
Development of a Wearable Mouth Guard Device for Monitoring Teeth Clenching during Exercise

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
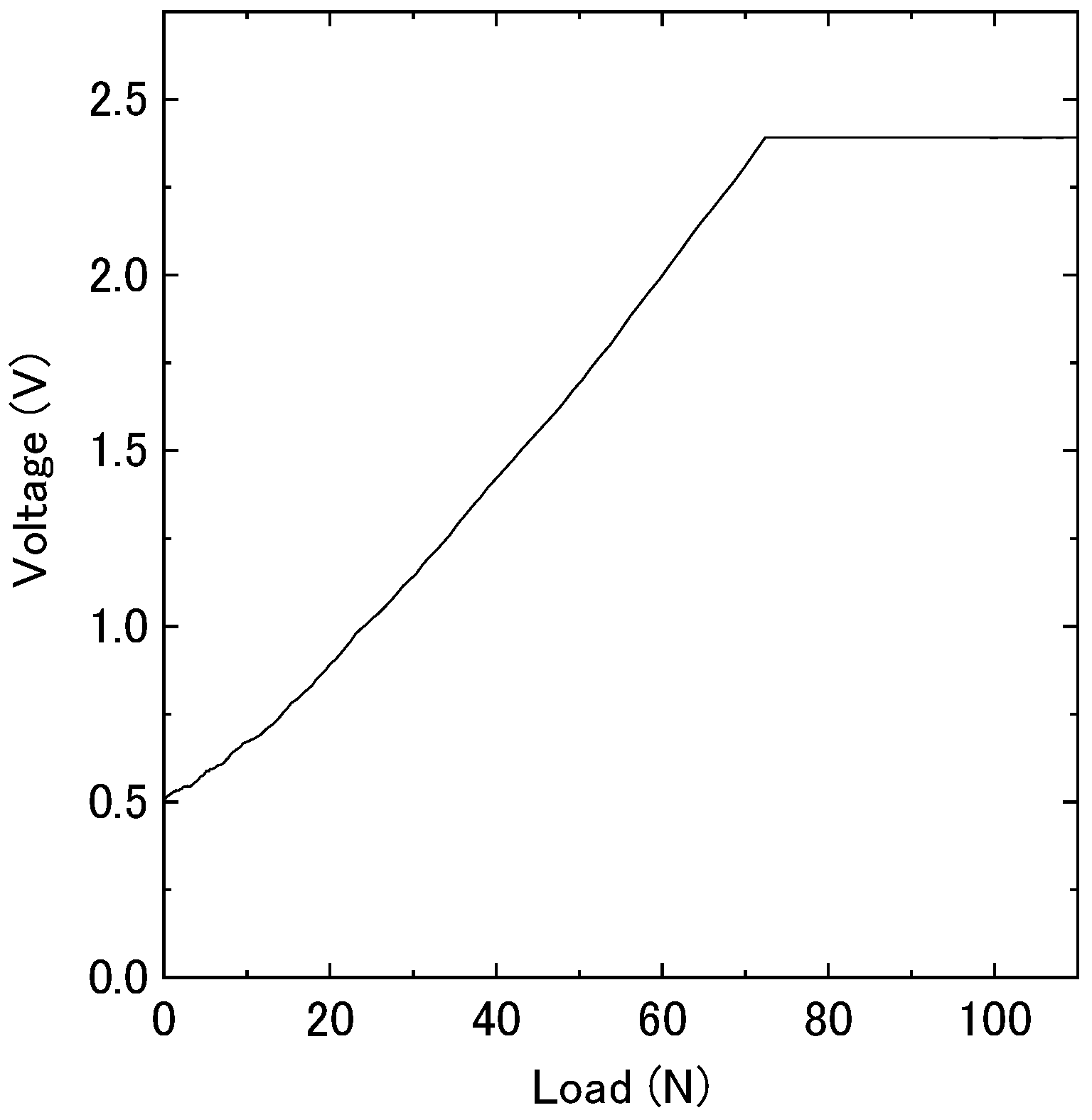
2.1. Response of the Force Sensor in MG Materials
2.2. Fabrication of the MG Sensor
2.3. Dental Occlusion Test with the MG Sensor
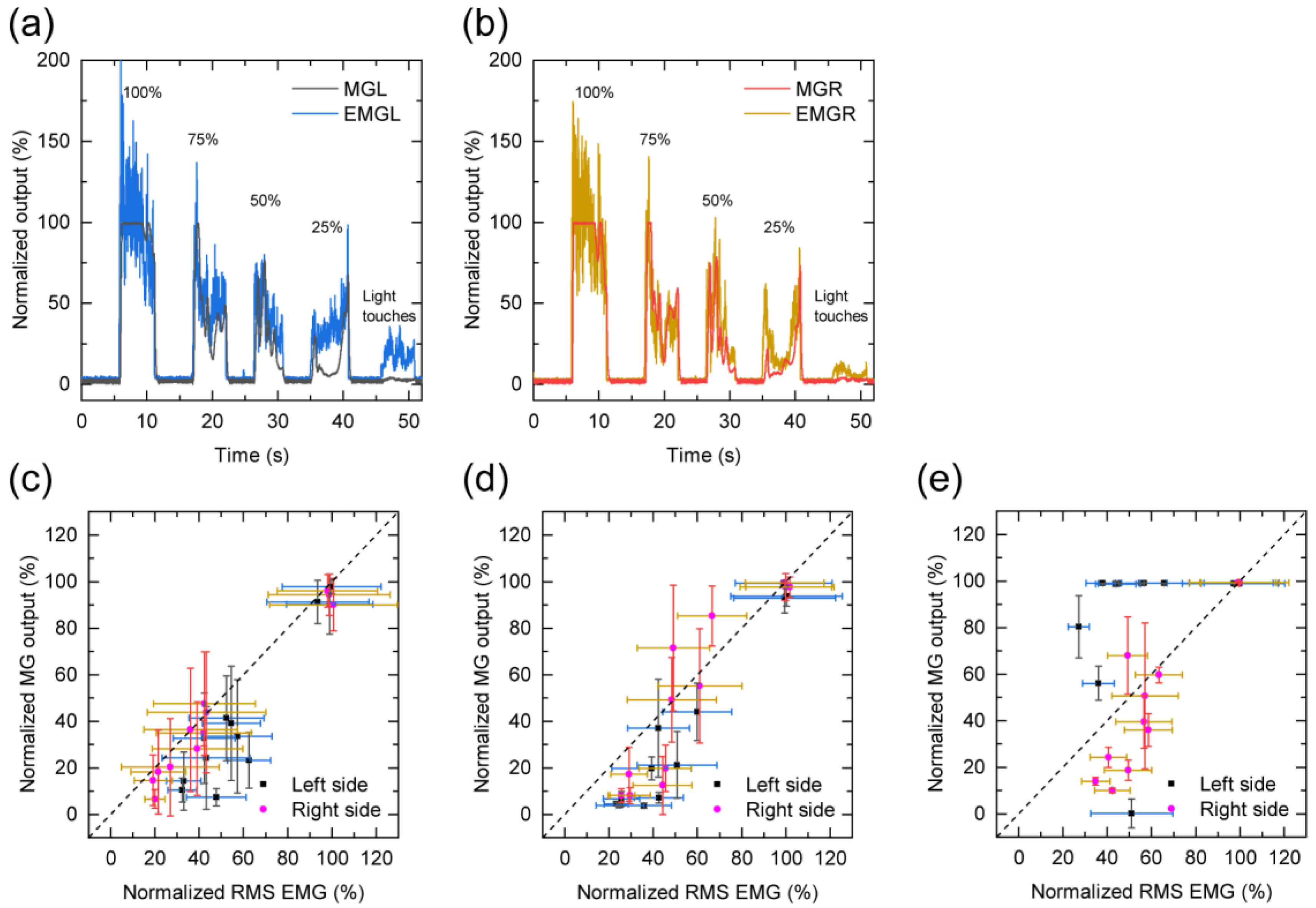
- Teeth clenching: teeth clenching, performed for 5 s at four different clenching intensity levels from 100% to 25% in steps of 25%, and light teeth touches were examined using visual feedback control to determine the relationship between the sensitivity of the MG sensor and the EMG. The participants were instructed to match each intensity level of the MG sensor output displayed on a monitor in front of them.
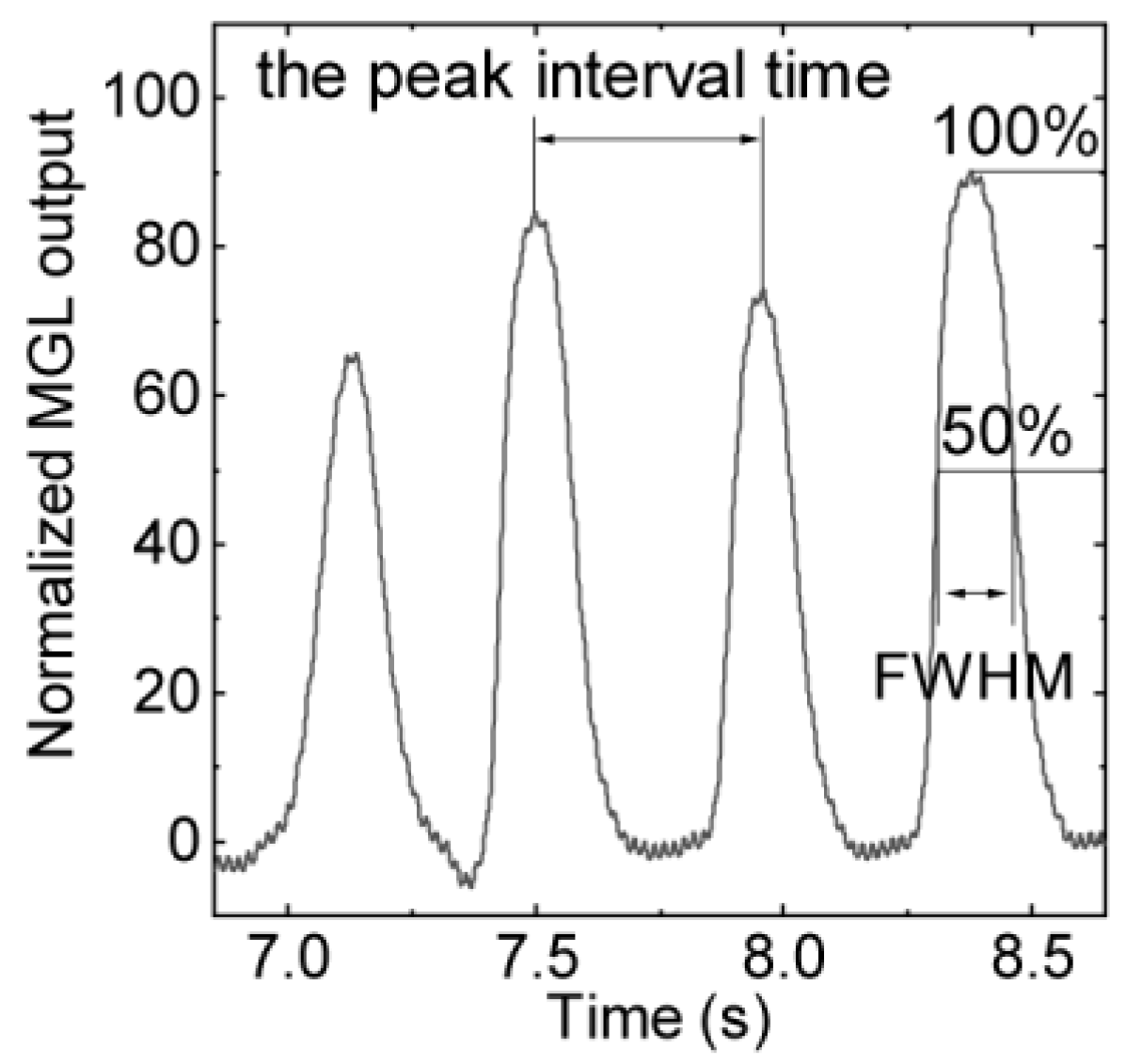
- Teeth tapping: strong and quick teeth-tapping tasks were examined for approximately 10 s to compare the temporal resolutions of both sides of the force sensors in the MG sensor and EMGs using the peak interval time and the full width at half maximum (FWHM).
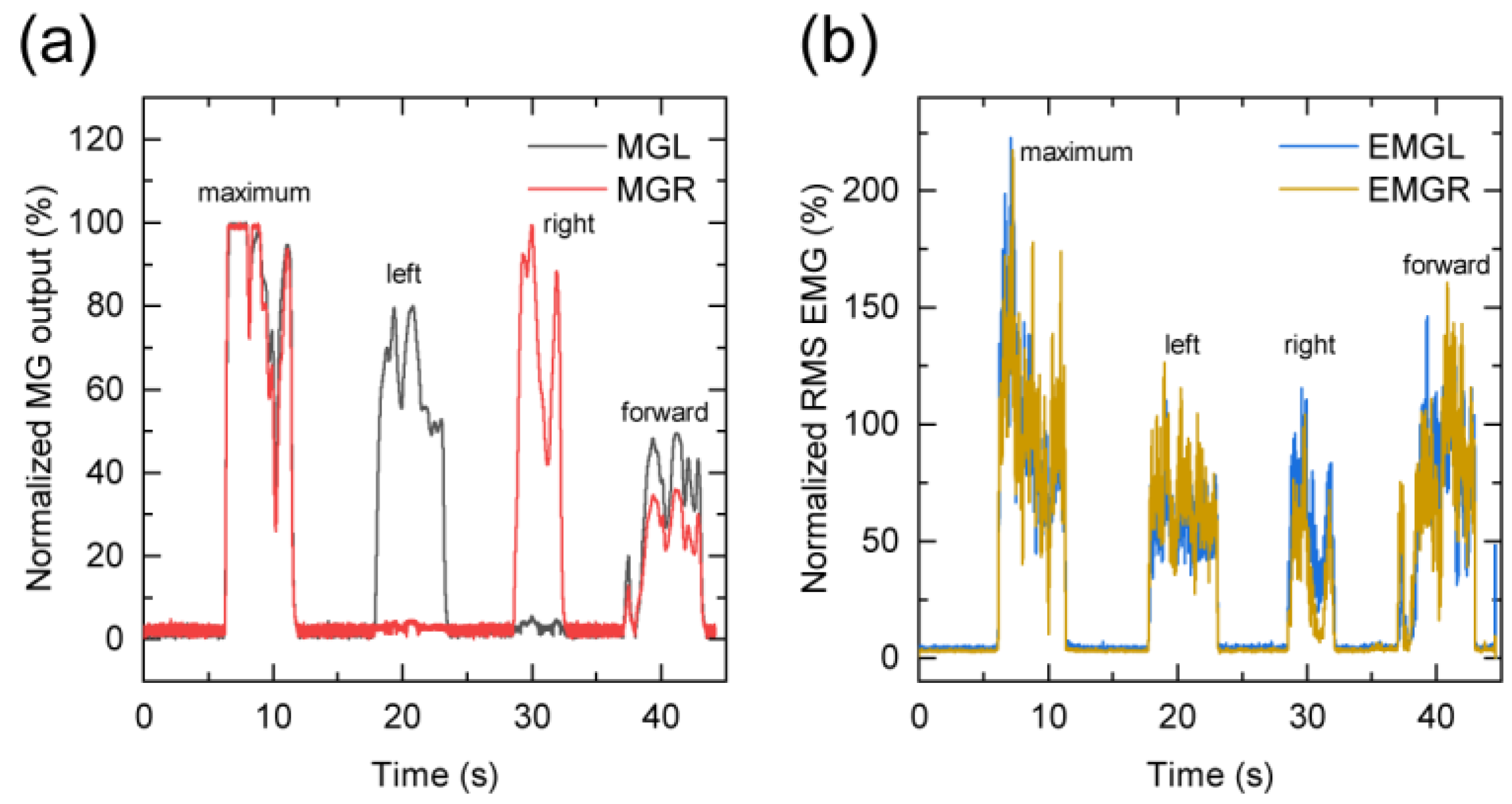
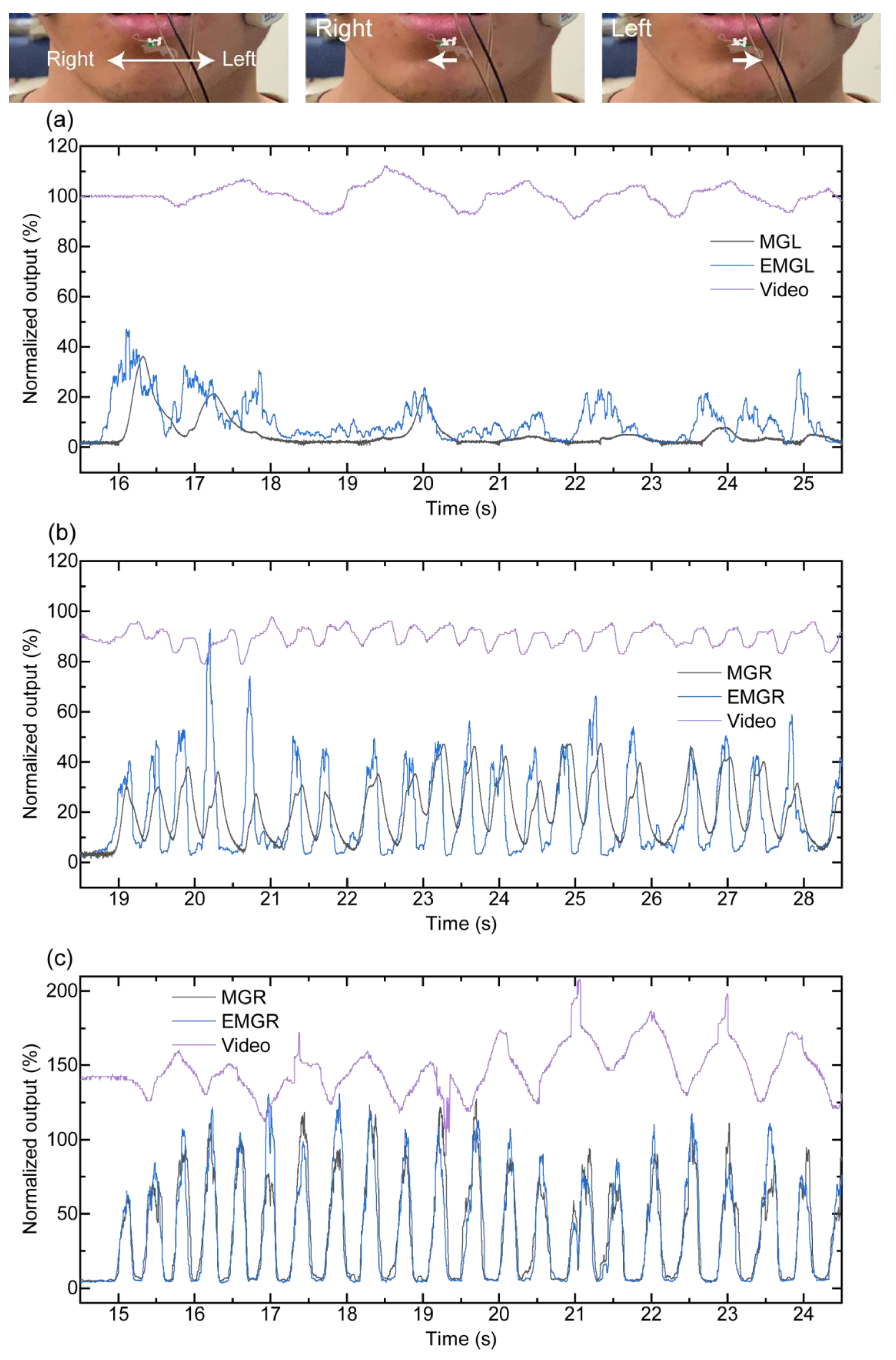
- Jaw movement: first, maximum voluntary teeth clenching was performed at the intercuspal position. After holding at the resting position, left lateral movement of the mandible, right lateral movement of the mandible, and movement of the lower jaw to the protruded position, teeth clenching was performed to check the responses of the left and right force sensors when the mandible moved from side to side and forward. Each motion required 5 s, and there was a 5-s interval between the different motions.
- Teeth grinding: the participants ground their teeth laterally for approximately 10 s; the EMG was compared with the MG sensor output obtained from teeth grinding.
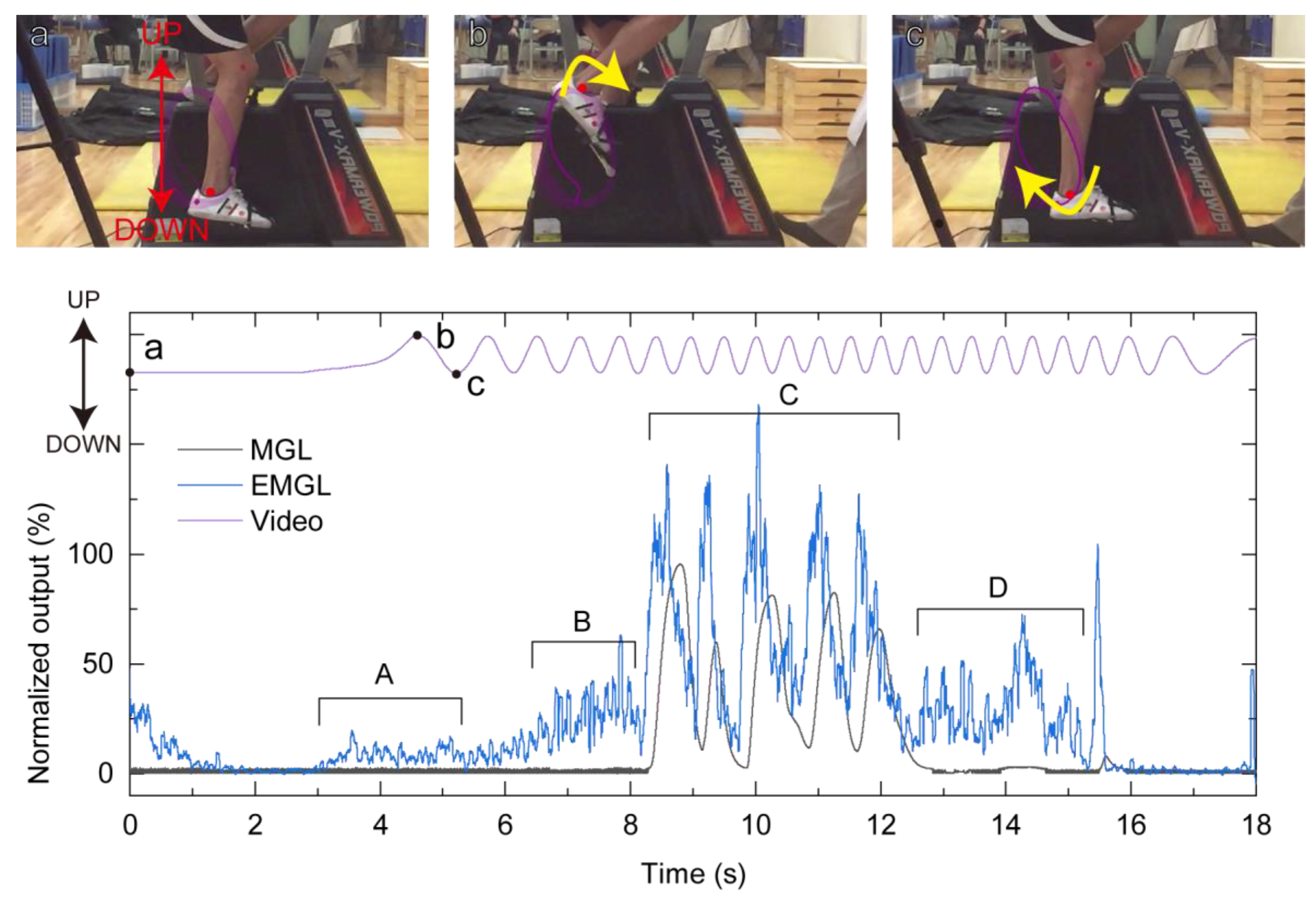
2.4. Demonstration Measurement during Exercise
3. Results
3.1. Sensitivity of the Force Sensor in MG Materials
3.2. MG Sensor Response to the Dental Occlusion Test
3.3. Exercise Tolerance Test with MG Sensor
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ohkawa, S.; Shinohara, K.; Hashihara, M.; Adachi, S.; Gurita, T.; Komura, I.; Yoshida, M.; Nishinaka, H.; Yatuzuka, N.; Abe, Y.; et al. Sports Medical Analysis on Masticatory Muscles Function in Volleyball and Handball Players. J. Jpn. Soc. Stomatognath. Funct. 1994, 1, 33–44. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, S.; Hirai, T.; Koshino, H.; Yokoyama, Y.; Ishijima, T. Influence of Teeth Clenching on the Bodily Equilibrium against Striking Weight Impact. Prosthodont. Res. Pract. 2006, 5, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Fujino, S.; Takahashi, T.; Ueno, T. Influence of Voluntary Teeth Clenching on the Stabilization of Postural Stance Disturbed by Electrical Stimulation of Unilateral Lower Limb. Gait Posture 2010, 31, 122–125. [Google Scholar] [CrossRef]
- Jung, J.K.; Chae, W.S.; Lee, K.B. Analysis of the Characteristics of Mouthguards that Affect Isokinetic Muscular Ability and Anaerobic Power. J. Adv. Prosthodont. 2013, 5, 388–395. [Google Scholar] [CrossRef] [Green Version]
- Baldini, A.; Nota, A.; Tripodi, D.; Longoni, S.; Tecco, S. Dental Occlusion and Sports Performance: A Critical Review. Gazz. Med. Ital. 2013, 172, 791–797. [Google Scholar]
- Hasegawa, K.; Takeda, T.; Nakajima, K.; Ozawa, T.; Ishigami, K.; Narimatsu, K.; Noh, K. Does Clenching Reduce Indirect Head Acceleration during Rugby Contact? Dent. Traumatol. 2014, 30, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Grosdent, S.; O’Thanh, R.; Domken, O.; Lamy, M.; Croisier, J.L. Dental Occlusion Influences Knee Muscular Performances in Asymptomatic Females. J. Strength Cond. Res. 2014, 28, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Narimatsu, K.; Takeda, T.; Nakajima, K.; Konno, M.; Ozawa, T.; Ishigami, K. Effect of Clenching with a Mouthguard on Head Acceleration during Heading of a Soccer Ball. Gen. Dent. 2015, 63, 41–46. [Google Scholar] [PubMed]
- Julià-Sánchez, S.; Álvarez-Herms, J.; Gatterer, H.; Burtscher, M.; Pagès, T.; Viscor, G. The Influence of Dental Occlusion on the Body Balance in Unstable Platform Increases after High Intensity Exercise. Neurosci. Lett. 2016, 617, 116–121. [Google Scholar] [CrossRef]
- Lloyd, J.D.; Nakamura, W.S.; Maeda, Y.; Takeda, T.; Leesungbok, R.; Lazarchik, D.; Dorney, B.; Gonda, T.; Nakajima, K.; Yasui, T.; et al. Mouthguards and their Use in Sports: Report of the 1st International Sports Dentistry Workshop, 2016. Dent. Traumatol. 2017, 33, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Yoshida, Y.; Churei, H.; Aizawa, J.; Hirohata, K.; Ohmi, T.; Ohji, S.; Takahashi, T.; Enomoto, M.; Ueno, T.; et al. The Effect of Teeth Clenching on Dynamic Balance at Jump-Landing: A Pilot Study. J. Appl. Biomech. 2017, 33, 211–215. [Google Scholar] [CrossRef] [Green Version]
- Mitsuyama, A.; Takahashi, T.; Ueno, T. Effects of Teeth Clenching on the Soleus H Reflex during Lower Limb Muscle Fatigue. J. Prosthodont. Res. 2017, 61, 202–209. [Google Scholar] [CrossRef]
- Ferreira, G.B.; Guimarães, L.S.; Fernandes, C.P.; Dias, R.B.; Coto, N.P.; Antunes, L.A.A.; Antunes, L.S. Is there Enough Evidence that Mouthguards do not Affect Athletic Performance? A Systematic Literature Review. Int. Dent. J. 2018, 69, 25–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leroux, E.; Leroux, S.; Maton, F.; Ravalec, X.; Sorel, O. Influence of Dental Occlusion on the Athletic Performance of Young Elite Rowers: A Pilot Study. Clinics 2018, 73, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Dias, A.A.; Redinha, L.A.; Silva, L.M.; Pezarat-Correia, P.C. Effects of Dental Occlusion on Body Sway, Upper Body Muscle Activity and Shooting Performance in Pistol Shooters. Appl. Bionics Biomech. 2018, 2018, 9360103. [Google Scholar] [CrossRef]
- Julià-Sánchez, S.; Álvarez-Herms, J.; Burtscher, M. Dental Occlusion and Body Balance: A Question of Environmental Constraints? J. Oral Rehabil. 2019, 46, 388–397. [Google Scholar] [CrossRef]
- Hoshino, H.; Koshino, H. The Relationship between Occlusal Force and Power Profile during Exercise by Alpine Skiers. J. Sports Dent. 2019, 23, 1–7. [Google Scholar]
- Takeuchi, M.; Shimosato, T. Study of Teeth-clenching in Sports. J. Sports Dent. 2019, 22, 42–49. [Google Scholar]
- Nukaga, H.; Takeda, T.; Nakajima, K.; Narimatsu, K.; Ozawa, T.; Ishigami, K.; Funato, K. Masseter Muscle Activity in Track and Field Athletes: A Pilot Study. Open Dent. J. 2016, 10, 474–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asano, T. Masticatory Muscle Activities during Snatch Weightlifting. Int. J. Sports Dent. 2009, 1, 33–40. [Google Scholar]
- Hoshino, H.; Takeda, H.; Koshino, H. Investigation of the Relationship between Occlusal Force, Jaw Stability, and Power Properties for Alpine Skiers. J. Ski Sci. 2015, 12, 15–24. [Google Scholar]
- Michelotti, A.; Buonocore, G.; Farella, M.; Pellegrino, G.; Piergentili, C.; Altobelli, S.; Martina, R. Postural Stability and Unilateral Posterior Crossbite: Is there a Relationship? Neurosci. Lett. 2006, 392, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Bourdin, M.; Brunet-Patru, I.; Hager, P.E.; Allard, Y.; Hager, J.P.; Lacour, J.R.; Moyen, B. Influence of Maxillary Mouthguards on Physiological Parameters. Med. Sci. Sports Exerc. 2006, 38, 1500–1504. [Google Scholar] [CrossRef] [PubMed]
- Von Arx, T.; Flury, R.; Tschan, J.; Buergin, W.; Geiser, T. Exercise Capacity in Athletes with Mouthguards. Int. J. Sports Med. 2008, 29, 435–438. [Google Scholar] [CrossRef]
- Yamazaki, G.; Takeda, T.; Nakajima, K.; Konno, M.; Ozawa, T.; Ishigami, K. Influence of Experimentally Deviated Mandibular Position on Static Standing Posture. Int. J. Sports Dent. 2014, 7, 085–093. [Google Scholar]
- Sakaguchi, K.; Mehta, N.R.; Abdallah, E.F.; Forgione, A.G.; Hirayama, H.; Kawasaki, T.; Yokoyama, A. Examination of the Relationship Between Mandibular Position and Body Posture. Cranio J. 2007, 25, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Bergamini, M.; Pierleoni, F.; Gizdulich, A.; Bergamini, C. Dental Occlusion and Body Posture: A Surface EMG Study. Cranio J. 2008, 26, 25–32. [Google Scholar] [CrossRef]
- Tardieu, C.; Dumitrescu, M.; Giraudeau, A.; Blanc, J.L.; Cheynet, F.; Borel, L. Dental Occlusion and Postural Control in Adults. Neurosci. Lett. 2009, 450, 221–224. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, C.M.; Lowery, M.M.; Doherty, L.S.; McHugh, M.; O’Muircheartaigh, C.; Cullen, J.; Nolan, P.; McNicholas, W.T.; O’Malley, M.J. Improved Surface EMG Electrode for Measuring Genioglossus Muscle Activity. Respir. Physiol. Neurobiol. 2007, 159, 55–67. [Google Scholar] [CrossRef]
- Diaz Lantada, A.; González Bris, C.; Lafont Morgado, P.; Sanz Maudes, J. Novel System for Bite-Force Sensing and Monitoring Based on Magnetic Near Field Communication. Sensors 2012, 12, 11544–11558. [Google Scholar] [CrossRef] [Green Version]
- Camarillo, D.B.; Shull, P.B.; Mattson, J.; Shultz, R.; Garza, D. An Instrumented Mouthguard for Measuring Linear and Angular Head Impact Kinematics in American Football. Ann. Biomed. Eng. 2013, 41, 1939–1949. [Google Scholar] [CrossRef] [Green Version]
- Kuo, C.; Wu, L.C.; Hammoor, B.T.; Luck, J.F.; Cutcliffe, H.C.; Lynall, R.C.; Kait, J.R.; Campbell, K.R.; Mihalik, J.P.; Bass, C.R.; et al. Effect of the Mandible on Mouthguard Measurements of Head Kinematics. J. Biomech. 2016, 49, 1845–1853. [Google Scholar] [CrossRef]
- Arakawa, T.; Kuroki, Y.; Nitta, H.; Chouhan, P.; Toma, K.; Sawada, S.; Takeuchi, S.; Sekita, T.; Akiyoshi, K.; Minakuchi, S.; et al. Mouthguard Biosensor with Telemetry System for Monitoring of Saliva Glucose: A Novel Cavitas Sensor. Biosens. Bioelectron. 2016, 84, 106–111. [Google Scholar] [CrossRef] [Green Version]
- Toma, K.; Tomoto, K.; Yokota, K.; Yasuda, N.; Ishikawa, T.; Arakawa, T.; Mitsubayashi, K. Mouthguard Controller for Unconstrained Control of External Devices. Sensors Mater. 2018, 30, 3053–3060. [Google Scholar] [CrossRef]
- Bridgman, H.; Kwong, M.T.; Bergmann, J.H.M. Mechanical Safety of Embedded Electronics for In-body Wearables: A Smart Mouthguard Study. Ann. Biomed. Eng. 2019, 47, 1725–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.C.; Kuo, C.; Loza, J.; Kurt, M.; Laksari, K.; Yanez, L.Z.; Senif, D.; Anderson, S.C.; Miller, L.E.; Urban, J.E.; et al. Detection of American Football Head Impacts Using Biomechanical Features and Support Vector Machine Classification. Sci. Rep. 2018, 8, 1–14. [Google Scholar] [CrossRef]
- Mizumachi, M.; Sumita, Y.; Ueno, T. Effect of Wearing a Mouthguard on the Vestibulocollic Reflex. J. Sci. Med. Sport 2008, 11, 191–197. [Google Scholar] [CrossRef]
- Hayashi, K.; Churei, H.; Tanabe, G.; Togawa, K.; Chowdhury, R.U.; Ueno, T. Improving the Wearing Rate of Mouthguards in the Youth Rugby Category Affects the Total Future Mouthguard Wearing Rate. Dent. J. 2020, 8, 77. [Google Scholar] [CrossRef]
- Bousdras, V.A.; Cunningham, J.L.; Ferguson-Pell, M.; Bamber, M.A.; Sindet-Pedersen, S.; Blunn, G.; Goodship, A.E. A Novel Approach to Bite Force Measurements in a Porcine Model in Vivo. Int. J. Oral Maxillofac. Surg. 2006, 35, 663–667. [Google Scholar] [CrossRef]
- Testa, M.; Di Marco, A.; Pertusio, R.; Van Roy, P.; Cattrysse, E.; Roatta, S. A Validation Study of a New Instrument for Low Cost Bite Force Measurement. J. Electromyogr. Kinesiol. 2016, 30, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Somogyi, S.; Wenisch, T.F.; Hardavellas, N.; Kim, J.; Ailamaki, A.; Falsafi, B. Bite Force Recording Devices—A Review. J. Clin. Diagn. Res. 2017, 11, 1–5. [Google Scholar] [CrossRef]
- Talwar, R.M.; Ellis, E.; Throckmorton, G.S. Adaptations of the Masticatory System after Bilateral Fractures of the Mandibular Condylar Process. J. Oral Maxillofac. Surg. 1998, 56, 430–439. [Google Scholar] [CrossRef]
- Moriya, Y.; Tuchida, K.; Moriya, Y.; Sawada, T.; Koga, J.; Sato, J.; Nishikawa, M.; Takizawa, T.; Uematsu, H.; Ozaki, T.; et al. The Influence of Craniofacial form on Bite Force and EMG Activity of Masticatory Muscles VIII-1. Bite Force of Complete Denture Wearers. J. Oral Sci. 1999, 41, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Bakke, M. Bite Force and Occlusion. Semin. Orthod. 2006, 12, 120–126. [Google Scholar] [CrossRef]
- Takada, K.; Yashiro, K.; Sorihashi, Y.; Morimoto, T.; Sakuda, M. Tongue, jaw, and lip muscle activity and jaw movementduring experimental chewing efforts in man. J. Dent. Res. 1996, 75, 1598–1606. [Google Scholar] [CrossRef] [PubMed]
- Schieppati, M.; Di, F.G.; Nardone, A. Patterns of activityof perioral facial muscles during mastication in man. Exp. Brain Res. 1989, 77, 103–112. [Google Scholar] [CrossRef]
- Himejima, A.; Shirao, K.; Tsurumi, A.; Tanaka, M.; Morita, S. Occlusal Contact and Muscle Activity during Judo. Int. J. Sports Dent. 2013, 6, 43–56. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sensor Type | Objective | Performances | |
|---|---|---|---|
| Diaz et al. (2012) [30] | Force sensor | Monitoring of human bruxism | Bruxism events in vitro trials were performed for validation Force sensor (ZFLEX A201-100, Tekscan Inc., South Boston, MA, USA) was used. Measurement range: 0–about 1000 N, Sampling rate: unknown, in vitro and in vivo tests |
| Camarillo et al. (2013) [31] | Acceleration sensor | Measuring 6-DOF head kinematic response during impact | Laboratory-based impact testing performed at points on the helmet and facemask |
| Kuo et al. (2016) [32] | Acceleration sensor (and force sensor) | To evaluate the mandible constraint’s effect on MG’s kinematic measurement accuracy | Free fall drop experiments performed on football helmeted ATD * and PMHS * heads over a range of impact locations and heights while varying the mandible constraint Force sensor (FlexiForce A201, Tekscan Inc., South Boston, MA, USA) was used to check mandible constraint, Measurement range: −300 N, Sampling rate: unknown, in vitro test |
| Toma et al. (2018) [34] | Force sensor | Expecting that oral motion can be used to control external devices because occlusion or tongue motion remains possible for tetraplegics | Measuring occlusal pressures at three different positions—front tooth and right and left second molars—in an MG-type controller with pressure sensors Measurement range 1.7–50.2 N, Sampling rate: unknown (data from a logger were transmitted with a time interval or 30 s.), in vitro test |
| Wu et al. (2018) [36] | Acceleration sensor | For detecting field football head impacts | Validating instrumented MG data from collegiate football games and practices, with ground truth data established from video review |
| Proposed study | Force sensor | For monitoring timing, duration, and a degree of teeth clenching during exercise to explain the relationship between teeth clenching and sports performance | Four types of dental occlusion tests -clenching, tapping, jaw movement and grinding- and an exercise tolerance test with an MG sensor device Measurement range: 0–100 N, Sampling rate: 1000 Hz, in vivo test |
| The Mean of Peak Interval Time (msec) | The Mean of Full Width at Half Maximum (msec) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Participant | Trial | MGL | MGR | EMGL | EMGR | MGL | MGR | EMGL | EMGR |
| A | 1 | 280 ± 23 a | 297 ± 64 a | 281 ± 33 a | 280 ± 24 a | 166 ± 16 a | 159 ± 17 a | 110 ± 22 b | 107 ± 17 b |
| 2 | 303 ± 22 a | 303 ± 22 a | 305 ± 22 a | 302 ± 26 a | 173 ± 8 a | 173 ± 10 a | 109 ± 25 b | 104 ± 24 b | |
| 3 | 296 ± 27 a | 296 ± 29 a | 295 ± 39 a | 294 ± 35 a | 166 ± 13 a | 166 ± 17 a | 107 ± 22 b | 108 ± 21 b | |
| B | 1 | 563 ± 48 a | 564 ± 50 a | 566 ± 51 a | 566 ± 61 a | 227 ± 30 a | 234 ± 30 a | 228 ± 35 a | 236 ± 38 a |
| 2 | 312 ± 19 a | 312 ± 18 a | 312 ± 23 a | 311 ± 24 a | 159 ± 11 a | 161 ± 9 a | 109 ± 19 b | 114 ± 20 b | |
| 3 | 305 ± 23 a | 305 ± 22 a | 304 ± 31 a | 304 ± 27 a | 160 ± 10 a | 160 ± 9 a | 115 ± 21 b | 127 ± 22 b | |
| C | 1 | 337 ± 19 a | 337 ± 19 a | 336 ± 28 a | 336 ± 32 a | 239 ± 27 a | 196 ± 18 b | 136 ± 32 c | 130 ± 30 c |
| 2 | 323 ± 24 a | 323 ± 21 a | 323 ± 44 a | 321 ± 31 a | 240 ± 40 a | 198 ± 24 b | 134 ± 30 c | 135 ± 28 c | |
| 3 | 311 ± 21 a | 311 ± 18 a | 308 ± 39 a | 313 ± 40 a | 235 ± 30 a | 193 ± 19 b | 137 ± 24 c | 136 ± 29 c | |
| Left (%) | Right (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Participant | Trial | MGL | MGR | EMGL | EMGR | MGL | MGR | EMGL | EMGR |
| A | 1 | 66 ± 10 | 3.2 ± 0.7 | 61 ± 11 | 67 ± 17 | 3.4 ± 0.9 | 72 ± 19 | 57 ± 21 | 36 ± 23 |
| 2 | 70 ± 8 | 4.4 ± 0.6 | 72 ± 15 | 76 ± 22 | 4.2 ± 1.1 | 85 ± 14 | 71 ± 21 | 42 ± 22 | |
| 3 | 72 ± 4 | 4.7 ± 0.3 | 68 ± 15 | 100 ± 22 | 4.9 ± 1.0 | 81 ± 9 | 79 ± 19 | 54 ± 33 | |
| B | 1 | 56 ± 11 | 65 ± 17 | 74 ± 26 | 83 ± 18 | 49 ± 6 | 99 ± 0.3 | 71 ± 11 | 83 ± 18 |
| 2 | 70 ± 13 | 82 ± 10 | 82 ± 28 | 82 ± 17 | 21 ± 11 | 40 ± 13 | 41 ± 18 | 56 ± 16 | |
| 3 | 59 ± 14 | 85 ± 13 | 57 ± 14 | 69 ± 13 | 43 ± 7 | 84 ± 7 | 57 ± 9 | 62 ± 13 | |
| C | 1 | 86 ± 4 | 2.4 ± 0.2 | 49 ± 8 | 36 ± 6 | 70 ± 4 | 99 ± 0.2 | 65 ± 12 | 79 ± 22 |
| 2 | 89 ± 2 | 2.4 ± 0.3 | 49 ± 8 | 39 ± 7 | 56 ± 1 | 83 ± 4 | 42 ± 6 | 53 ± 9 | |
| 3 | 91 ± 2 | 2.6 ± 0.2 | 45 ± 8 | 39 ± 7 | 54 ± 6 | 78 ± 5 | 34 ± 9 | 55 ± 10 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinjo, R.; Wada, T.; Churei, H.; Ohmi, T.; Hayashi, K.; Yagishita, K.; Uo, M.; Ueno, T. Development of a Wearable Mouth Guard Device for Monitoring Teeth Clenching during Exercise. Sensors 2021, 21, 1503. https://doi.org/10.3390/s21041503
Kinjo R, Wada T, Churei H, Ohmi T, Hayashi K, Yagishita K, Uo M, Ueno T. Development of a Wearable Mouth Guard Device for Monitoring Teeth Clenching during Exercise. Sensors. 2021; 21(4):1503. https://doi.org/10.3390/s21041503
Chicago/Turabian StyleKinjo, Rio, Takahiro Wada, Hiroshi Churei, Takehiro Ohmi, Kairi Hayashi, Kazuyoshi Yagishita, Motohiro Uo, and Toshiaki Ueno. 2021. "Development of a Wearable Mouth Guard Device for Monitoring Teeth Clenching during Exercise" Sensors 21, no. 4: 1503. https://doi.org/10.3390/s21041503