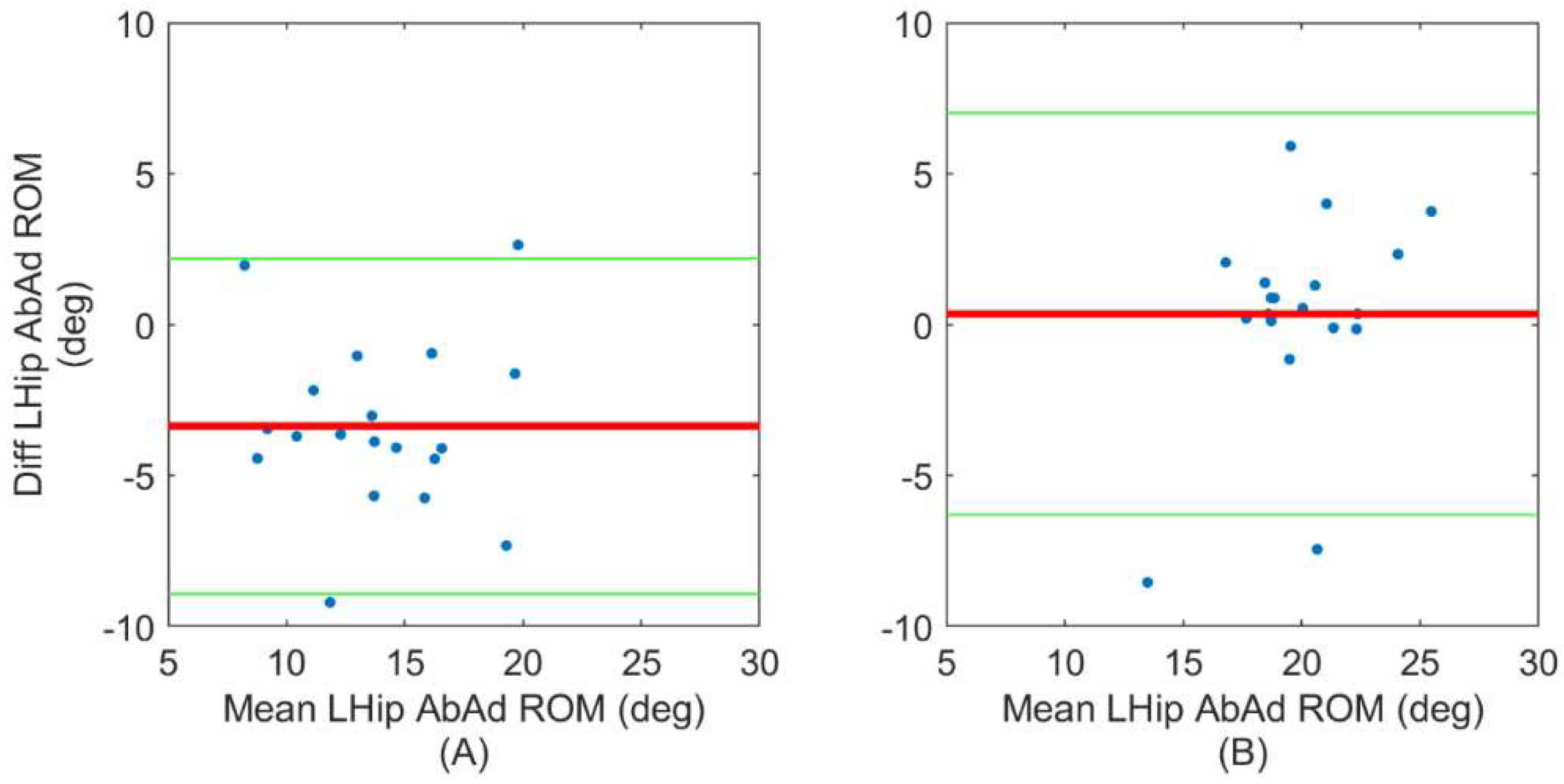
4.3. Utility of ErKF Joint Angle Range of Motion Estimates
4.4. Comparison of ErKF Method to other IMU-Based Methods
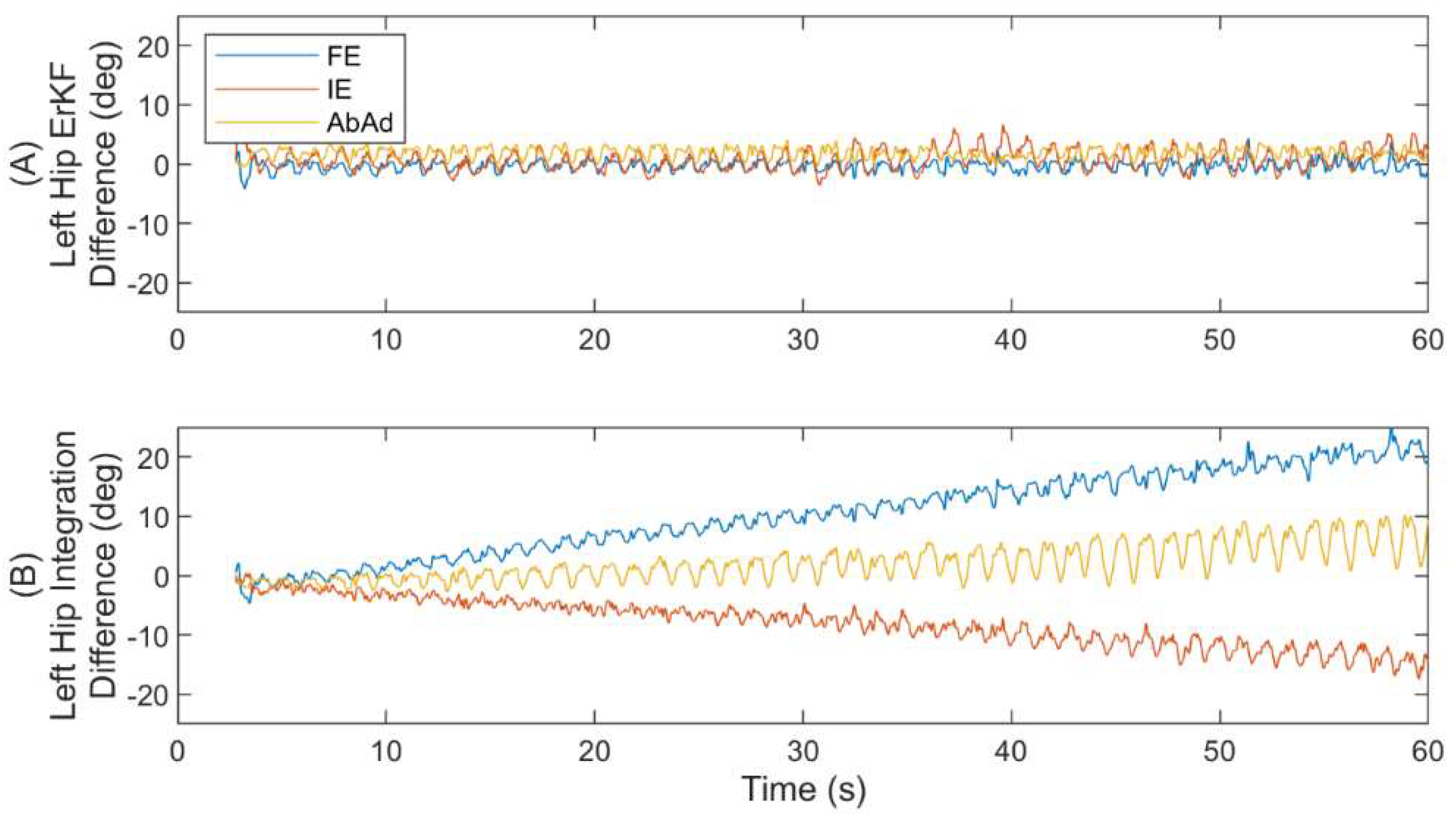
4.5. Performance of Novel Hip “Soft” Hinge Correction
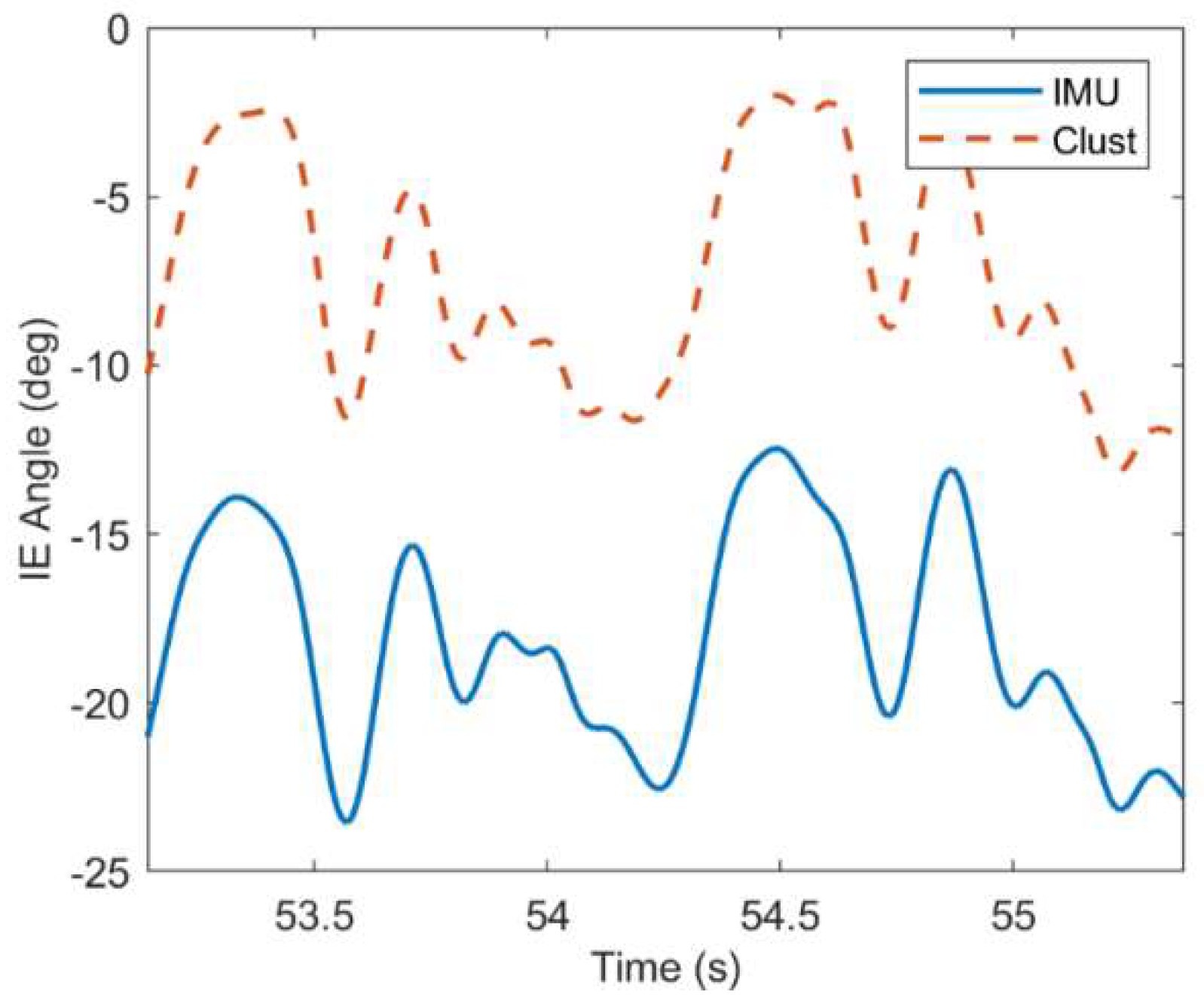
4.6. Factors Leading to Abnormally Poor Estimates
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A.—Example Trajectories for Six Walking Gaits






References
- Seth, A.; Hicks, J.L.; Uchida, T.K.; Habib, A.; Dembia, C.L.; Dunne, J.J.; Ong, C.F.; DeMers, M.S.; Rajagopal, A.; Millard, M.; et al. OpenSim: Simulating Musculoskeletal Dynamics and Neuromuscular Control to Study Human and Animal Movement. PLoS Comput. Biol. 2018, 14, e1006223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, K.R.; Myer, G.D.; Toms, H.E.; Hewett, T.E. Gender Differences in the Kinematics of Unanticipated Cutting in Young Athletes. Med. Sci. Sports Exerc. 2005, 37, 124–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugan, S.A.; Bhat, K.P. Biomechanics and Analysis of Running Gait. Phys. Med. Rehabil. Clin. N. Am. 2005, 16, 603–621. [Google Scholar] [CrossRef] [PubMed]
- Andriacchi, T.P.; Alexander, E.J. Studies of Human Locomotion: Past, Present and Future. J. Biomech. 2000, 33, 1217–1224. [Google Scholar] [CrossRef]
- Brach, J.S.; Berlin, J.E.; VanSwearingen, J.M.; Newman, A.B.; Studenski, S.A. Too Much or Too Little Step Width Variability Is Associated with a Fall History in Older Persons Who Walk at or near Normal Gait Speed. J. Neuroeng. Rehabil. 2005, 2, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamacher, D.; Singh, N.B.; Van Dieën, J.H.; Heller, M.O.; Taylor, W.R. Kinematic Measures for Assessing Gait Stability in Elderly Individuals: A Systematic Review. J. R. Soc. Interface 2011, 8, 1682–1698. [Google Scholar] [CrossRef]
- Cavanagh, P.R.; Kram, R. Stride Length in Distance Running: Velocity, Body Dimensions, and Added Mass Effects. Med. Sci. Sports Exerc. 1989, 21, 467–479. [Google Scholar] [CrossRef]
- Novacheck, T.F. The Biomechanics of Running. Gait Posture 1998, 7, 77–95. [Google Scholar] [CrossRef]
- Davis, R.B., III; Õunpuu, S.; Tyburski, D.; Gage, J.R. A Gait Analysis Data Collection and Reduction Technique. Hum. Mov. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Cimolin, V.; Galli, M. Summary Measures for Clinical Gait Analysis: A Literature Review. Gait Posture 2014, 39, 1005–1010. [Google Scholar] [CrossRef]
- Ranavolo, A.; Draicchio, F.; Varrecchia, T.; Silvetti, A.; Iavicoli, S. Wearable Monitoring Devices for Biomechanical Risk Assessment at Work: Current Status and Future Challenges—A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 2001. [Google Scholar] [CrossRef] [Green Version]
- Pannurat, N.; Thiemjarus, S.; Nantajeewarawat, E. Automatic Fall Monitoring: A Review. Sensors 2014, 14, 12900–12936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Titterton, D.H.; Weston, J.L. Strapdown Inertial Navigation Technology; IET: London, UK, 2004; Volume 17, ISBN 0863413587. [Google Scholar]
- Angelo, M. Sabatini Quaternion-Based Extended Kalman Filter for Determining Orientation by Inertial and Magnetic Sensing. IEEE Trans. Biomed. Eng. 2006, 53, 1346–1356. [Google Scholar]
- O’Donovan, K.J.; Kamnik, R.; O’Keeffe, D.T.; Lyons, G.M. An Inertial and Magnetic Sensor Based Technique for Joint Angle Measurement. J. Biomech. 2007, 40, 2604–2611. [Google Scholar] [CrossRef] [PubMed]
- Schepers, M.; Giuberti, M.; Bellusci, G. Xsens MVN: Consistent Tracking of Human Motion Using Inertial Sensing. Xsens Technol. 2018, 1–8. [Google Scholar]
- Šlajpah, S.; Kamnik, R.; Munih, M. Kinematics Based Sensory Fusion for Wearable Motion Assessment in Human Walking. Comput. Methods Programs Biomed. 2014, 116, 131–144. [Google Scholar] [CrossRef]
- Picerno, P. 25 Years of Lower Limb Joint Kinematics by Using Inertial and Magnetic Sensors: A Review of Methodological Approaches. Gait Posture 2017, 51, 239–246. [Google Scholar] [CrossRef]
- de Vries, W.H.K.; Veeger, H.E.J.; Baten, C.T.M.; van der Helm, F.C.T. Magnetic Distortion in Motion Labs, Implications for Validating Inertial Magnetic Sensors. Gait Posture 2009, 29, 535–541. [Google Scholar] [CrossRef]
- Seel, T.; Raisch, J.; Schauer, T. IMU-Based Joint Angle Measurement for Gait Analysis. Sensors 2014, 14, 6891–6909. [Google Scholar] [CrossRef] [Green Version]
- Vitali, R.V.; Cain, S.M.; McGinnis, R.S.; Zaferiou, A.M.; Ojeda, L.V.; Davidson, S.P.; Perkins, N.C. Method for Estimating Three-Dimensional Knee Rotations Using Two Inertial Measurement Units: Validation with a Coordinate Measurement Machine. Sensors 2017, 17, 1970. [Google Scholar] [CrossRef] [Green Version]
- Teufl, W.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Validity, Test-Retest Reliability and Long-Term Stability of Magnetometer Free Inertial Sensor Based 3D Joint Kinematics. Sensors 2018, 18, 1980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGrath, T.; Stirling, L. Body-Worn Imu Human Skeletal Pose Estimation Using a Factor Graph-Based Optimization Framework. Sensors 2020, 20, 6887. [Google Scholar] [CrossRef] [PubMed]
- Weygers, I.; Kok, M.; De Vroey, H.; Verbeerst, T.; Versteyhe, M.; Hallez, H.; Claeys, K. Drift-Free Inertial Sensor-Based Joint Kinematics for Long-Term Arbitrary Movements. IEEE Sens. J. 2020, 20, 7969–7979. [Google Scholar] [CrossRef] [Green Version]
- Weygers, I.; Kok, M.; Konings, M.; Hallez, H.; De Vroey, H.; Claeys, K. Inertial Sensor-Based Lower Limb Joint Kinematics: A Methodological Systematic Review. Sensors 2020, 20, 673. [Google Scholar] [CrossRef] [Green Version]
- Potter, M.V.; Ojeda, L.V.; Perkins, N.C.; Cain, S.M. Effect of IMU Design on IMU-Derived Stride Metrics for Running. Sensors 2019, 19, 2601. [Google Scholar] [CrossRef] [Green Version]
- Blair, S.; Duthie, G.; Robertson, S.; Hopkins, W.; Ball, K. Concurrent Validation of an Inertial Measurement System to Quantify Kicking Biomechanics in Four Football Codes. J. Biomech. 2018, 73, 24–32. [Google Scholar] [CrossRef]
- Teufl, W.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Validity of Inertial Sensor Based 3D Joint Kinematics of Static and Dynamic Sport and Physiotherapy Specific Movements. PLoS ONE 2019, 14, e0213064. [Google Scholar] [CrossRef] [Green Version]
- Adamowicz, L.; Gurchiek, R.D.; Ferri, J.; Ursiny, A.T.; Fiorentino, N.; McGinnis, R.S. Validation of Novel Relative Orientation and Inertial Sensor-to-Segment Alignment Algorithms for Estimating 3D Hip Joint Angles. Sensors 2019, 19, 5143. [Google Scholar] [CrossRef] [Green Version]
- Mavor, M.P.; Ross, G.B.; Clouthier, A.L.; Karakolis, T.; Graham, R.B. Validation of an IMU Suit for Military-Based Tasks. Sensors 2020, 20, 4280. [Google Scholar] [CrossRef]
- Ojeda, L.V.; Zaferiou, A.M.; Cain, S.M.; Vitali, R.V.; Davidson, S.P.; Stirling, L.A.; Perkins, N.C. Estimating Stair Running Performance Using Inertial Sensors. Sensors 2017, 17, 2647. [Google Scholar] [CrossRef] [Green Version]
- Ahmadi, A.; Destelle, F.; Unzueta, L.; Monaghan, D.S.; Linaza, M.T.; Moran, K.; O’Connor, N.E. 3D Human Gait Reconstruction and Monitoring Using Body-Worn Inertial Sensors and Kinematic Modeling. IEEE Sens. J. 2016, 16, 8823–8831. [Google Scholar] [CrossRef]
- Fasel, B.; Spörri, J.; Schütz, P.; Lorenzetti, S.; Aminian, K. Validation of Functional Calibration and Strap-down Joint Drift Correction for Computing 3D Joint Angles of Knee, Hip, and Trunk in Alpine Skiing. PLoS ONE 2017, 12, e0181446. [Google Scholar] [CrossRef] [PubMed]
- Rapp, E.; Shin, S.; Thomsen, W.; Ferber, R.; Halilaj, E. Estimation of Kinematics from Inertial Measurement Units Using a Combined Deep Learning and Optimization Framework. J. Biomech. 2021, 116, 110229. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.; Kim, B.; Park, S. Prediction of Lower Limb Kinetics and Kinematics during Walking by a Single IMU on the Lower Back Using Machine Learning. Sensors 2020, 20, 130. [Google Scholar] [CrossRef] [Green Version]
- Mundt, M.; Koeppe, A.; David, S.; Witter, T.; Bamer, F.; Potthast, W.; Markert, B. Estimation of Gait Mechanics Based on Simulated and Measured IMU Data Using an Artificial Neural Network. Front. Bioeng. Biotechnol. 2020, 8, 41. [Google Scholar] [CrossRef] [PubMed]
- Potter, M.V.; Cain, S.M.; Ojeda, L.V.; Gurchiek, R.D.; McGinnis, R.S.; Perkins, N.C. Error-State Kalman Filter for Lower-Body Kinematic Estimation: Evaluation on a 3-Body Model. PLoS ONE 2021, 16, e0249577. [Google Scholar] [CrossRef]
- Vitali, R.V.; Perkins, N.C. Determining Anatomical Frames via Inertial Motion Capture: A Survey of Methods. J. Biomech. 2020, 106, 109832. [Google Scholar] [CrossRef]
- Olsson, F.; Kok, M.; Seel, T.; Halvorsen, K. Robust Plug-and-Play Joint Axis Estimation Using Inertial Sensors. Sensors 2020, 20, 3534. [Google Scholar] [CrossRef]
- Seel, T.; Kok, M.; McGinnis, R.S. Inertial Sensors—Applications and Challenges in a Nutshell. Sensors 2020, 20, 6221. [Google Scholar] [CrossRef]
- Sola, J. Quaternion Kinematics for the Error-State KF. arXiv 2017, arXiv:1711.02508. Available online: https://arxiv.org/abs/1711.02508 (accessed on 3 January 2019).
- Madyastha, V.K.; Ravindray, V.C.; Mallikarjunan, S.; Goyal, A. Extended Kalman Filter vs. Error State Kalman Filter for Aircraft Attitude Estimation. AIAA Guid. Navig. Control. Conf. 2011, 2011, 6615. [Google Scholar] [CrossRef]
- Ojeda, L.; Borenstein, J. Non-GPS Navigation for Security Personnel and First Responders. J. Navig. 2007, 60, 391–407. [Google Scholar] [CrossRef] [Green Version]
- Foxlin, E. Pedestrian Tracking with Shoe-Mounted Inertial Sensors. IEEE Comput. Graph. Appl. 2005, 25, 38–46. [Google Scholar] [CrossRef]
- Miezal, M.; Taetz, B.; Bleser, G. On Inertial Body Tracking in the Presence of Model Calibration Errors. Sensors 2016, 16, 1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camomilla, V.; Cereatti, A.; Vannozzi, G.; Cappozzo, A. An Optimized Protocol for Hip Joint Centre Determination Using the Functional Method. J. Biomech. 2006, 39, 1096–1106. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Measuring Agreement in Method Comparison Studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Delp, S.L.; Loan, J.P.; Hoy, M.G.; Zajac, F.E.; Topp, E.L.; Rosen, J.M. An Interactive Graphics-Based Model of the Lower Extremity to Study Orthopaedic Surgical Procedures. IEEE Trans. Biomed. Eng. 1990, 37, 757–767. [Google Scholar] [CrossRef]
- Delp, S.L.; Anderson, F.C.; Arnold, A.S.; Loan, P.; Habib, A.; John, C.T.; Guendelman, E.; Thelen, D.G. OpenSim: Open-Source Software to Create and Analyze Dynamic Simulations of Movement. IEEE Trans. Biomed. Eng. 2007, 54, 1940–1950. [Google Scholar] [CrossRef] [Green Version]
- Grood, E.S.; Suntay, W.J. A Joint Coordinate System for the Clinical Description of Three-Dimensional Motions: Application to the Knee. J. Biomech. Eng. 1983, 105, 136–144. [Google Scholar] [CrossRef]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB Recommendation on Definitions of Joint Coordinate System of Various Joints for the Reporting of Human Joint Motion—Part I: Ankle, Hip, and Spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Dabirrahmani, D.; Hogg, M. Modification of the Grood and Suntay Joint Coordinate System Equations for Knee Joint Flexion. Med. Eng. Phys. 2017, 39, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Roach, K.E.; Miles, T.P. Normal Hip and Knee Active Range of Motion: The Relationship to Age. Phys. Ther. 1991, 71, 656–665. [Google Scholar] [CrossRef] [PubMed]
- Verrall, G.M.; Slavotinek, J.P.; Barnes, P.G.; Esterman, A.; Oakeshott, R.D.; Spriggins, A.J. Hip Joint Range of Motion Restriction Precedes Athletic Chronic Groin Injury. J. Sci. Med. Sport 2007, 10, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Qu, X.; Yeo, J.C. Effects of Load Carriage and Fatigue on Gait Characteristics. J. Biomech. 2011, 44, 1259–1263. [Google Scholar] [CrossRef]
- Teufl, W.; Lorenz, M.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Towards Inertial Sensor Based Mobile Gait Analysis: Event-Detection and Spatio-Temporal Parameters. Sensors 2019, 19, 38. [Google Scholar] [CrossRef] [Green Version]
- Hara, R.; McGinley, J.; Briggs, C.; Baker, R.; Sangeux, M. Predicting the Location of the Hip Joint Centres, Impact of Age Group and Sex. Sci. Rep. 2016, 6, 37707. [Google Scholar] [CrossRef] [Green Version]
- Siston, R.A.; Daub, A.C.; Giori, N.J.; Goodman, S.B.; Delp, S.L. Evaluation of Methods That Locate the Center of the Ankle for Computer-Assisted Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 2005, 129–135. [Google Scholar] [CrossRef]
- Challis, J.H. A Procedure for Determining Rigid Body Transformation Parameters. J. Biomech. 1995, 28, 733–737. [Google Scholar] [CrossRef]
- Getting Started with Inverse Kinematics. Available online: https://simtk-confluence.stanford.edu/display/OpenSim/Getting+Started+with+Inverse+Kinematics#GettingStartedwithInverseKinematics-BestPracticesandTroubleshooting (accessed on 2 February 2021).
- Carmo, A.; Kleiner, A.; Costa, P.; Barros, R. Three-Dimensional Kinematic Analysis of Upper and Lower Limb Motion during Gait of Post-Stroke Patients. Braz. J. Med. Biol. Res. 2012, 45, 537–545. [Google Scholar] [CrossRef] [Green Version]
- Chapman, R.M.; Moschetti, W.E.; van Citters, D.W. Stance and Swing Phase Knee Flexion Recover at Different Rates Following Total Knee Arthroplasty: An Inertial Measurement Unit Study. J. Biomech. 2019, 84, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Bergamini, E.; Ligorio, G.; Summa, A.; Vannozzi, G.; Cappozzo, A.; Sabatini, A.M. Estimating Orientation Using Magnetic and Inertial Sensors and Different Sensor Fusion Approaches: Accuracy Assessment in Manual and Locomotion Tasks. Sensors 2014, 14, 18625–18649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeVita, P.; Hortobagyi, T. Age Causes a Redistribution of Joint Torques and Powers during Gait. J. Appl. Physiol. 2000, 88, 1804–1811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sofuwa, O.; Nieuwboer, A.; Desloovere, K.; Willems, A.-M.; Chavret, F.; Jonkers, I. Quantitative Gait Analysis in Parkinson’s Disease: Comparison with a Healthy Control Group. Arch. Phys. Med. Rehabil. 2005, 86, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.T.; Novak, A.C.; Brouwer, B.; Li, Q. Concurrent Validation of Xsens MVN Measurement of Lower Limb Joint Angular Kinematics. Physiol. Meas. 2013, 34, N63–N69. [Google Scholar] [CrossRef]
- Nüesch, C.; Roos, E.; Pagenstert, G.; Mündermann, A. Measuring Joint Kinematics of Treadmill Walking and Running: Comparison between an Inertial Sensor Based System and a Camera-Based System. J. Biomech. 2017, 57, 32–38. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Noise Parameter | (m/s2) | (deg/s) | (m/s) | (deg) | (m) | (deg) | (deg) |
|---|---|---|---|---|---|---|---|
| Value | 0.013 | 2.83 | 0.01 | 5.73 | 0.01 | 1.15 | 57.3 |
| Normal | Fast | Slow | Back | Left | Right | |
|---|---|---|---|---|---|---|
| RHip FE | 2.54 (1.23) | 2.28 (0.86) | 2.21 (0.80) | 2.34 (1.18) | 2.80 (1.89) | 2.94 (1.94) |
| LHip FE | 2.17 (0.89) | 2.25 (0.83) | 2.40 (1.44) | 2.61 (1.22) | 3.00 (1.61) | 2.63 (1.41) |
| RKnee FE | 3.13 (1.06) | 3.37 (0.83) | 3.07 (1.21) | 3.10 (1.13) | 3.77 (1.96) | 3.65 (1.78) |
| LKnee FE | 3.16 (1.05) | 3.52 (1.37) | 2.99 (1.17) | 3.07 (1.33) | 3.71 (1.13) | 3.05 (1.18) |
| RAnkle DP | 4.24 (1.81) | 3.99 (1.70) | 5.03 (2.04) | 5.50 (1.80) | 6.32 (1.98) | 6.00 (1.89) |
| LAnkle DP | 3.00 (1.23) | 3.13 (1.15) | 3.41 (1.22) | 2.87 (1.51) | 3.31 (1.63) | 3.02 (1.53) |
| RHip IE | 7.40 (3.56) | 6.08 (3.00) | 7.40 (5.75) | 10.55 (9.44) | 8.30 (9.52) | 9.44 (8.45) |
| LHip IE | 7.47 (7.60) | 6.57 (4.68) | 11.97 (12.76) | 11.45 (10.89) | 10.35 (7.83) | 8.17 (7.89) |
| RKnee IE | 8.83 (3.88) | 7.96 (4.00) | 8.21 (3.60) | 8.48 (2.95) | 6.87 (3.28) | 7.34 (3.47) |
| LKnee IE | 7.29 (6.96) | 6.74 (6.59) | 7.63 (8.05) | 8.29 (7.27) | 9.83 (8.76) | 9.38 (8.12) |
| RAnkle IE | 2.72 (1.10) | 2.40 (0.85) | 3.83 (1.90) | 2.81 (1.38) | 3.74 (1.82) | 4.15 (1.79) |
| LAnkle IE | 3.14 (1.76) | 2.58 (1.35) | 3.85 (1.75) | 3.10 (1.75) | 3.19 (1.95) | 3.29 (1.77) |
| RHip AbAd | 4.15 (2.13) | 3.49 (1.69) | 3.52 (2.25) | 3.85 (3.02) | 3.43 (2.70) | 4.04 (3.36) |
| LHip AbAd | 3.45 (2.05) | 3.40 (1.66) | 4.07 (2.32) | 3.67 (1.76) | 4.09 (1.93) | 2.92 (1.28) |
| RKnee AbAd | 4.62 (3.40) | 4.52 (3.36) | 4.24 (3.70) | 3.38 (3.40) | 3.16 (2.91) | 3.64 (3.54) |
| LKnee AbAd | 4.60 (1.68) | 4.46 (1.84) | 4.31 (1.64) | 3.85 (1.74) | 3.62 (1.56) | 3.62 (1.64) |
| RAnkle InEv | 2.61 (0.79) | 2.72 (0.80) | 2.70 (1.00) | 1.96 (0.68) | 2.42 (0.66) | 2.58 (0.67) |
| LAnkle InEv | 2.40 (0.94) | 2.35 (1.16) | 2.51 (0.88) | 2.00 (1.07) | 2.08 (0.68) | 2.27 (0.89) |
| Normal | Fast | Slow | Back | Left | Right | |
|---|---|---|---|---|---|---|
| RHip FE | 7.03 (4.37) | 7.16 (4.21) | 5.96 (4.49) | 6.33 (4.53) | 5.67 (4.52) | 6.03 (4.73) |
| LHip FE | 7.23 (4.03) | 7.00 (3.71) | 6.75 (3.85) | 6.97 (4.55) | 6.33 (4.09) | 6.73 (4.46) |
| RKnee FE | 4.36 (2.14) | 4.74 (2.10) | 4.16 (2.26) | 4.35 (1.89) | 4.50 (2.14) | 4.64 (2.09) |
| LKnee FE | 3.79 (1.26) | 4.14 (1.26) | 3.37 (1.54) | 4.18 (1.48) | 4.15 (1.63) | 3.84 (1.70) |
| RAnkle DP | 5.41 (2.98) | 5.48 (3.07) | 5.40 (2.92) | 5.20 (2.64) | 4.33 (2.46) | 4.92 (2.61) |
| LAnkle DP | 5.28 (2.14) | 5.64 (2.22) | 4.76 (2.35) | 3.52 (1.87) | 4.62 (4.13) | 3.59 (1.77) |
| RHip IE | 7.43 (3.59) | 6.19 (2.55) | 8.50 (6.43) | 11.26 (10.24) | 9.58 (8.54) | 11.03 (9.44) |
| LHip IE | 8.56 (7.43) | 7.21 (4.95) | 13.54 (13.34) | 12.67 (11.30) | 11.61 (9.19) | 9.28 (8.41) |
| RKnee IE | 5.91 (2.71) | 5.66 (2.34) | 5.98 (3.01) | 6.12 (3.30) | 5.81 (3.27) | 5.83 (3.08) |
| LKnee IE | 7.32 (5.20) | 7.70 (5.11) | 6.87 (5.93) | 7.43 (5.94) | 8.62 (6.79) | 7.66 (6.01) |
| RAnkle IE | 4.23 (2.32) | 4.49 (1.28) | 4.39 (2.06) | 3.90 (2.49) | 4.81 (3.30) | 3.89 (2.55) |
| LAnkle IE | 4.76 (2.68) | 5.35 (2.72) | 4.49 (2.43) | 3.73 (2.30) | 4.87 (3.93) | 4.17 (1.82) |
| RHip AbAd | 4.74 (2.04) | 4.53 (1.77) | 4.33 (1.35) | 3.88 (1.96) | 3.39 (1.61) | 4.51 (1.79) |
| LHip AbAd | 4.37 (1.47) | 4.44 (1.47) | 4.64 (1.78) | 4.00 (1.41) | 4.27 (1.65) | 3.52 (1.63) |
| RKnee AbAd | 3.99 (1.53) | 4.26 (1.66) | 3.17 (1.22) | 2.65 (1.28) | 2.65 (1.63) | 2.67 (1.35) |
| LKnee AbAd | 3.90 (2.06) | 3.72 (1.81) | 3.26 (1.88) | 3.73 (1.97) | 2.96 (1.61) | 3.55 (2.06) |
| RAnkle InEv | 4.56 (1.32) | 4.94 (1.51) | 4.88 (1.32) | 5.79 (1.57) | 6.27 (1.22) | 6.07 (1.80) |
| LAnkle InEv | 4.70 (1.50) | 5.16 (1.72) | 4.42 (1.18) | 4.71 (1.68) | 5.35 (1.89) | 5.48 (2.11) |
| Normal | Fast | Slow | Back | Left | Right | |
|---|---|---|---|---|---|---|
| RHip FE | 1.22 (0.36) | 1.60 (0.69) | 1.35 (0.57) | 2.26 (0.85) | 2.39 (1.89) | 1.58 (0.58) |
| LHip FE | 1.69 (1.54) | 1.69 (1.32) | 3.59 (4.82) | 2.74 (2.31) | 2.19 (1.23) | 1.86 (1.20) |
| RHip IE | 1.98 (0.99) | 1.98 (0.71) | 2.41 (0.87) | 2.53 (1.06) | 3.28 (1.60) | 3.22 (1.53) |
| LHip IE | 2.15 (0.80) | 2.10 (0.64) | 2.41 (0.92) | 3.15 (1.04) | 2.92 (1.22) | 2.54 (1.04) |
| RHip AbAd | 3.14 (1.84) | 2.98 (2.08) | 2.51 (1.61) | 2.27 (0.98) | 2.97 (1.22) | 2.26 (0.96) |
| LHip AbAd | 3.29 (3.19) | 2.24 (1.75) | 4.24 (4.99) | 3.02 (3.27) | 2.58 (1.97) | 2.77 (1.21) |
| Normal | Fast | Slow | Back | Left | Right | |
|---|---|---|---|---|---|---|
| RHip FE | 4.17 (2.40) | 4.61 (2.72) | 3.26 (1.85) | 3.70 (2.38) | 2.13 (0.88) | 2.44 (0.90) |
| LHip FE | 4.14 (2.07) | 4.56 (2.33) | 4.59 (4.25) | 2.94 (1.99) | 2.33 (0.99) | 2.21 (1.02) |
| RHip IE | 5.22 (2.75) | 5.53 (2.50) | 4.84 (2.89) | 4.05 (2.17) | 5.92 (3.58) | 4.20 (2.26) |
| LHip IE | 4.77 (2.71) | 5.28 (2.21) | 4.49 (2.77) | 4.13 (2.42) | 3.69 (1.43) | 5.93 (2.82) |
| RHip AbAd | 3.48 (2.20) | 4.40 (2.66) | 3.29 (2.30) | 3.28 (1.58) | 2.43 (1.51) | 2.36 (1.45) |
| LHip AbAd | 4.30 (1.88) | 5.71 (2.42) | 4.41 (2.42) | 4.00 (2.43) | 2.74 (2.40) | 2.69 (1.39) |
| RKnee FE | 4.62 (2.65) | 4.37 (2.65) | 4.53 (2.71) | 3.01 (1.88) | 2.94 (1.84) | 2.88 (1.08) |
| LKnee FE | 3.44 (2.22) | 2.89 (2.18) | 3.61 (2.12) | 2.92 (1.50) | 3.14 (1.10) | 2.57 (0.98) |
| RKneeIE | 4.88 (2.60) | 5.43 (3.41) | 3.14 (2.15) | 3.61 (1.74) | 4.21 (1.44) | 3.90 (1.61) |
| LKnee IE | 4.71 (2.05) | 5.16 (1.74) | 3.16 (1.43) | 3.28 (1.39) | 4.85 (2.06) | 4.61 (1.64) |
| RKnee AbAd | 5.77 (4.36) | 6.85 (5.11) | 4.00 (2.66) | 2.35 (1.52) | 1.51 (0.87) | 1.89 (0.80) |
| LKnee AbAd | 3.70 (3.01) | 3.81 (2.69) | 3.66 (2.67) | 2.71 (1.47) | 2.05 (1.09) | 1.99 (0.82) |
| RAnkle DP | 4.49 (2.29) | 5.38 (2.26) | 3.63 (2.10) | 2.50 (1.23) | 2.33 (0.65) | 2.51 (1.54) |
| LAnkle DP | 5.26 (2.80) | 6.21 (2.93) | 3.05 (1.71) | 1.84 (0.87) | 5.36 (11.45) | 2.14 (1.07) |
| RAnkle IE | 8.21 (3.18) | 9.33 (2.78) | 6.71 (2.77) | 4.05 (1.39) | 3.71 (1.59) | 3.15 (1.81) |
| LAnkle IE | 8.90 (3.89) | 10.57 (3.05) | 6.86 (3.01) | 3.33 (1.74) | 5.69 (11.62) | 2.76 (1.76) |
| RAnkle InEv | 3.79 (1.72) | 3.22 (1.16) | 4.89 (1.99) | 5.65 (2.49) | 6.10 (2.73) | 7.21 (3.22) |
| LAnkle InEv | 5.27 (2.75) | 4.52 (2.57) | 5.77 (3.27) | 5.62 (2.45) | 7.57 (3.45) | 5.66 (2.31) |
| Normal | Fast | Slow | Back | Left | Right | |
|---|---|---|---|---|---|---|
| SL RMS Diff | 0.07 (0.03) | 0.05 (0.02) | 0.16 (0.05) | 0.11 (0.05) | 0.07 (0.03) | 0.06 (0.02) |
| Mean SL | 1.09 (0.15) | 1.40 (0.17) | 0.84 (0.15) | 0.62 (0.15) | 0.48 (0.08) | 0.46 (0.08) |
| % Diff SL | 6.0% | 3.4% | 19.1% | 17.6% | 15.5% | 13.3% |
| SW RMS Diff | 0.05 (0.02) | 0.05 (0.02) | 0.07 (0.04) | 0.12 (0.06) | 0.10 (0.08) | 0.09 (0.05) |
| Mean SW | 0.12 (0.03) | 0.11 (0.03) | 0.13 (0.03) | 0.15 (0.03) | 0.01 (0.02) | 0.00 (0.02) |
| % Diff SW | 40.4% | 43.1% | 57.4% | 80.8% | NA | NA |
| Belt Speed | 0.86 (0.17) | 1.32 (0.21) | 0.47 (0.09) | 0.43 (0.08) | 0.39 (0.07) | 0.38 (0.08) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Potter, M.V.; Cain, S.M.; Ojeda, L.V.; Gurchiek, R.D.; McGinnis, R.S.; Perkins, N.C. Evaluation of Error-State Kalman Filter Method for Estimating Human Lower-Limb Kinematics during Various Walking Gaits. Sensors 2022, 22, 8398. https://doi.org/10.3390/s22218398
Potter MV, Cain SM, Ojeda LV, Gurchiek RD, McGinnis RS, Perkins NC. Evaluation of Error-State Kalman Filter Method for Estimating Human Lower-Limb Kinematics during Various Walking Gaits. Sensors. 2022; 22(21):8398. https://doi.org/10.3390/s22218398
Chicago/Turabian StylePotter, Michael V., Stephen M. Cain, Lauro V. Ojeda, Reed D. Gurchiek, Ryan S. McGinnis, and Noel C. Perkins. 2022. "Evaluation of Error-State Kalman Filter Method for Estimating Human Lower-Limb Kinematics during Various Walking Gaits" Sensors 22, no. 21: 8398. https://doi.org/10.3390/s22218398