
Pelvis-Toe Distance: 3-Dimensional Gait Characteristics of Functional Limb Shortening in Hemiparetic Stroke

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure and Data Collection
2.3. Kinematic Outcome Measures
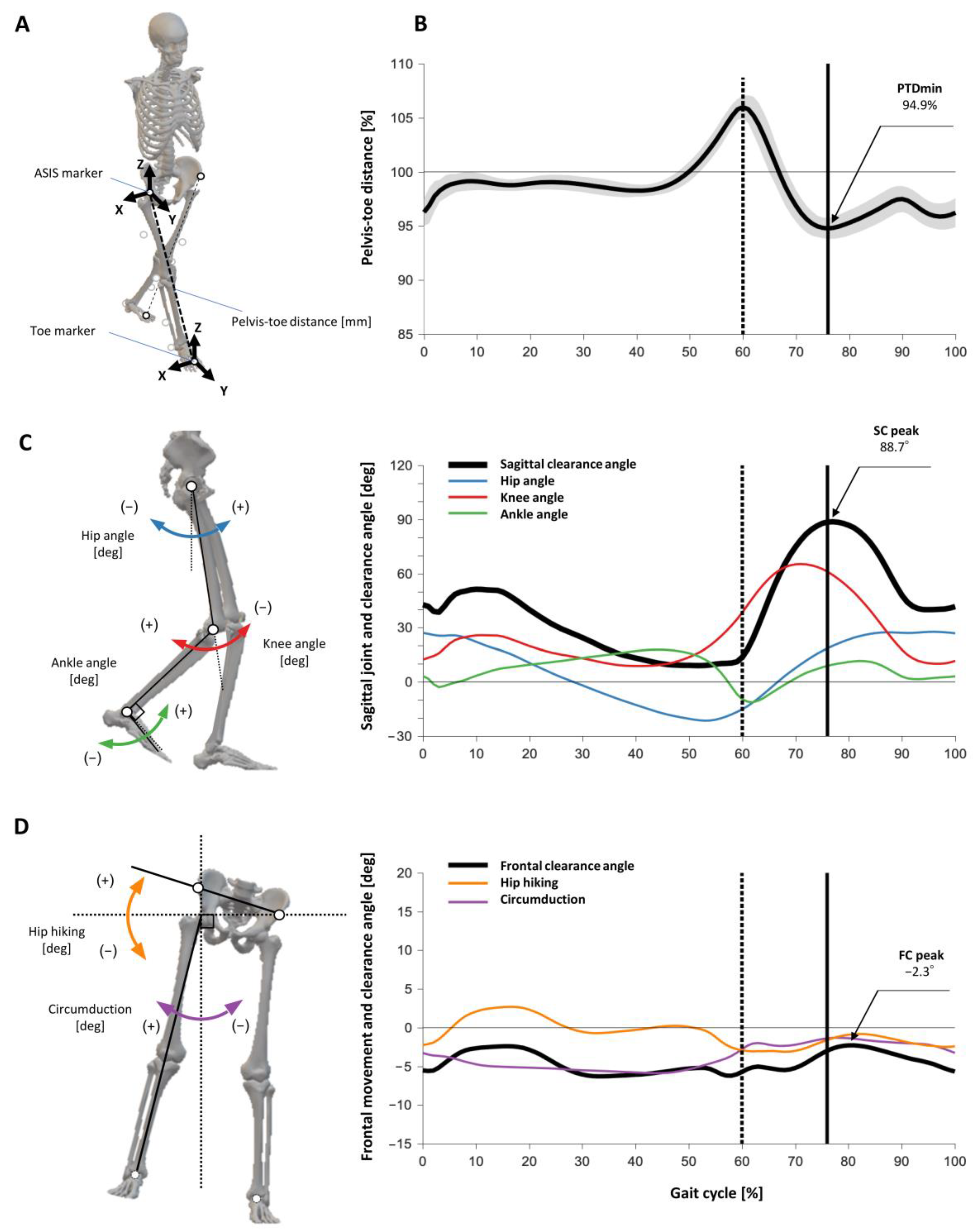
2.3.1. PTD and PTDmin
2.3.2. Index for the SC Angle
2.3.3. Index for the FC Angle
2.4. Clinical Outcome Measures
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASIS | anterior superior iliac spine |
| CI | confidence interval |
| FC | frontal clearance |
| FMA-LE | Fugl-Meyer Assessment Lower Extremity Subscale |
| GAIT | Gait Assessment and Intervention Tool |
| MAS | modified Ashworth scale |
| PTD | pelvis-toe distance |
| PTDmin | minimum %pelvis-toe distance |
| SC | sagittal clearance |
| SSWS | self-selected walking speed |
References
- Knutsson, E.; Richards, C.L. Different Types of Disturbed Motor Control in Gait of Hemiparetic Patients. Brain 1979, 102, 405–430. [Google Scholar] [CrossRef]
- Moore, S.; Schurr, K.; Wales, A.; Moseley, A.; Herbert, R. Observation and analysis of hemiplegic gait: Swing phase. Aust. J. Physiother. 1993, 39, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.; Patten, C.; Kothari, D.H.; Zajac, F.E. Gait differences between individuals with post-stroke hemiparesis and non-disabled controls at matched speeds. Gait Posture 2005, 22, 51–56. [Google Scholar] [CrossRef]
- Stanhope, V.A.; Knarr, B.A.; Reisman, D.S.; Higginson, J.S. Frontal plane compensatory strategies associated with self-selected walking speed in individuals post-stroke. Clin. Biomech. 2014, 29, 518–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.; Eng, J.J. Magnitude and pattern of 3D kinematic and kinetic gait profiles in persons with stroke: Relationship to walking speed. Gait Posture 2004, 20, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Kerrigan, D.C.; Frates, E.P.; Rogan, S.; Riley, P.O. Hip Hiking and circumduction: Quantitative definitions. Am. J. Phys. Med. Rehabilitation 2000, 79, 247–252. [Google Scholar] [CrossRef]
- Reisman, D.S.; Kesar, T.M.; Perumal, R.; Roos, M.A.; Rudolph, K.S.; Higginson, J.; Helm, E.; Binder-Macleod, S. Time Course of Functional and Biomechanical Improvements during a Gait Training Intervention in Persons with Chronic Stroke. J. Neurol. Phys. Ther. 2013, 37, 159–165. [Google Scholar] [CrossRef]
- Huitema, R.B.; Hof, A.L.; Mulder, T.; Brouwer, W.H.; Dekker, R.; Postema, K. Functional recovery of gait and joint kinematics after right hemispheric stroke. Arch. Phys. Med. Rehabil. 2004, 85, 1982–1988. [Google Scholar] [CrossRef] [Green Version]
- Wonsetler, E.; Bowden, M.G. A systematic review of mechanisms of gait speed change post-stroke. Part 2: Exercise capacity, muscle activation, kinetics, and kinematics. Top. Stroke Rehabil. 2017, 24, 394–403. [Google Scholar] [CrossRef]
- Levin, M.F.; Kleim, J.A.; Wolf, S.L. What Do Motor “Recovery” and “Compensation” Mean in Patients Following Stroke? Neurorehabilit. Neural Repair 2009, 23, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Yavuzer, G.; Oken, O.; Elhan, A.; Stam, H.J. Repeatability of lower limb three-dimensional kinematics in patients with stroke. Gait Posture 2008, 27, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Kwakkel, G.; Lannin, N.; Borschmann, K.; English, C.; Ali, M.; Churilov, L.; Saposnik, G.; Winstein, C.; van Wegen, E.; Wolf, S.L.; et al. Standardized Measurement of Sensorimotor Recovery in Stroke Trials: Consensus-Based Core Recommendations from the Stroke Recovery and Rehabilitation Roundtable. Neurorehabilit. Neural Repair 2017, 31, 784–792. [Google Scholar] [CrossRef] [Green Version]
- Mulroy, S.; Gronley, J.; Weiss, W.; Newsam, C.; Perry, J. Use of cluster analysis for gait pattern classification of patients in the early and late recovery phases following stroke. Gait Posture 2003, 18, 114–125. [Google Scholar] [CrossRef]
- Mena, D.; Mansour, J.; Simon, S. Analysis and synthesis of human swing leg motion during gait and its clinical applications. J. Biomech. 1981, 14, 823–832. [Google Scholar] [CrossRef]
- Cruz, T.H.; Lewek, M.; Dhaher, Y.Y. Biomechanical impairments and gait adaptations post-stroke: Multi-factorial associations. J. Biomech. 2009, 42, 1673–1677. [Google Scholar] [CrossRef] [Green Version]
- Kuo, A.D. The six determinants of gait and the inverted pendulum analogy: A dynamic walking perspective. Hum. Mov. Sci. 2007, 26, 617–656. [Google Scholar] [CrossRef]
- Bazargan-Lari, Y.; Eghtesad, M.; Khoogar, A.; Mohammad-Zadeh, A. Dynamics and Regulation of Locomotion of a Human Swing Leg as a Double-Pendulum Considering Self-Impact Joint Constraint. J. Biomed. Phys. Eng. 2014, 4, 91–102. [Google Scholar] [PubMed]
- Murray, P.M.; Clarkson, B.H. The Vertical Pathways of the Foot During Level Walking. II. Clinical Examples of Distorted Pathways. Phys. Ther. 1966, 46, 590–599. [Google Scholar] [CrossRef]
- Moosabhoy, M.A.; Gard, S.A. Methodology for determining the sensitivity of swing leg toe clearance and leg length to swing leg joint angles during gait. Gait Posture 2006, 24, 493–501. [Google Scholar] [CrossRef]
- Little, V.L.; McGuirk, T.E.; Patten, C. Impaired Limb Shortening following Stroke: What’s in a Name? PLoS ONE 2014, 9, e110140. [Google Scholar] [CrossRef]
- Tyrell, C.M.; Roos, M.A.; Rudolph, K.S.; Reisman, D.S. Influence of Systematic Increases in Treadmill Walking Speed on Gait Kinematics After Stroke. Phys. Ther. 2011, 91, 392–403. [Google Scholar] [CrossRef] [Green Version]
- Turnbull, G.I.; Charteris, J.; Wall, J.C. A comparison of the range of walking speeds between normal and hemiplegic subjects. Scand. J. Rehabil. Med. 1995, 27, 175–182. [Google Scholar]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. A method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar]
- See, J.; Dodakian, L.; Chou, C.; Chan, V.; McKenzie, A.; Reinkensmeyer, D.J.; Cramer, S.C. A Standardized Approach to the Fugl-Meyer Assessment and Its Implications for Clinical Trials. Neurorehabilit. Neural Repair 2013, 27, 732–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W.; Smith, M.B. Interrater Reliability of a Modified Ashworth Scale of Muscle Spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef] [PubMed]
- Daly, J.; Nethery, J.; McCabe, J.; Brenner, I.; Rogers, J.; Gansen, J.; Butler, K.; Burdsall, R.; Roenigk, K.; Holcomb, J. Development and testing of the Gait Assessment and Intervention Tool (G.A.I.T.): A measure of coordinated gait components. J. Neurosci. Methods 2009, 178, 334–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winter, D.A. Foot Trajectory in Human Gait: A Precise and Multifactorial Motor Control Task. Phys. Ther. 1992, 72, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Olney, S.J.; Richards, C.L. Hemiparetic gait following stroke. Part I: Characteristics. Gait Posture 1996, 4, 136–148. [Google Scholar] [CrossRef]
- Matsuda, F.; Mukaino, M.; Ohtsuka, K.; Tanikawa, H.; Tsuchiyama, K.; Teranishi, T.; Kanada, Y.; Kagaya, H.; Saitoh, E. Biomechanical factors behind toe clearance during the swing phase in hemiparetic patients. Top. Stroke Rehabil. 2017, 24, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Roche, N.; Bonnyaud, C.; Geiger, M.; Bussel, B.; Bensmail, D. Relationship between hip flexion and ankle dorsiflexion during swing phase in chronic stroke patients. Clin. Biomech. 2015, 30, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Pohl, J.; Held, J.P.O.; Verheyden, G.; Murphy, M.A.; Engelter, S.; Flöel, A.; Keller, T.; Kwakkel, G.; Nef, T.; Walker, M.; et al. Consensus-Based Core Set of Outcome Measures for Clinical Motor Rehabilitation After Stroke—A Delphi Study. Front. Neurol. 2020, 11. [Google Scholar] [CrossRef]
- Figueiredo, J.; Moreno, J.C.; Matias, A.C.; Pereira, F.; Santos, C.P. Outcome measures and motion capture systems for assessing lower limb orthosis-based interventions after stroke: A systematic review. Disabil. Rehabil. Assist. Technol. 2021, 16, 674–683. [Google Scholar] [CrossRef]
- Shin, S.Y.; Lee, R.K.; Spicer, P.; Sulzer, J. Does kinematic gait quality improve with functional gait recovery? A longitudinal pilot study on early post-stroke individuals. J. Biomech. 2020, 105, 109761. [Google Scholar] [CrossRef] [PubMed]
- Roelker, S.A.; Bowden, M.G.; Kautz, S.A.; Neptune, R.R. Paretic propulsion as a measure of walking performance and functional motor recovery post-stroke: A review. Gait Posture 2019, 68, 6–14. [Google Scholar] [CrossRef]
- Awad, L.N.; Lewek, M.D.; Kesar, T.M.; Franz, J.R.; Bowden, M.G. These legs were made for propulsion: Advancing the diagnosis and treatment of post-stroke propulsion deficits. J. Neuroeng. Rehabil. 2020, 17, 139. [Google Scholar] [CrossRef]
- Ogihara, H.; Tsushima, E.; Kamo, T.; Sato, T.; Matsushima, A.; Niioka, Y.; Asahi, R.; Azami, M. Kinematic gait asymmetry assessment using joint angle data in patients with chronic stroke—A normalized cross-correlation approach. Gait Posture 2020, 80, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Chow, J.W.; Stokic, D.S. Intersegmental coordination of gait after hemorrhagic stroke. Exp. Brain Res. 2015, 233, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Sakuma, K.; Tateuchi, H.; Nishishita, S.; Okita, Y.; Kitatani, R.; Koyama, Y.; Ibuki, S.; Ichihashi, N. Gait kinematics and physical function that most affect intralimb coordination in patients with stroke. NeuroRehabilitation 2019, 45, 493–499. [Google Scholar] [CrossRef]
- Guzik, A.; Drużbicki, M.; Maistrello, L.; Turolla, A.; Agostini, M.; Kiper, P. Relationship Between Observational Wisconsin Gait Scale, Gait Deviation Index, and Gait Variability Index in Individuals Poststroke. Arch. Phys. Med. Rehabil. 2019, 100, 1680–1687. [Google Scholar] [CrossRef]
- Guzik, A.; Drużbicki, M. Application of the Gait Deviation Index in the analysis of post-stroke hemiparetic gait. J. Biomech. 2020, 99, 109575. [Google Scholar] [CrossRef]
- Gouelle, A.; Megrot, F.; Presedo, A.; Husson, I.; Yelnik, A.; Penneçot, G.-F. The Gait Variability Index: A new way to quantify fluctuation magnitude of spatiotemporal parameters during gait. Gait Posture 2013, 38, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.E.; Crowner, B.E.; Kluding, P.M.; Nichols, D.; Rose, D.K.; Yoshida, R.; Zipp, G.P. Outcome Measures for Individuals With Stroke: Process and Recommendations From the American Physical Therapy Association Neurology Section Task Force. Phys. Ther. 2013, 93, 1383–1396. [Google Scholar] [CrossRef]
- Pongpipatpaiboon, K.; Mukaino, M.; Matsuda, F.; Ohtsuka, K.; Tanikawa, H.; Yamada, J.; Tsuchiyama, K.; Saitoh, E. The impact of ankle-foot orthoses on toe clearance strategy in hemiparetic gait: A cross-sectional study. J. Neuroeng. Rehabil. 2018, 15, 41. [Google Scholar] [CrossRef]
- Khamis, S.; Springer, S.; Ovadia, D.; Krimus, S.; Carmeli, E. Measuring Dynamic Leg Length during Normal Gait. Sensors 2018, 18, 4191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rinaldi, L.A.; Monaco, V. Spatio-temporal parameters and intralimb coordination patterns describing hemiparetic locomotion at controlled speed. J. Neuroeng. Rehabil. 2013, 10, 53. [Google Scholar] [CrossRef] [Green Version]
- Burpee, J.L.; Lewek, M.D. Biomechanical gait characteristics of naturally occurring unsuccessful foot clearance during swing in individuals with chronic stroke. Clin. Biomech. 2015, 30, 1102–1107. [Google Scholar] [CrossRef]
- Bernhardt, J.; Hayward, K.S.; Kwakkel, G.; Ward, N.S.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; Boyd, L.A.; Carmichael, S.T.; Corbett, D.; et al. Agreed Definitions and a Shared Vision for New Standards in Stroke Recovery Research: The Stroke Recovery and Rehabilitation Roundtable Taskforce. Neurorehabilit. Neural Repair 2017, 31, 793–799. [Google Scholar] [CrossRef]
- Vilas-Boas, M.D.C.; Choupina, H.M.P.; Rocha, A.P.; Fernandes, J.M.; Cunha, J.P.S. Full-body motion assessment: Concurrent validation of two body tracking depth sensors versus a gold standard system during gait. J. Biomech. 2019, 87, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Refai, M.I.M.; Van Beijnum, B.-J.F.; Buurke, J.H.; Veltink, P.H. Portable Gait Lab: Tracking Relative Distances of Feet and CoM Using Three IMUs. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 2255–2264. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stroke | Control | p Value | |
|---|---|---|---|
| Number of subjects | 42 | 10 | |
| Age [years] | 52.3 (13.0) | 51.9 (14.8) | 0.93 |
| Sex [F/M] | 12/32 | 5/5 | 0.26 |
| Height [cm] | 166.5 (6.9) | 165.8 (7.1) | 0.77 |
| Weight [kg] | 62.8 (9.6) | 64.3 (14.1) | 0.68 |
| Affected side [R/L] | 21/23 | - | |
| Time after onset [months] | 42.5 (33.6) | - | |
| FMA-LE [0–34] | 25.9 (3.8) | - | |
| MAS quadriceps [0–5] | 0 (0, 1) | - | |
| MAS hamstrings [0–5] | 0 (0, 1) | - | |
| MAS gastrocnemius [0–5] | 1 (0.25, 2) | - | |
| SSWS [m/s] | 0.8 (0.3) | 1.4 (0.1) | <0.01 |
| GAIT total score [0–62] | 23.3 (8.9) | - | |
| GAIT swing subscore [0–24] | 9.8 (4.4) | - |
| Stroke | Control | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Affected Side | Non-Affected Side | Both Sides | ||||||||
| PTDmin | [%] | 98.5 | (2.1) | ** | 95.0 | (2.0) | * | ‡ | 96.1 | (1.0) |
| PTDmin timing | [%gait cycle] | 79.6 | (9.2) | 81.5 | (4.8) | ** | 76.5 | (1.8) | ||
| Frontal clearance peak | [deg] | 10.6 | (9.5) | ** | 2.2 | (6.5) | ‡ | 1.4 | (5.8) | |
| Frontal clearance peak timing | [%gait cycle] | 82.3 | (6.1) | ** | 88.2 | (10.6) | ‡ | 88.5 | (8.5) | |
| Hip hiking angle peak | [deg] | 4.5 | (4.7) | ** | 0.1 | (2.5) | ‡ | 0.6 | (1.2) | |
| Circumduction angle peak | [deg] | 6.7 | (6.5) | ** | 2.8 | (6.5) | ‡ | 1.7 | (6.3) | |
| Sagittal clearance peak | [deg] | 65.9 | (26.3) | ** | 94.2 | (14.1) | * | ‡ | 84.9 | (12.1) |
| Sagittal clearance peak timing | [%gait cycle] | 78.2 | (6.1) | 82.6 | (4.3) | ** | ‡ | 78.6 | (1.7) | |
| Hip flexion angle peak | [deg] | 28.3 | (8.1) | 34.9 | (6.8) | * | ‡ | 30.2 | (6.6) | |
| Knee flexion angle peak | [deg] | 42.0 | (5.8) | ** | 65.2 | (9.5) | ‡ | 65.2 | (5.3) | |
| Ankle dorsiflexion angle peak | [deg] | 5.8 | (7.8) | 9.5 | (5.2) | * | ‡ | 6.2 | (4.7) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haruyama, K.; Kawakami, M.; Okada, K.; Okuyama, K.; Tsuzuki, K.; Liu, M. Pelvis-Toe Distance: 3-Dimensional Gait Characteristics of Functional Limb Shortening in Hemiparetic Stroke. Sensors 2021, 21, 5417. https://doi.org/10.3390/s21165417
Haruyama K, Kawakami M, Okada K, Okuyama K, Tsuzuki K, Liu M. Pelvis-Toe Distance: 3-Dimensional Gait Characteristics of Functional Limb Shortening in Hemiparetic Stroke. Sensors. 2021; 21(16):5417. https://doi.org/10.3390/s21165417
Chicago/Turabian StyleHaruyama, Koshiro, Michiyuki Kawakami, Kohsuke Okada, Kohei Okuyama, Keita Tsuzuki, and Meigen Liu. 2021. "Pelvis-Toe Distance: 3-Dimensional Gait Characteristics of Functional Limb Shortening in Hemiparetic Stroke" Sensors 21, no. 16: 5417. https://doi.org/10.3390/s21165417