
Fall Prediction Based on Instrumented Measures of Gait and Turning in Daily Life in People with Multiple Sclerosis

 ,
, 
_Carlson-Kuhta.jpg) ,
,
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Demographics
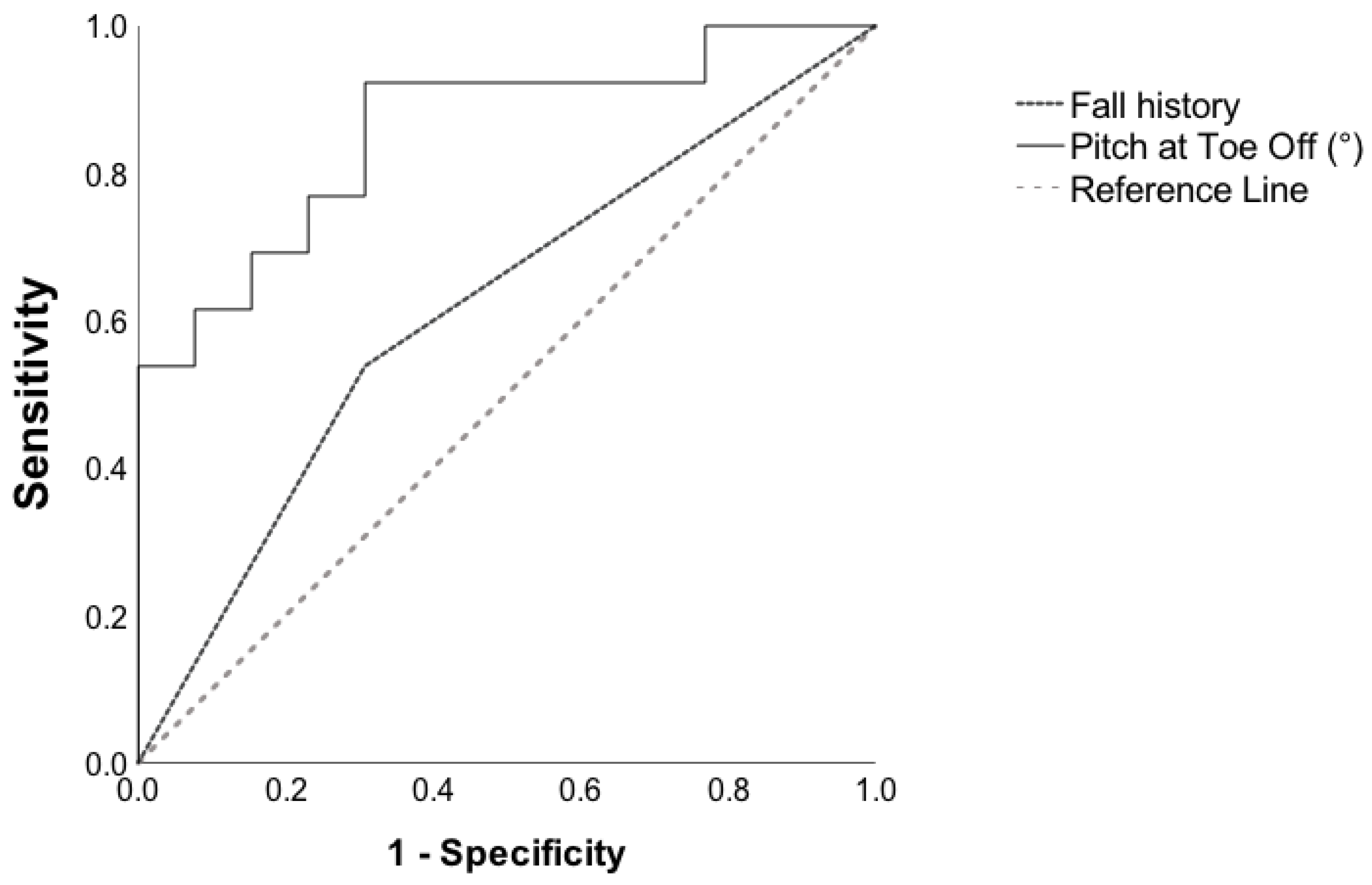
3.2. Fall Prediction Based on Instrumented Measures of Mobility
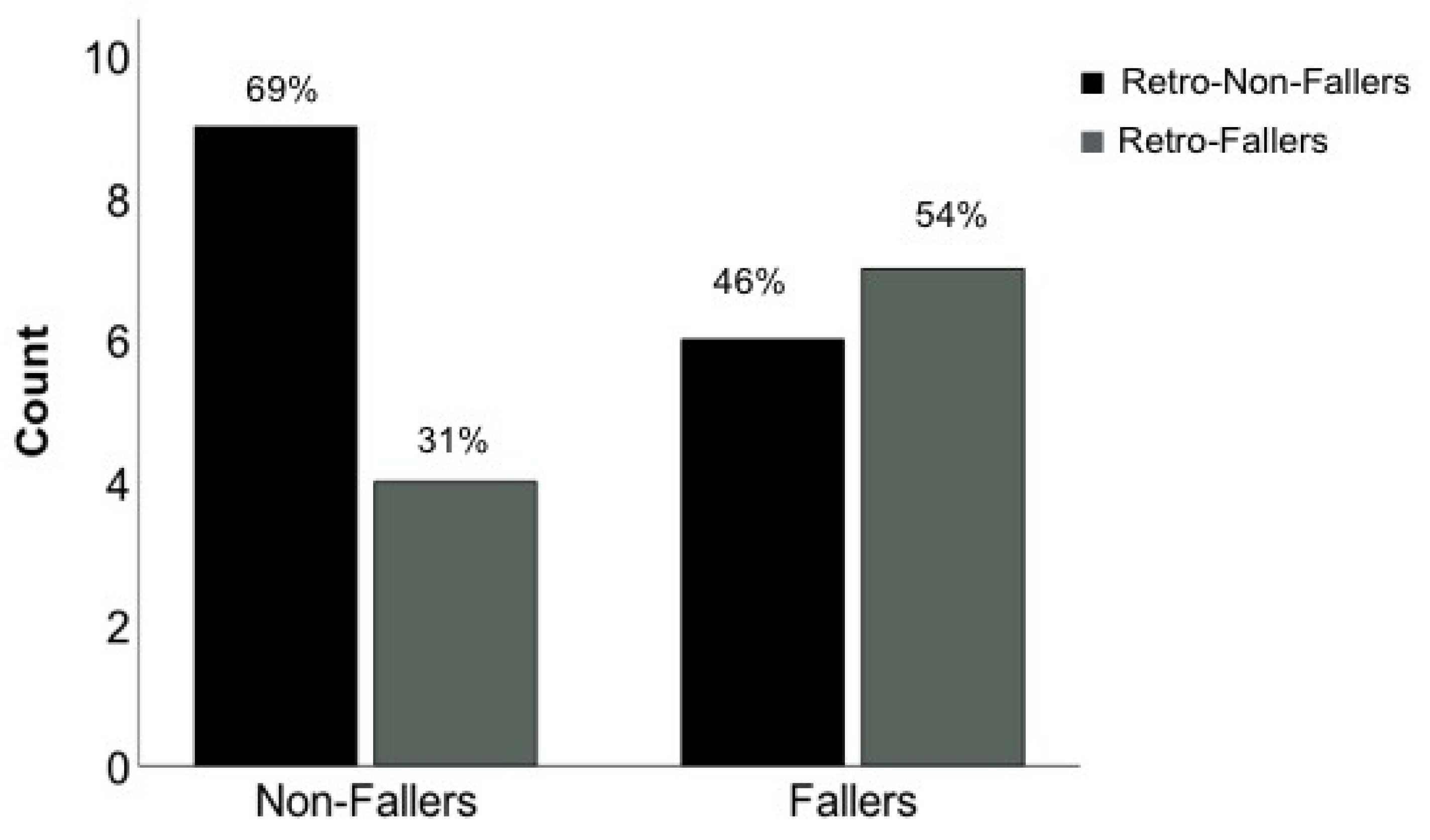
3.3. Fall Prediction Based on the History of Falls
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hauser, S.L.; Oksenberg, J.R. The neurobiology of multiple sclerosis: Genes, inflammation, and neurodegeneration. Neuron 2006, 52, 61–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trapp, B.D.; Nave, K.A. Multiple sclerosis: An immune or neurodegenerative disorder? Annu. Rev. Neurosci. 2008, 31, 247–269. [Google Scholar] [CrossRef] [PubMed]
- Nilsagård, Y.; Gunn, H.; Freeman, J.; Hoang, P.; Lord, S.; Mazumder, R.; Cameron, M. Falls in people with MS—An individual data meta-analysis from studies from Australia, Sweden, United Kingdom and the United States. Mult. Scler. J. 2015, 21, 92–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsagård, Y.; Lundholm, C.; Denison, E.; Gunnarsson, L.G. Predicting accidental falls in people with multiple sclerosis—A longitudinal study. Clin. Rehabil. 2009, 23, 259–269. [Google Scholar] [CrossRef]
- Quinn, G.; Comber, L.; Galvin, R.; Coote, S. The ability of clinical balance measures to identify falls risk in multiple sclerosis: A systematic review and meta-analysis. Clin. Rehabil. 2018, 32, 571–582. [Google Scholar] [CrossRef]
- Chinnadurai, S.A.; Gandhirajan, D.; Srinivasan, A.V.; Kesavamurthy, B.; Ranganathan, L.N.; Pamidimukkala, V. Predicting falls in multiple sclerosis: Do electrophysiological measures have a better predictive accuracy compared to clinical measures? Mult. Scler. Relat. Disord. 2018, 20, 199–203. [Google Scholar] [CrossRef]
- Sosnoff, J.J.; Socie, M.J.; Boes, M.K.; Sandroff, B.M.; Pula, J.H.; Suh, Y.; Weikert, M.; Balantrapu, S.; Morrison, S.; Motl, R.W. Mobility, balance and falls in persons with multiple sclerosis. PLoS ONE 2011, 6, e28021. [Google Scholar] [CrossRef] [Green Version]
- Gunn, H.J.; Newell, P.; Haas, B.; Marsden, J.F.; Freeman, J.A. Identification of risk factors for falls in multiple sclerosis: A systematic review and meta-analysis. Phys. Ther. 2013, 93, 504–513. [Google Scholar] [CrossRef]
- Peterson, E.W.; Ben Ari, E.; Asano, M.; Finlayson, M.L. Fall attributions among middle-aged and older adults with multiple sclerosis. Arch. Phys. Med. Rehabil. 2013, 94, 890–895. [Google Scholar] [CrossRef]
- Mazumder, R.; Murchison, C.; Bourdette, D.; Cameron, M. Falls in people with multiple sclerosis compared with falls in healthy controls. PLoS ONE 2014, 9, e107620. [Google Scholar] [CrossRef]
- Spain, R.I.; St George, R.J.; Salarian, A.; Mancini, M.; Wagner, J.M.; Horak, F.B.; Bourdette, D. Body-worn motion sensors detect balance and gait deficits in people with multiple sclerosis who have normal walking speed. Gait Posture 2012, 35, 573–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradshaw, M.J.; Farrow, S.; Motl, R.W.; Chitnis, T. Wearable biosensors to monitor disability in multiple sclerosis. Neurol. Clin. Pract. 2017, 7, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Schwenk, M.; Mohler, J.; Wendel, C.; D’Huyvetter, K.; Fain, M.; Taylor-Piliae, R.; Najafi, B. Wearable sensor-based in-home assessment of gait, balance, and physical activity for discrimination of frailty status: Baseline results of the Arizona frailty cohort study. Gerontology 2015, 61, 258–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernhard, F.P.; Sartor, J.; Bettecken, K.; Hobert, M.A.; Arnold, C.; Weber, Y.G.; Poli, S.; Margraf, N.G.; Schlenstedt, C.; Hansen, C.; et al. Wearables for gait and balance assessment in the neurological ward-study design and first results of a prospective cross-sectional feasibility study with 384 inpatients. BMC Neurol. 2018, 18, 114. [Google Scholar] [CrossRef] [PubMed]
- Manor, B.; Yu, W.; Zhu, H.; Harrison, R.; Lo, O.-Y.; Lipsitz, L.; Travison, T.; Pascual-Leone, A.; Zhou, J. Smartphone App-Based Assessment of Gait During Normal and Dual-Task Walking: Demonstration of Validity and Reliability. JMIR mHealth uHealth 2018, 6, e36. [Google Scholar] [CrossRef] [PubMed]
- Berg-Hansen, P.; Moen, S.M.; Austeng, A.; Gonzales, V.; Klyve, T.D.; Negård, H.; Seeberg, T.M.; Celius, E.G.; Meyer, F. Sensor-based gait analyses of the six-minute walk test identify qualitative improvement in gait parameters of people with multiple sclerosis after rehabilitation. J. Neurol. 2022, 269, 1–12. [Google Scholar] [CrossRef]
- Cameron, M.H. Predicting falls in people with multiple sclerosis: Fall history is as accurate as more complex measures. Mult. Scler. Int. 2013, 2013, 496325. [Google Scholar] [CrossRef] [Green Version]
- Shah, V.V.; McNames, J.; Mancini, M.; Carlson-Kuhta, P.; Spain, R.I.; Nutt, J.G.; El-Gohary, M.; Curtze, C.; Horak, F.B. Laboratory versus daily life gait characteristics in patients with multiple sclerosis, Parkinson’s disease, and matched controls. J. Neuroeng. Rehabil. 2020, 17, 159. [Google Scholar] [CrossRef]
- Shah, V.V.; McNames, J.; Harker, G.; Curtze, C.; Carlson-Kuhta, P.; Spain, R.I.; El-Gohary, M.; Mancini, M.; Horak, F.B. Does gait bout definition influence the ability to discriminate gait quality between people with and without multiple sclerosis during daily life? Gait Posture 2021, 84, 108–113. [Google Scholar] [CrossRef]
- El-Gohary, M.; Pearson, S.; McNames, J.; Mancini, M.; Horak, F.; Mellone, S.; Chiari, L. Continuous monitoring of turning in patients with movement disability. Sensors 2013, 14, 356–369. [Google Scholar] [CrossRef] [Green Version]
- Shah, V.V.; McNames, J.; Mancini, M.; Carlson-Kuhta, P.; Spain, R.I.; Nutt, J.G.; El-Gohary, M.; Curtze, C.; Horak, F.B. Quantity and quality of gait and turning in people with multiple sclerosis, Parkinson’s disease and matched controls during daily living. J. Neurol. 2020, 267, 1188–1196. [Google Scholar] [CrossRef] [PubMed]
- Dionyssiotis, Y. Analyzing the problem of falls among older people. Int. J. Gen. Med. 2012, 5, 805–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zecevic, A.A.; Salmoni, A.W.; Speechley, M.; Vandervoort, A.A. Defining a fall and reasons for falling: Comparisons among the views of seniors, health care providers, and the research literature. Gerontologist 2006, 46, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.L.; Lizarraga, K.J.; Waddell, E.M.; Myers, T.L.; Jensen-Roberts, S.; Modica, J.S.; Schneider, R.B. Digital Technology in Movement Disorders: Updates, Applications, and Challenges. Curr. Neurol. Neurosci. Rep. 2021, 21, 16. [Google Scholar] [CrossRef] [PubMed]
- Irrera, F.; Cabestany, J.; Suppa, A. Editorial: New Advanced Wireless Technologies for Objective Monitoring of Motor Symptoms in Parkinson’s Disease. Front. Neurol. 2018, 9, 216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, G.; Grimmer, M.; Seyfarth, A. The mechanisms and mechanical energy of human gait initiation from the lower-limb joint level perspective. Sci. Rep. 2021, 11, 22473. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.W.; Shorter, K.A.; Adamczyk, P.G.; Kuo, A.D. Mechanical and energetic consequences of reduced ankle plantar-flexion in human walking. J. Exp. Biol. 2015, 218 Pt 22, 3541–3550. [Google Scholar] [CrossRef] [Green Version]
- Ong, C.F.; Geijtenbeek, T.; Hicks, J.L.; Delp, S.L. Predicting gait adaptations due to ankle plantarflexor muscle weakness and contracture using physics-based musculoskeletal simulations. PLoS Comput. Biol. 2019, 15, e1006993. [Google Scholar] [CrossRef] [Green Version]
- Kyrdalen, I.L.; Thingstad, P.; Sandvik, L.; Ormstad, H. Associations between gait speed and well-known fall risk factors among community-dwelling older adults. Physiother. Res. Int. 2019, 24, e1743. [Google Scholar] [CrossRef] [Green Version]
- Osoba, M.Y.; Rao, A.K.; Agrawal, S.K.; Lalwani, A.K. Balance and gait in the elderly: A contemporary review. Laryngoscope Investig. Otolaryngol. 2019, 4, 143–153. [Google Scholar] [CrossRef] [Green Version]
- Kwon, M.S.; Kwon, Y.R.; Park, Y.S.; Kim, J.W. Comparison of gait patterns in elderly fallers and non-fallers. Technol. Health Care 2018, 26, 427–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortaza, N.; Abu Osman, N.A.; Mehdikhani, N. Are the spatio-temporal parameters of gait capable of distinguishing a faller from a non-faller elderly? Eur. J. Phys.Rehabil. Med. 2014, 50, 677–691. [Google Scholar] [PubMed]
- Mancini, M.; Curtze, C.; Stuart, S.; El-Gohary, M.; McNames, J.; Nutt, J.G.; Horak, F.B. The Impact Of Freezing Of Gait On Balance Perception And Mobility In Community-Living With Parkinson’S Disease. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2018, 2018, 3040–3043. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| DEMOGRAPHIC FEATURES | Faller/ | N | Mean | Std. Error | p value | |
| Non-faller | ||||||
| Age (yrs) | Non-Fallers | 13 | 49.2 | 2.4 | 0.1 | |
| Fallers | 13 | 49.1 | 3.5 | |||
| EDSS (#) | Non-Fallers | 13 | 4.3 | 0.23 | 0.8 | |
| Fallers | 13 | 4.2 | 0.18 | |||
| Weight (lbs) | Non-Fallers | 13 | 156.9 | 10.5 | 0.8 | |
| Fallers | 13 | 160.2 | 11.4 | |||
| Height (cm) | Non-Fallers | 13 | 170.2 | 2.2 | 1 | |
| Fallers | 13 | 170 | 3 | |||
| Disease Duration (yrs) | Non-Fallers | 13 | 13.8 | 2 | 0.4 | |
| Fallers | 13 | 16.8 | 2.9 | |||
| QUANTITY OF MOBILITY | Bouts/hour (#) | Non-Fallers | 13 | 5.89 | 0.91 | 0.7 |
| Fallers | 13 | 6.4 | 0.72 | |||
| Strides/hour (#) | Non-Fallers | 13 | 137.11 | 29 | 0.8 | |
| Fallers | 13 | 130.5 | 15.56 | |||
| Turns/hour (#) | Non-Fallers | 13 | 17.74 | 4.33 | 0.8 | |
| Fallers | 13 | 18.88 | 2.57 |
| Test Result Variable(s) | N | Mean | Std. Error | 95% Confidence Interval | Range | p Value | Effect Size | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Lower | Upper | Min | Max | Cohen’s d | ||||||
| Pitch at Toe Off (°) | Non-Fallers | 13 | 30.92 | 1.00 | 28.74 | 33.09 | 23.94 | 37.18 | 0.00 | 1.42 |
| Fallers | 13 | 23.88 | 1.66 | 20.26 | 27.50 | 13.73 | 33.15 | |||
| Gait Speed (m/s) | Non-Fallers | 13 | 1.08 | 0.03 | 1.01 | 1.16 | 0.90 | 1.26 | 0.01 | 1.05 |
| Fallers | 13 | 0.89 | 0.06 | 0.76 | 1.03 | 0.40 | 1.31 | |||
| Stride Length (m) | Non-Fallers | 13 | 1.22 | 0.03 | 1.15 | 1.30 | 1.00 | 1.41 | 0.01 a | 0.99 |
| Fallers | 13 | 1.06 | 0.06 | 0.93 | 1.18 | 0.68 | 1.40 | |||
| Double Support (%) | Non-Fallers | 13 | 22.70 | 0.70 | 21.17 | 24.23 | 18.48 | 26.94 | 0.01 | 1.14 |
| Fallers | 13 | 26.14 | 0.95 | 24.06 | 28.22 | 21.07 | 31.29 | |||
| Swing (%) | Non-Fallers | 13 | 38.68 | 0.35 | 37.91 | 39.44 | 36.58 | 40.76 | 0.01 | 1.13 |
| Fallers | 13 | 37.03 | 0.45 | 36.05 | 38.02 | 34.47 | 39.46 | |||
| Pitch at Initial Contact (°) | Non-Fallers | 13 | 22.09 | 1.09 | 19.73 | 24.46 | 26.51 | 12.46 | 0.02 a | 0.92 |
| Fallers | 13 | 17.30 | 1.74 | 13.52 | 21.08 | 24.41 | 5.38 | |||
| Turn Angle (°) | Non-Fallers | 12 | 88.79 | 1.40 | 85.71 | 91.87 | 79.03 | 95.58 | 0.04 | 0.87 |
| Fallers | 13 | 82.55 | 2.43 | 77.25 | 87.86 | 63.36 | 97.65 | |||
| Test Result Variable (s) | Area | Std. Error a | Asymptotic Sig. b | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Pitch at Toe Off (°) | 0.85 | 0.080 | 0.003 | 0.690 | 1.000 |
| Gait Speed (m/s) | 0.78 | 0.096 | 0.017 | 0.595 | 0.969 |
| Stride Length (m) | 0.78 | 0.100 | 0.019 | 0.579 | 0.972 |
| Double Support (%) | 0.78 | 0.095 | 0.017 | 0.589 | 0.962 |
| Swing (%) | 0.78 | 0.094 | 0.017 | 0.598 | 0.966 |
| Pitch at Initial Contact (°) | 0.77 | 0.093 | 0.020 | 0.587 | 0.951 |
| Turn Angle (°) | 0.75 | 0.104 | 0.034 | 0.546 | 0.954 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arpan, I.; Shah, V.V.; McNames, J.; Harker, G.; Carlson-Kuhta, P.; Spain, R.; El-Gohary, M.; Mancini, M.; Horak, F.B. Fall Prediction Based on Instrumented Measures of Gait and Turning in Daily Life in People with Multiple Sclerosis. Sensors 2022, 22, 5940. https://doi.org/10.3390/s22165940
Arpan I, Shah VV, McNames J, Harker G, Carlson-Kuhta P, Spain R, El-Gohary M, Mancini M, Horak FB. Fall Prediction Based on Instrumented Measures of Gait and Turning in Daily Life in People with Multiple Sclerosis. Sensors. 2022; 22(16):5940. https://doi.org/10.3390/s22165940
Chicago/Turabian StyleArpan, Ishu, Vrutangkumar V. Shah, James McNames, Graham Harker, Patricia Carlson-Kuhta, Rebecca Spain, Mahmoud El-Gohary, Martina Mancini, and Fay B. Horak. 2022. "Fall Prediction Based on Instrumented Measures of Gait and Turning in Daily Life in People with Multiple Sclerosis" Sensors 22, no. 16: 5940. https://doi.org/10.3390/s22165940