
Validation of Visually Identified Muscle Potentials during Human Sleep Using High Frequency/Low Frequency Spectral Power Ratios

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
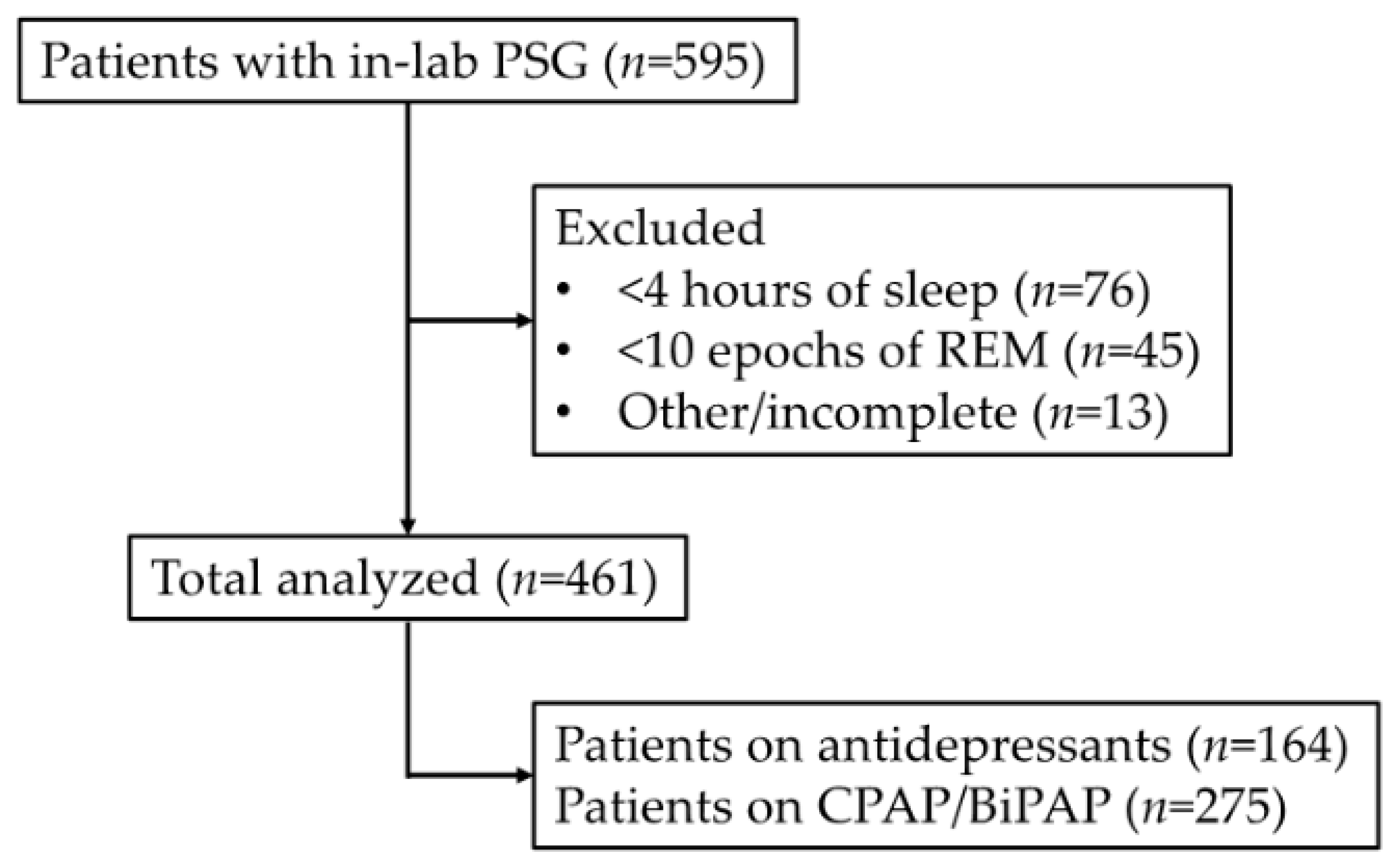
2.1. Participants and Polysomnography Recording
2.2. HF:LF Analysis
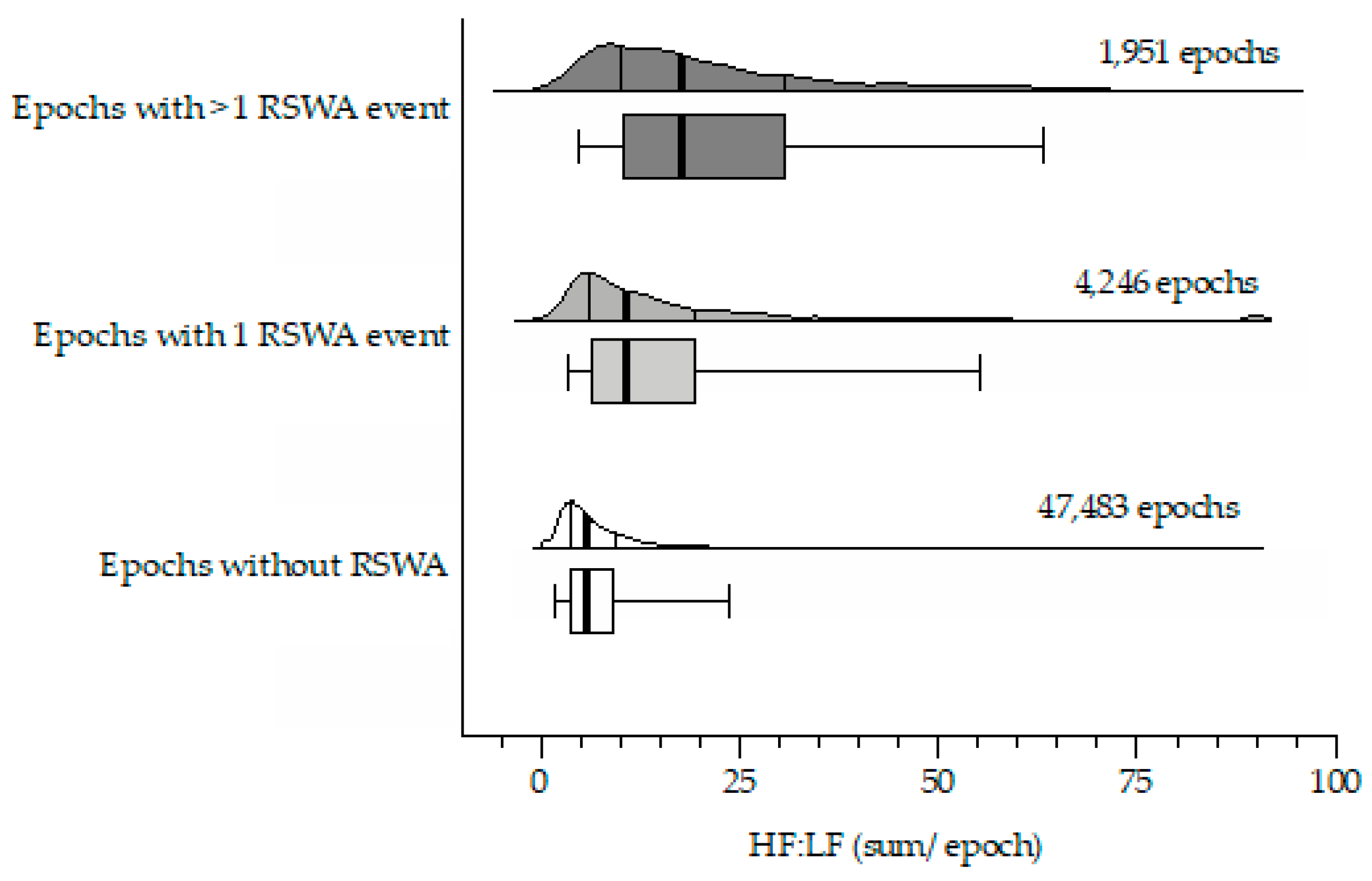
2.3. Epoch-Based HF:LF Analysis: Grouping Based on the Number of REM Sleep without Atonia Episodes per REM Epoch
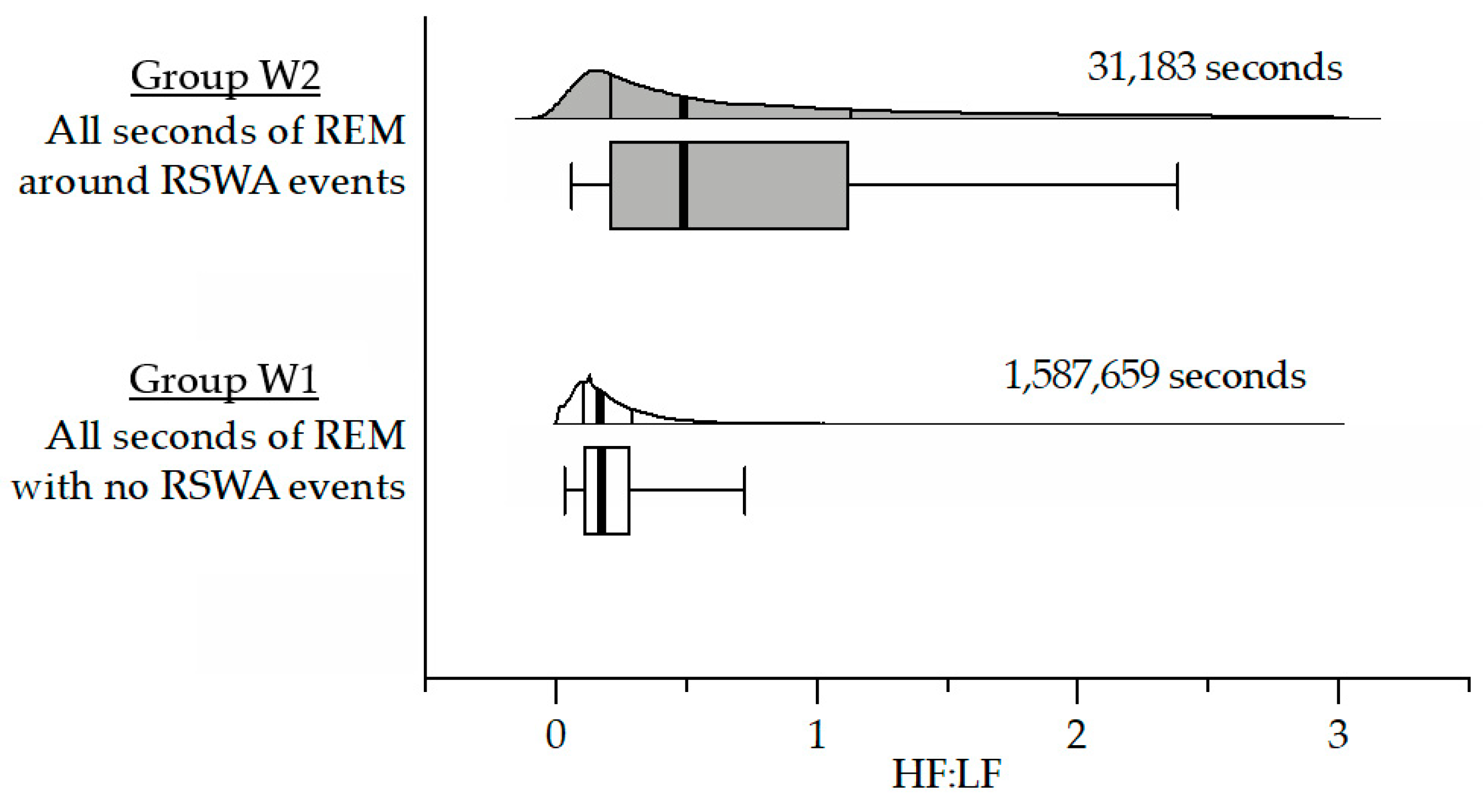
2.4. Window-Based HF:LF Analysis: Compare All EMG-Index Values for Every Second
3. Results
3.1. Datasets
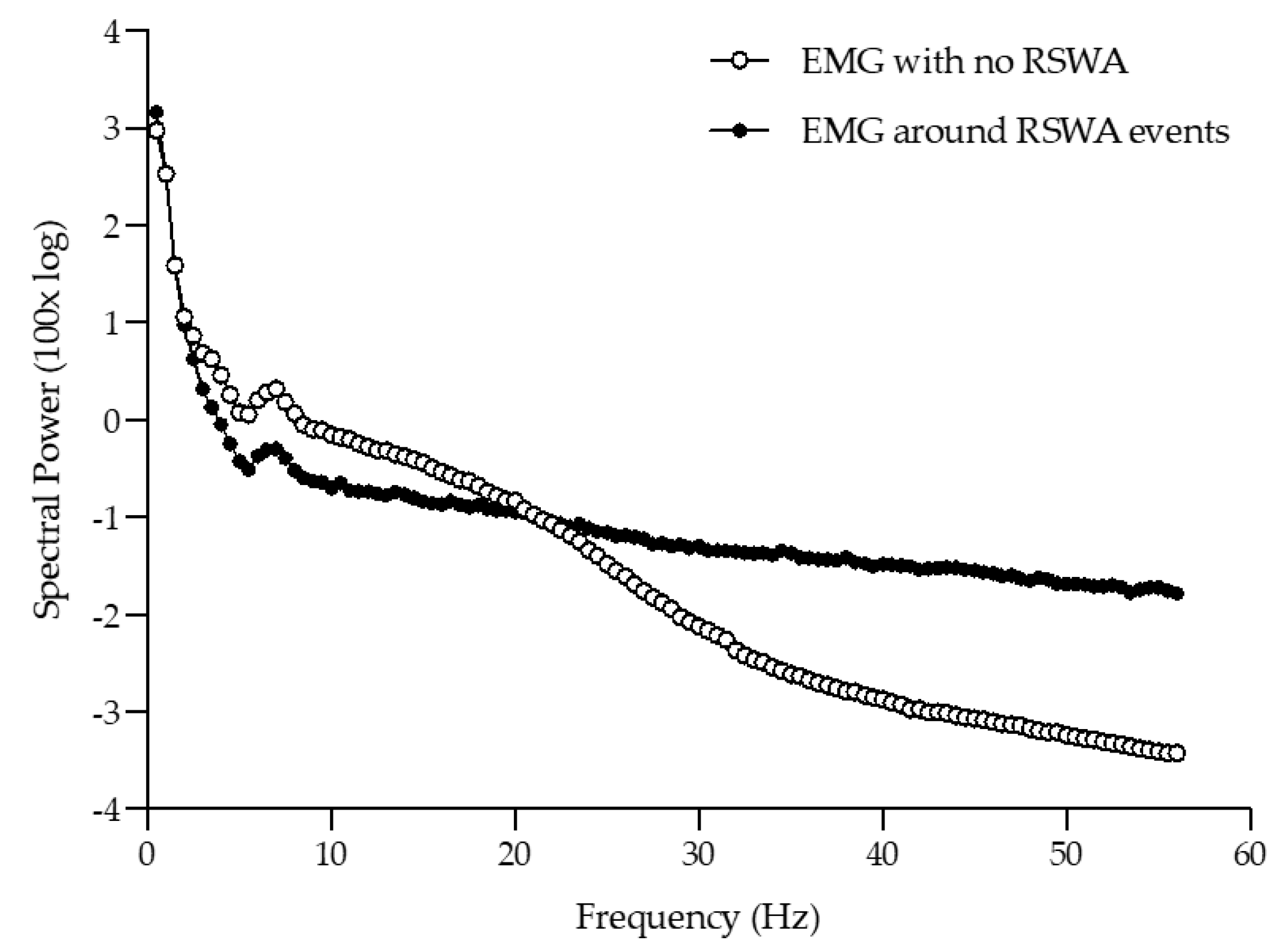
3.2. EMG Relative Spectral Power
3.3. Epoch-Based HF:LF Analysis
3.4. Window-Based HF:LF Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berry, R.B.; Brooks, R.; Gamaldo, C.E.; Harding, S.M.; Marcus, C.L.; Vaughn, B.V.; Tangredi, M.M. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications; Version 2.0.; American Academy of Sleep Medicine: Darien, IL, USA, 2012. [Google Scholar]
- Dement, W. The occurence of low voltage, fast, electroencephalogram patterns during behavioral sleep in the cat. Electroencephalogr. Clin. Neurophysiol. 1958, 10, 291–296. [Google Scholar] [CrossRef]
- Jouvet, M.; Michel, M.; Courjon, J. Sur la mise en jeu de deux mechanismes a l’expression electro-encephalographique differente au cours du sommeil physiologique chez le Chat. Comptes Rendus Seances L’Academie Sci. 1959, 248, 3043–3045. [Google Scholar]
- Bliwise, D.; Coleman, R.; Bergmann, B.; Wincor, M.Z.; Pivii, R.T.; Rechtschaffen, A. Facial Muscle Tonus During REM and NREM Sleep. Psychophysiology 1974, 11, 497–508. [Google Scholar] [CrossRef]
- Schenck, C.H.; Bundlie, S.R.; Ettinger, M.G.; Mahowald, M.W. Chronic Behavioral Disorders of Human REM Sleep: A New Category of Parasomnia. Sleep 1986, 9, 293–308. [Google Scholar] [CrossRef] [Green Version]
- Boeve, B.; Silber, M.; Ferman, T.; Lin, S.; Benarroch, E.; Schmeichel, A.; Ahlskog, J.; Caselli, R.; Jacobson, S.; Sabbagh, M.; et al. Clinicopathologic correlations in 172 cases of rapid eye movement sleep behavior disorder with or without a coexisting neurologic disorder. Sleep Med. 2013, 14, 754–762. [Google Scholar] [CrossRef] [Green Version]
- Plazzi, G.; Corsini, R.; Provini, F.; Pierangeli, G.; Martinelli, P.; Montagna, P.; Lugaresi, E.; Cortelli, P. REM sleep behavior disorders in multiple system atrophy. Neurology 1997, 48, 1094–1096. [Google Scholar] [CrossRef] [PubMed]
- Marion, M.-H.; Qurashi, M.; Marshall, G.; Foster, O. Is REM sleep Behaviour Disorder (RBD) a risk factor of dementia in idiopathic Parkinson’s disease? J. Neurol. 2008, 255, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, J.-F.; Postuma, R.B.; Mazza, S.; Doyon, J.; Montplaisir, J. Rapid-eye-movement sleep behaviour disorder and neurodegenerative diseases. Lancet Neurol. 2006, 5, 424–432. [Google Scholar] [CrossRef]
- Galbiati, A.; Verga, L.; Giora, E.; Zucconi, M.; Ferini-Strambi, L. The risk of neurodegeneration in REM sleep behavior disorder: A systematic review and meta-analysis of longitudinal studies. Sleep Med. Rev. 2019, 43, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Barone, D.A.; Henchcliffe, C. Rapid eye movement sleep behavior disorder and the link to alpha-synucleinopathies. Clin. Neurophysiol. 2018, 129, 1551–1564. [Google Scholar] [CrossRef]
- Iranzo, A.; Stockner, H.; Serradell, M.; Seppi, K.; Valldeoriola, F.; Frauscher, B.; Molinuevo, J.L.; Vilaseca, I.; Mitterling, T.; Gaig, C.; et al. Five-year follow-up of substantia nigra echogenicity in idiopathic REM sleep behavior disorder. Mov. Disord. 2014, 29, 1774–1780. [Google Scholar] [CrossRef] [PubMed]
- Schenck, C.H.; Boeve, B.F.; Mahowald, M.W. Delayed emergence of a parkinsonian disorder or dementia in 81% of older men initially diagnosed with idiopathic rapid eye movement sleep behavior disorder: A 16-year update on a previously reported series. Sleep Med. 2013, 14, 744–748. [Google Scholar] [CrossRef]
- Berg, D.; Postuma, R.B.; Adler, C.H.; Bloem, B.R.; Chan, P.; Dubois, B.; Gasser, T.; Goetz, C.G.; Halliday, G.; Joseph, L.; et al. MDS research criteria for prodromal Parkinson’s disease. Mov. Disord. 2015, 30, 1600–1611. [Google Scholar] [CrossRef] [PubMed]
- Lapierre, O.; Montplaisir, J. Polysomnographic features of REM sleep behavior disorder: Development of a scoring method. Neurology 1992, 42, 1371. [Google Scholar] [CrossRef]
- Bliwise, D.L.; He, L.; Pour Ansari, F.; Rye, D.B. Quantification of Electromyographic Activity During Sleep: A Phasic Electromyographic Metric. J. Clin. Neurophysiol. 2006, 23, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Fairley, J.A.; Georgoulas, G.; Mehta, N.A.; Gray, A.G.; Bliwise, D.L. Computer detection approaches for the identification of phasic electromyographic (EMG) activity during human sleep. Biomed. Signal Process. Control. 2012, 7, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Lai, D.; Bin Heyat, B.; Khan, F.I.; Zhang, Y. Prognosis of Sleep Bruxism Using Power Spectral Density Approach Applied on EEG Signal of Both EMG1-EMG2 and ECG1-ECG2 Channels. IEEE Access 2019, 7, 82553–82562. [Google Scholar] [CrossRef]
- Bin Heyat, B.; Akhtar, F.; Khan, M.H.; Ullah, N.; Gul, I.; Khan, H.; Lai, D. Detection, Treatment Planning, and Genetic Predisposition of Bruxism: A Systematic Mapping Process and Network Visualization Technique. CNS Neurol. Disord. Drug Targets 2021, 20, 755–775. [Google Scholar] [CrossRef]
- Ferri, R.; Fulda, S.; Cosentino, F.I.; Pizza, F.; Plazzi, G. A preliminary quantitative analysis of REM sleep chin EMG in Parkinson’s disease with or without REM sleep behavior disorder. Sleep Med. 2012, 13, 707–713. [Google Scholar] [CrossRef]
- Figorilli, M.; Ferri, R.; Zibetti, M.; Beudin, P.; Puligheddu, M.; Lopiano, L.; Cicolin, A.; Durif, F.; Marques, A.; Fantini, M.L. Comparison Between Automatic and Visual Scorings of REM Sleep Without Atonia for the Diagnosis of REM Sleep Behavior Disorder in Parkinson Disease. Sleep 2017, 40, 13–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yildiz, S.; Opel, R.A.; Elliott, J.E.; Kaye, J.; Cao, H.; Lim, M.M. Categorizing Sleep in Older Adults with Wireless Activity Monitors Using LSTM Neural Networks. In Proceedings of the EMBC 2019, Berlin, Germany, 23–27 July 2019; pp. 3368–3372. [Google Scholar] [CrossRef]
- Bin Heyat, B.; Lai, D.; Khan, F.I.; Zhang, Y. Sleep Bruxism Detection Using Decision Tree Method by the Combination of C4-P4 and C4-A1 Channels of Scalp EEG. IEEE Access 2019, 7, 102542–102553. [Google Scholar] [CrossRef]
- Ali, L.; He, Z.; Cao, W.; Rauf, H.T.; Imrana, Y.; Bin Heyat, B. MMDD-Ensemble: A Multimodal Data–Driven Ensemble Approach for Parkinson’s Disease Detection. Front. Neurosci. 2021, 15. [Google Scholar] [CrossRef] [PubMed]
- Bin Heyat, B.; Akhtar, F.; Ansari, M.; Khan, A.; Alkahtani, F.; Khan, H.; Lai, D. Progress in Detection of Insomnia Sleep Disorder: A Comprehensive Review. Curr. Drug Targets 2021, 22, 672–684. [Google Scholar] [CrossRef] [PubMed]
- Heyat, B.; Akhtar, F.; Khan, A.; Noor, A.; Benjdira, B.; Qamar, Y.; Abbas, S.; Lai, D. A Novel Hybrid Machine Learning Classification for the Detection of Bruxism Patients Using Physiological Signals. Appl. Sci. 2020, 10, 7410. [Google Scholar] [CrossRef]
- Fernández-Arcos, A.; Serradell, M.; Guaita, M.; Santamaria, J.; Iranzo, A.; Gaig, C.; Salamero, M. Diagnostic Value of Isolated Mentalis Versus Mentalis Plus Upper Limb Electromyography in Idiopathic REM Sleep Behavior Disorder Patients Eventually Developing a Neurodegenerative Syndrome. Sleep 2017, 40, zsx025. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Christensen, J.A.; Sixel-Döring, F.; Trenkwalder, C.; Mayer, G.; Oertel, W.H.; Jennum, P.; Sorensen, H. Validation of a new data-driven automated algorithm for muscular activity detection in REM sleep behavior disorder. J. Neurosci. Methods 2019, 312, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Seven, Y.B.; Mantilla, C.; Zhan, W.-Z.; Sieck, G.C. Non-stationarity and power spectral shifts in EMG activity reflect motor unit recruitment in rat diaphragm muscle. Respir. Physiol. Neurobiol. 2013, 185, 400–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shokrollahi, M.; Krishnan, S. A Review of Sleep Disorder Diagnosis by Electromyogram Signal Analysis. Crit. Rev. Biomed. Eng. 2015, 43, 1–20. [Google Scholar] [CrossRef]
- Elliott, J.E.; Opel, R.A.; Pleshakov, D.; Rachakonda, T.; Chau, A.Q.; Weymann, K.B.; Lim, M.M. Posttraumatic stress disorder increases the odds of REM sleep behavior disorder and other parasomnias in Veterans with and without comorbid traumatic brain injury. Sleep 2020, 43, zsz237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, J.E.; Opel, R.A.; Weymann, K.B.; Chau, A.Q.; Papesh, M.A.; Callahan, M.L.; Storzbach, D.; Lim, M.M. Sleep Disturbances in Traumatic Brain Injury: Associations with Sensory Sensitivity. J. Clin. Sleep Med. 2018, 14, 1177–1186. [Google Scholar] [CrossRef] [Green Version]
- Balba, N.M.; Elliott, J.E.; Weymann, K.B.; Opel, R.A.; Duke, J.W.; Oken, B.S.; Morasco, B.J.; Heinricher, M.M.; Lim, M.M. Increased sleep disturbances and pain in Veterans with co-morbid TBI and PTSD. J. Clin. Sleep Med. 2018, 14, 1865–1878. [Google Scholar] [CrossRef] [Green Version]
- Sandsmark, D.K.; Elliott, J.; Lim, M.M. Sleep-Wake Disturbances after Traumatic Brain Injury: Synthesis of Human and Animal Studies. Sleep 2017, 40, 44. [Google Scholar] [CrossRef] [Green Version]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Arnulf, I.; Hogl, B.; Iranzo, A.; Miyamoto, T.; Jennum, P.; Pelletier, A.; Wolfson, C.; Leu-Semenescu, S.; Frauscher, B.; et al. A Single-Question Screen for REM Sleep Behavior Disorder: A Multicenter Validation Study. Mov. Disord. 2012, 27, 913–916. [Google Scholar] [CrossRef]
- Cesari, M.; Heidbreder, A.; Louis, E.K.S.; Sixel-Döring, F.; Bliwise, D.L.; Baldelli, L.; Bes, F.; Fantini, M.L.; Iranzo, A.; Knudsen-Heier, S.; et al. Video-polysomnography procedures for diagnosis of rapid eye movement sleep behavior disorder (RBD) and the identification of its prodromal stages: Guidelines from the International RBD Study Group. Sleep 2021. [Google Scholar] [CrossRef]
- Ferri, R.; Rundo, F.; Manconi, M.; Plazzi, G.; Bruni, O.; Oldani, A.; Strambi, L.F.; Zucconi, M. Improved computation of the atonia index in normal controls and patients with REM sleep behavior disorder. Sleep Med. 2010, 11, 947–949. [Google Scholar] [CrossRef]
- Frauscher, B.; Gabelia, D.; Biermayr, M.; Stefani, A.; Hackner, H.; Mitterling, T.; Poewe, W.; Högl, B. Validation of an Integrated Software for the Detection of Rapid Eye Movement Sleep Behavior Disorder. Sleep 2014, 37, 1663–1671. [Google Scholar] [CrossRef] [Green Version]
- Guttowski, D.; Mayer, G.; Oertel, W.; Kesper, K.; Rosenberg, T. Validation of semiautomatic scoring of REM sleep without atonia in patients with RBD. Sleep Med. 2018, 46, 107–113. [Google Scholar] [CrossRef]
- Mayer, G.; Kesper, K.; Ploch, T.; Canisius, S.; Penzel, T.; Oertel, W.; Stiasny-Kolster, K. Quantification of Tonic and Phasic Muscle Activity in REM Sleep Behavior Disorder. J. Clin. Neurophysiol. 2008, 25, 48–55. [Google Scholar] [CrossRef]
- Cooray, N.; Andreotti, F.; Lo, C.; Symmonds, M.; Hu, M.; De Vos, M. Detection of REM sleep behaviour disorder by automated polysomnography analysis. Clin. Neurophysiol. 2019, 130, 505–514. [Google Scholar] [CrossRef]
- Frandsen, R.; Nikolic, M.; Zoetmulder, M.; Kempfner, L.; Jennum, P. Analysis of automated quantification of motor activity in REM sleep behaviour disorder. J. Sleep Res. 2015, 24, 583–590. [Google Scholar] [CrossRef]
- Winkelman, J.W.; James, L. Serotonergic Antidepressants are Associated with REM Sleep without Atonia. Sleep 2004, 27, 317–321. [Google Scholar] [CrossRef] [Green Version]
- Frauscher, B.; Jennum, P.; Ju, Y.-E.; Postuma, R.B.; Arnulf, I.; De Cock, V.C.; Dauvilliers, Y.; Fantini, M.L.; Strambi, L.F.; Gabelia, D.; et al. Comorbidity and medication in REM sleep behavior disorder: A multicenter case-control study. Neurology 2014, 82, 1076–1079. [Google Scholar] [CrossRef] [Green Version]
- Iranzo, A.; Frauscher, B.; Santos, H.; Gschliesser, V.; Ratti, L.; Falkenstetter, T.; Stürner, C.; Salamero, M.; Tolosa, E.; Poewe, W. Usefulness of the SINBAR electromyographic montage to detect the motor and vocal manifestations occurring in REM sleep behavior disorder. Sleep Med. 2011, 12, 284–288. [Google Scholar] [CrossRef]
- Bliwise, P.D.L.; Fairley, P.J.; Hoff, M.S.; Rosenberg, P.R.S.; Rye, M.D.B.; Schulman, D.; Trotti, M.L.M. Inter-rater agreement for visual discrimination of phasic and tonic electromyographic activity in sleep. Sleep 2018, 41, 41. [Google Scholar] [CrossRef] [PubMed]
- Brooks, P.L.; Peever, J. A Temporally Controlled Inhibitory Drive Coordinates Twitch Movements during REM Sleep. Curr. Biol. 2016, 26, 1177–1182. [Google Scholar] [CrossRef] [Green Version]
- Brooks, P.L.; Peever, J.H. Glycinergic and GABAA-Mediated Inhibition of Somatic Motoneurons Does Not Mediate Rapid Eye Movement Sleep Motor Atonia. J. Neurosci. 2008, 28, 3535–3545. [Google Scholar] [CrossRef]
- Iranzo, A. The REM sleep circuit and how its impairment leads to REM sleep behavior disorder. Cell Tissue Res. 2018, 373, 245–266. [Google Scholar] [CrossRef]
- McCarter, S.J.; Sandness, D.J.; McCarter, A.R.; Feemster, J.C.; Teigen, L.N.; Timm, P.C.; Boeve, B.F.; Silber, M.H.; Louis, E.K.S. REM sleep muscle activity in idiopathic REM sleep behavior disorder predicts phenoconversion. Neurology 2019, 93, e1171–e1179. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Whole Group | |
|---|---|
| n = 461 | |
| Age, years | 53.9 ± 15.9 |
| Sex, male | 92.0% |
| Height, cm | 177.2 ± 7.8 |
| Weight, kg | 102.3 ± 21.1 |
| BMI, kg/m2 | 32.6 ± 6.6 |
| Race, white | 83.9% |
| Ethnicity, not Hispanic or Latino | 90.2% |
| Education, at least some college | 79.0% |
| Marital status, married/partnered | 62.5% |
| Living situation, spouse/partner | 63.8% |
| Exercise, >90 min/week | 28.0% |
| TBI, yes | 20.8% |
| PTSD, yes | 30.6% |
| RBD1Q dream enactment, yes | 43.4% |
| RLS, yes | 44.3% |
| Snore, yes | 88.3% |
| CPAP/BiPAP, yes | 59.7% |
| Antidepressant use, yes | 35.6% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Modarres, M.H.; Elliott, J.E.; Weymann, K.B.; Pleshakov, D.; Bliwise, D.L.; Lim, M.M. Validation of Visually Identified Muscle Potentials during Human Sleep Using High Frequency/Low Frequency Spectral Power Ratios. Sensors 2022, 22, 55. https://doi.org/10.3390/s22010055
Modarres MH, Elliott JE, Weymann KB, Pleshakov D, Bliwise DL, Lim MM. Validation of Visually Identified Muscle Potentials during Human Sleep Using High Frequency/Low Frequency Spectral Power Ratios. Sensors. 2022; 22(1):55. https://doi.org/10.3390/s22010055
Chicago/Turabian StyleModarres, Mo H., Jonathan E. Elliott, Kristianna B. Weymann, Dennis Pleshakov, Donald L. Bliwise, and Miranda M. Lim. 2022. "Validation of Visually Identified Muscle Potentials during Human Sleep Using High Frequency/Low Frequency Spectral Power Ratios" Sensors 22, no. 1: 55. https://doi.org/10.3390/s22010055