
Smart Patch for Skin Temperature: Preliminary Study to Evaluate Psychometrics and Feasibility

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
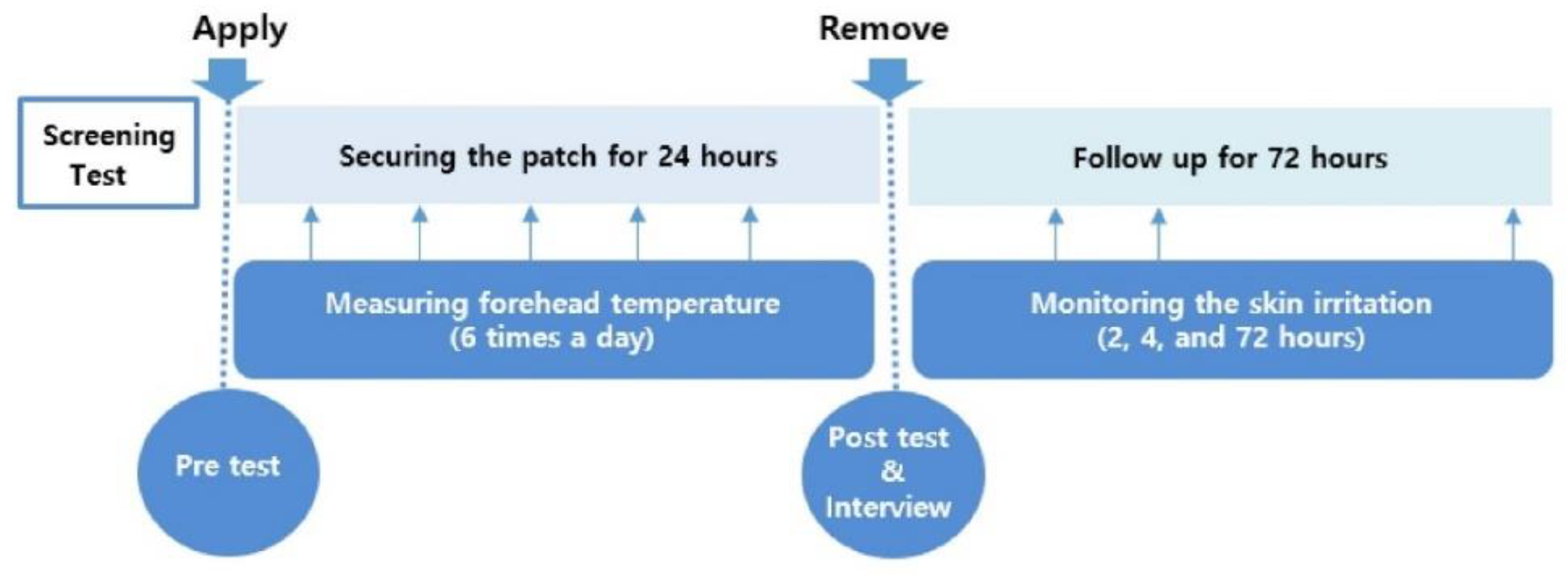
2.1. Study Design
2.2. Ethical Consideration
2.3. Study Participants
2.4. Measures
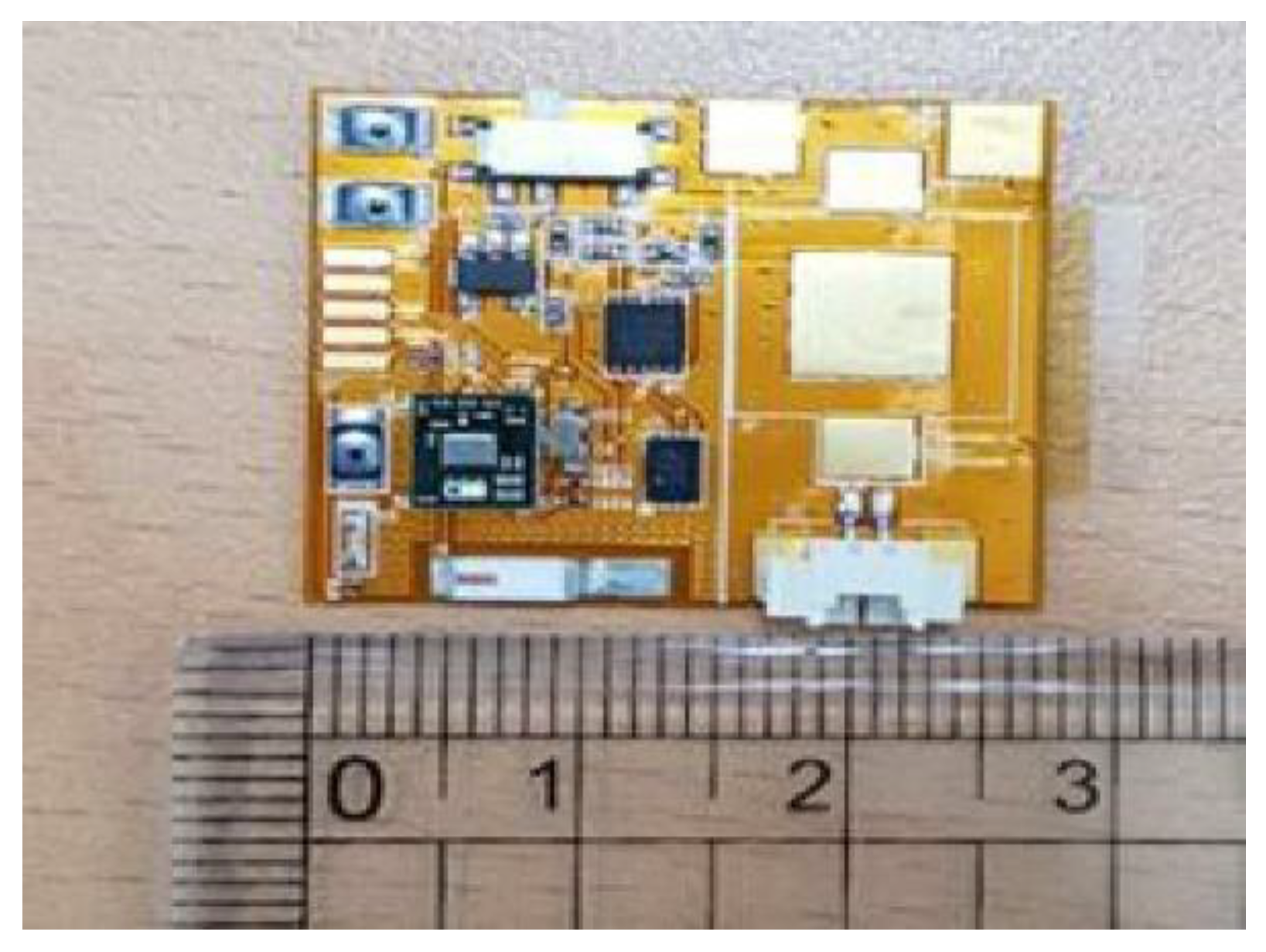
Description of Smart Patch for Skin Temperature
2.5. Data Collection
2.6. Data Analysis
3. Results
3.1. Description of the Study Participants
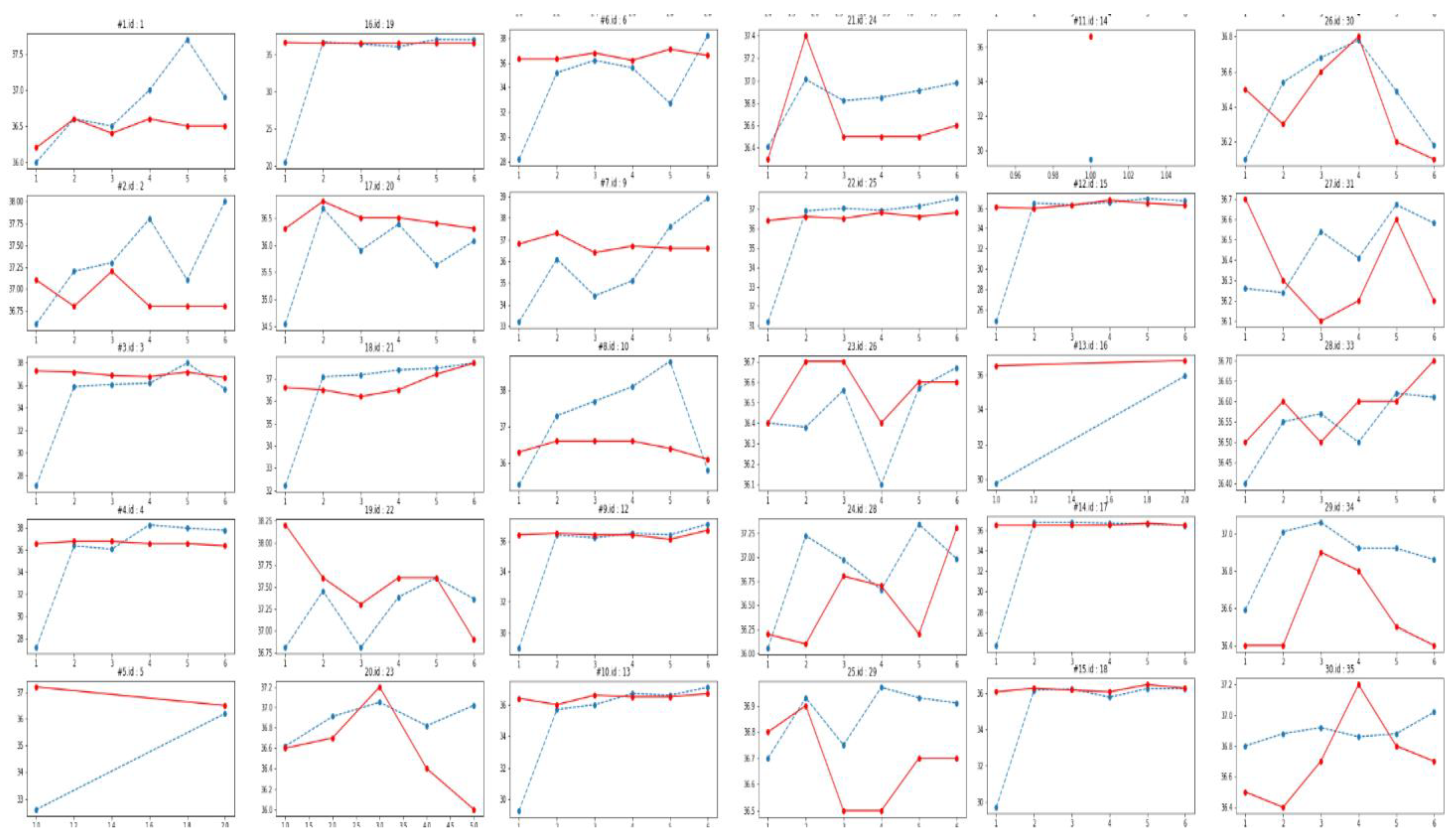
3.2. Comparison between Infrared Forehead and Smart Patch Body Temperatures
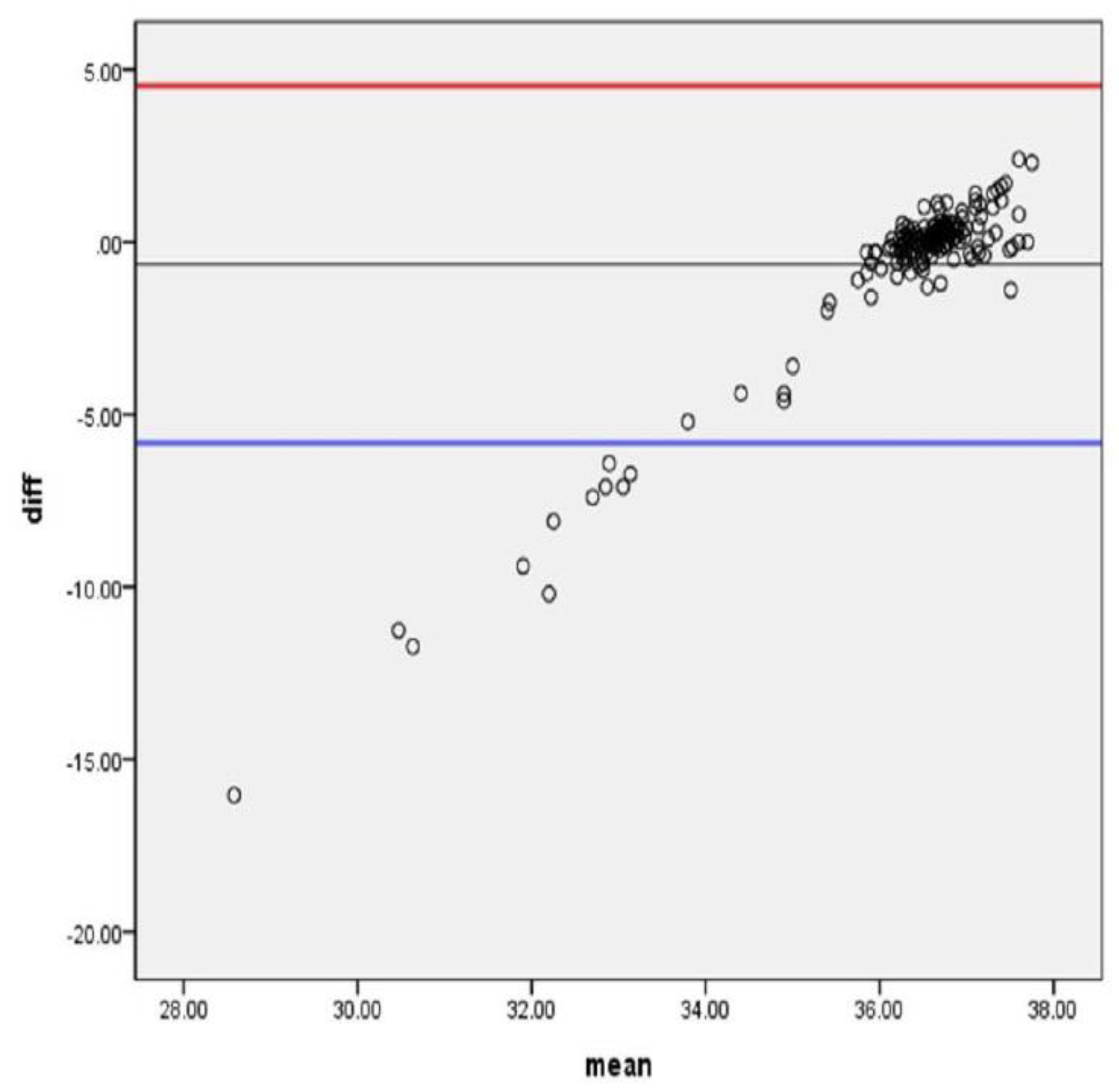
3.3. Consistency between Two Body Temperatures
3.4. Considerations of Users’ Intrapersonal Characteristics
3.5. Smart Patch Body Temperature Explained by Users’ Environmental Characteristics
3.6. Diagnostic Validity to Detect the Febrile Condition
3.7. User Evaluation
4. Discussion
4.1. Implication for Clinical Practice
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
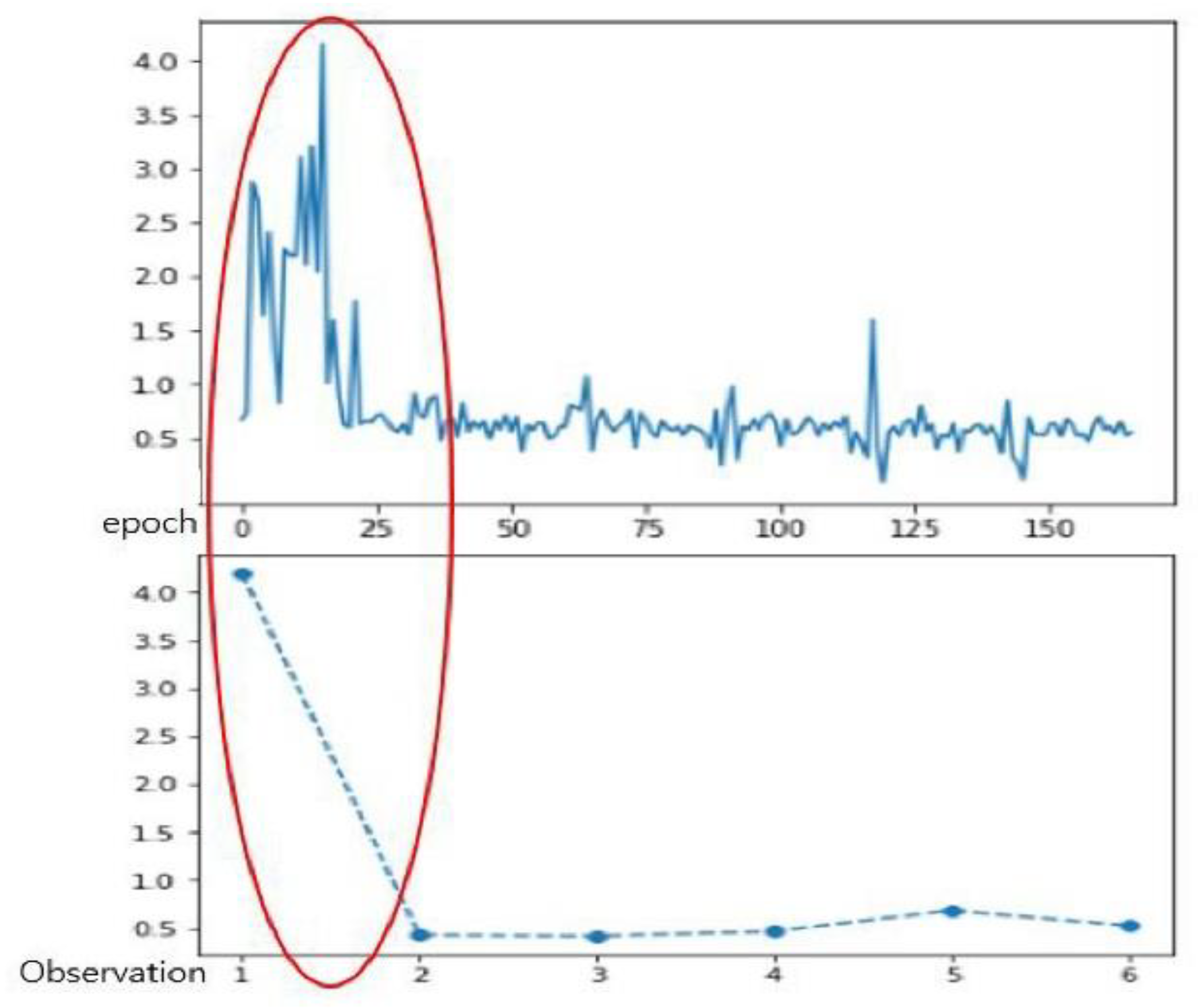
Appendix A. Individual Graphs of Two Measured Temperatures

Appendix B. Skin Observation before Attaching, during Attacking and after Detaching the Smart Patch
| Participant A |  |  |  |
| Participant B |  |  |  |
| Before attaching | During attaching | After detaching |
References
- Cox, R.A.; García-Palmieri, M.R. Cholesterol, triglycerides, and associated lipoproteins. In Clinical Methods: The History, Physical, and Laboratory Examinations, 3rd ed.; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworths: Boston, MA, USA, 1990. [Google Scholar]
- Beker, B.M.; Cervellera, C.; De Vito, A.; Musso, C.G. Human physiology in extreme heat and cold. Int. Arch. Clin. Physiol. 2018, 1, 1–8. [Google Scholar]
- Centers for Disease Control and Prevention. Prevent Hypothermia & Frostbite. Available online: https://www.cdc.gov/disasters/winter/staysafe/hypothermia.html (accessed on 14 December 2020).
- Basak, T.; Aciksoz, S.; Tosun, B.; Akyuz, A.; Acikel, C. Comparison of three different thermometers in evaluating the body temperature of healthy young adult individuals. Int. J. Nurs. Pract. 2013, 19, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.L.; Seal, R.F.; Spady, D.W.; Joffres, M.R. Comparison of esophageal, rectal, axillary, bladder, tympanic, and pulmonary artery temperatures in children. J. Pediatr. 1998, 133, 553–556. [Google Scholar] [CrossRef]
- Erickson, R.S.; Woo, T.M. Accuracy of infrared ear thermometry and traditional temperature methods in young children. Heart Lung 1994, 23, 181–195. [Google Scholar] [PubMed]
- Lodha, R.; Mukerji, N.; Sinha, N.; Pandey, R.M.; Jain, Y. Is axillary temperature an appropriate surrogate for core temperature? Indian J. Pediatr. 2000, 67, 571–574. [Google Scholar] [CrossRef]
- Casa, D.J.; Becker, S.M.; Ganio, M.S.; Brown, C.M.; Yeargin, S.W.; Roti, M.W.; Siegler, J.; Blowers, J.A.; Glaviano, N.R.; Huggins, R.A.; et al. Validity of devices that assess body temperature during outdoor exercise in the heat. J. Athl. Train. 2007, 42, 333–342. [Google Scholar]
- Ganio, M.S.; Brown, C.M.; Casa, D.J.; Becker, S.M.; Yeargin, S.W.; McDermott, B.P.; Boots, L.M.; Boyd, P.W.; Armstrong, L.E.; Maresh, C.M. Validity and reliability of devices that assess body temperature during indoor exercise in the heat. J. Athl. Train. 2009, 44, 124–135. [Google Scholar] [CrossRef] [Green Version]
- Hunt, A.; Bach, A.; Borg, D.; Costello, J.; Stewart, I. The systematic bias of ingestible core temperature sensors requires a correction by linear regression. Front. Physiol. 2017, 8, 260. [Google Scholar] [CrossRef] [Green Version]
- Canadian Agency for Drugs and Technology in Health. Non-Contact Thermometers for Detecting Fever: A Review of Clinical Effectiveness. Available online: https://www.ncbi.nlm.nih.gov/books/NBK263237/pdf/Bookshelf_NBK263237.pdf (accessed on 14 December 2020).
- Duncan, A.L.; Bell, A.J.; Chu, K.; Greenslade, J.H. Can a non-contact infrared thermometer be used interchangeably with other thermometers in an adult emergency department. Australas. Emerg. Nurs. J. 2008, 11, 130–134. [Google Scholar] [CrossRef]
- Food and Drug Administration. Non-Contact Temperature Assessment Devices During the COVID-19 Pandemic. Available online: https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-devices/non-contact-temperature-assessment-devices-during-covid-19-pandemic (accessed on 15 December 2020).
- Centers for Disease Control and Prevention. Non-Contact Temperature Measurement Devices: Considerations for Use in Port of Entry Screening Activities. Available online: https://stacks.cdc.gov/view/cdc/24857/cdc_24857_DS1.pdf? (accessed on 15 December 2020).
- Gostic, K.; Gomez, A.C.; Mummah, R.O.; Kucharski, A.J.; Lloyd-Smith, J.O. Estimated effectiveness of symptom and risk screening to prevent the spread of COVID-19. Elife 2020, 9, e55570. [Google Scholar] [CrossRef] [PubMed]
- Aw, J. The non-contact handheld cutaneous infra-red thermometer for fever screening during the COVID-19 global emergency. J Hosp. Infect. 2020, 104, 451. [Google Scholar] [CrossRef] [PubMed]
- Moreira, D.G.; Costello, J.T.; Brito, C.J.; Adamczyk, J.G.; Ammer, K.; Bach, A.J.E.; Costa, C.M.A.; Eglin, C.; Fernandes, A.A.; Fernández-Cuevas, I.; et al. Thermographic imaging in sports and exercise medicine: A Delphi study and consensus statement on the measurement of human skin temperature. J. Therm. Biol. 2017, 69, 155–162. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Yamamoto, D.; Takada, M.; Naito, H.; Arie, T.; Akita, S.; Takei, K. Efficient skin temperature sensor and stable gel-less sticky ECG sensor for a wearable flexible healthcare patch. Adv. Healthc. Mater. 2017, 6, 1700495–1700502. [Google Scholar] [CrossRef] [PubMed]
- Tamura, T.; Huang, M.; Togawa, T. Current developments in wearable thermometers. Adv. Biomed. Eng. 2018, 7, 88–99. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.; Wu, F.; Redouté, J.M.; Yuce, M.R. An autonomous wireless body area network implementation towards IoT connected healthcare applications. IEEE Access 2017, 5, 11413–11422. [Google Scholar] [CrossRef]
- Weigel, M.; Lu, T.; Bailly, G.; Oulasvirta, A.; Majidi, C.; Steimle, J. Iskin: Flexible, Stretchable and Visually Customizable On-Body Touch Sensors for Mobile Computing. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems, Seoul, Korea, 18–23 April 2015; pp. 2991–3000. [Google Scholar]
- Uejio, C.K.; Morano, L.H.; Jung, J.; Kintziger, K.; Jagger, M.; Chalmers, J.; Holmes, T. Occupational heat exposure among municipal workers. Int. Arch. Occup. Environ. Health 2018, 91, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Mazgaoker, S.; Ketko, I.; Yanovich, R.; Heled, Y.; Epstein, Y. Measuring core body temperature with a non-invasive sensor. J. Therm. Biol. 2017, 66, 17–20. [Google Scholar] [CrossRef]
- Weenk, M.; van Goor, H.; Frietman, B.; Engelen, L.J.; van Laarhoven, C.J.; Smit, J.; Bredie, S.J.; van de Belt, T.H. Continuous monitoring of vital signs using wearable devices on the general ward: Pilot study. JMIR mhealth uhealth 2017, 5, e91. [Google Scholar] [CrossRef] [PubMed]
- Pesonen, E.; Silvasti-Lundell, M.; Niemi, T.T.; Kivisaari, R.; Hernesniemi, J.; Mäkinen, M.T. The focus of temperature monitoring with zero-heat-flux technology (3M Bair-Hugger): A clinical study with patients undergoing craniotomy. J. Clin. Monit. Comput. 2019, 33, 917–923. [Google Scholar] [CrossRef] [Green Version]
- Appelboom, G.; Camacho, E.; Abraham, M.E.; Bruce, S.S.; Dumont, E.L.; Zacharia, B.E.; D’Amico, R.; Slomian, J.; Reginster, J.Y.; Bruyère, O.; et al. Smart wearable body sensors for patient self-assessment and monitoring. Arch. Public Health 2014, 72, 28–37. [Google Scholar] [CrossRef] [Green Version]
- Bevan, N.; Carter, J.; Earthy, J.; Geis, T.; Harker, S. New ISO Standards for Usability, Usability Reports and Usability Measures. In Human-Computer Interaction. Theory, Design, Development and Practice; Kurosu, M., Ed.; Lecture Notes in Computer Science LNCS; Springer: Cham, Switzerland, 2016; Volume 9731, pp. 268–278. [Google Scholar]
- Lee, S.; Gandla, S.; Naqi, M.; Jung, U.; Kang, S.; Youn, H.; Pyun, D.; Rhee, Y.; Kwon, H.J.; Kim, H.; et al. All-day mobile healthcare monitoring system based on heterogeneous stretchable sensors for medical Emergency. IEEE Trans. Ind. Electron. 2019, 67, 8808–8816. [Google Scholar] [CrossRef]
- Billingham, S.A.; Whitehead, A.L.; Julious, S.A. An audit of sample sizes for pilot and feasibility trials being undertaken in the United Kingdom registered in the United Kingdom Clinical Research Network database. BMC Med. Res. Methodol. 2013, 13, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.; Jung, W.; Oh, H.; Kim, Y.; Kim, E.; Kim, M.; Shin, H. Diagnostic accuracy of temporal artery temperatures measurements. J. Korean Clin. Nurs. Res. 2018, 24, 227–234. [Google Scholar]
- Joo, G.; Sohng, K.Y. Accuracy, precision, and validity of fever detection using non-invasive temperature measurement in adult coronary care unit patients with pulmonary catheters. J. Korean Acad. Nurs. 2012, 42, 424–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.J.; Park, S.H.; Kang, C.B. Systematic review and meta-analyses of diagnostic accuracy of infrared thermometer when identifying fever in children. J. Korean Acad. Nurs. 2013, 43, 746–759. [Google Scholar] [CrossRef]
- Garcia-Souto, M.D.P.; Dabnichki, P. Non-invasive and wearable early fever detection system for young children. Measurement 2018, 116, 216–229. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.M.; Altman, D.G. Agreement between methods of measurement with multiple observations per individual. J. Biopharm. Stat. 2007, 17, 571–582. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. RSV Surveillance Case Definitions. Available online: https://www.who.int/influenza/rsv/rsv_case_definition/en/ (accessed on 25 May 2020).
- Hunt, A.P.; Buller, M.J.; Maley, M.J.; Costello, J.T.; Stewart, I.B. Validity of a noninvasive estimation of deep body temperature when wearing personal protective equipment during exercise and recovery. Mil. Med. Res. 2019, 6, 20. [Google Scholar] [CrossRef] [Green Version]
- Yun, K.W.; Lim, I.S. A study for accuracy and usefulness of tympanic membrane and forehead thermometers. Korean J. Pediatr. 2005, 48, 820–825. [Google Scholar]
- Staley, K. Changing what researchers ‘think and do’: Is this how involvement impacts on research? Res. All 2017, 1, 158–167. [Google Scholar] [CrossRef]
- Staley, K.; Abbey-Vital, I.; Nolan, C. The impact of involvement on researchers: A learning experience. Res Involv. Engagem. 2017, 3, 1–9. [Google Scholar] [CrossRef] [PubMed]
- North, B. The Growing Role of Human Factors and Usability Engineering for Medical Devices. In What’s Required in The New Regulatory Landscape; British Standards Institution: London, UK, 2015. [Google Scholar]
- Mainz, G. Feasibility of Human Factors Research in Medical Device Development. Master’s Thesis, Johns Hopkins University, Baltimore, MD, USA, 2018. [Google Scholar]
- World Health Organization. Managing Epidemics: Key Facts about Major Deadly Diseases. Available online: https://apps.who.int/iris/handle/10665/272442 (accessed on 28 May 2020).
- Michaud, L.; Büla, C.; Berney, A.; Camus, V.; Voellinger, R.; Stiefel, F.; Burnand, B. Delirium: Guidelines for general hospitals. J. Psychosom. Res. 2007, 62, 371–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BT1 (Smart Patch) | BT2 (Infrared Forehead) | Mean Difference of BT1-BT2 | Correlation of BT1 and BT2 | ||
|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | t (p) | r (p) | |
| Time 1 | 36.58 (0.43) | 32.53 (4.60) | −4.05 (4.56) | −4.78 (<0.001) | 0.14 (0.482) |
| Time 2 | 36.62 (0.39) | 36.58 (0.52) | −0.04 (0.57) | −0.38 (0.709) | 0.23 (0.236) |
| Time 3 | 36.61 (0.29) | 36.56 (0.61) | −0.05 (0.60) | −0.47 (0.643) | 0.27 (0.168) |
| Time 4 | 36.62 (0.29) | 36.72 (0.70) | 0.10 (0.66) | 0.80 (0.432) | 0.35 (0.074) |
| Time 5 | 36.10 (0.34) | 36.89 (1.05) | 0.28 (1.12) | 1.28 (0.210) | −0.04 (0.856) |
| Time 6 | 36.61 (0.33) | 36.98 (0.74) | 0.37 (0.67) | 2.85 (0.009) | 0.43 (0.030) |
| Mean Difference of BT1-BT2 | |||
|---|---|---|---|
| Position | n(%) | M (SD) | F (p) |
| Sitting | 106 (74.6) | −0.72 (2.70) | 0.229 (0.796) |
| Supine | 12 (8.5) | −0.19 (3.06) | |
| Standing | 24 (16.9) | −0.53 (2.60) | |
| N = 133 at Times 1–6 | N = 87 at Times 2–4 | |
|---|---|---|
| B (p) | B (p) | |
| Ambient temperature | −0.079 (0.373) | −0.114 (0.337) |
| Ambient humidity | 0.048 (0.596) | −0.163 (0.152) |
| Infrared forehead body temperature | 0.188 (0.033) | 0.315 (0.006) |
| R2 (p) | 0.046 (0.099) | 0.125 (0.014) |
| Square root of the sum of the error at squared | 0.742 | 0.581 |
| Cutoff | 37.3 °C | 37.5 °C | ||
|---|---|---|---|---|
| Value | 95% CI | Value | 95% CI | |
| Sensitivity | 0.50 | (0.18, 0.82) | 0.50 | (0.09, 0.91) |
| Specificity | 0.84 | (0.82, 0.86) | 0.89 | (0.88, 0.91) |
| Positive predictive value | 0.17 | (0.06, 0.27) | 0.13 | (0.01, 0.28) |
| Negative predictive value | 0.96 | (0.94, 0.99) | 0.98 | (0.97, 0.99) |
| ROC | 0.71 | (0.53, 0.99) | 0.90 | (0.85, 0.95) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Kim, S.; Lee, M.; Rhee, Y.; Lee, S.; Jeong, Y.-R.; Kang, S.; Naqi, M.; Hong, S. Smart Patch for Skin Temperature: Preliminary Study to Evaluate Psychometrics and Feasibility. Sensors 2021, 21, 1855. https://doi.org/10.3390/s21051855
Kim H, Kim S, Lee M, Rhee Y, Lee S, Jeong Y-R, Kang S, Naqi M, Hong S. Smart Patch for Skin Temperature: Preliminary Study to Evaluate Psychometrics and Feasibility. Sensors. 2021; 21(5):1855. https://doi.org/10.3390/s21051855
Chicago/Turabian StyleKim, Heejung, Sunkook Kim, Mingoo Lee, Yumie Rhee, Sungho Lee, Yi-Rang Jeong, Sunju Kang, Muhammad Naqi, and Soyun Hong. 2021. "Smart Patch for Skin Temperature: Preliminary Study to Evaluate Psychometrics and Feasibility" Sensors 21, no. 5: 1855. https://doi.org/10.3390/s21051855