
The Impact of Environment on Gait Assessment: Considerations from Real-World Gait Analysis in Dementia Subtypes


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Clinical and Cognitive Assessment
2.3. Gait Assessment
2.4. Data Processing
2.5. Data Analysis
3. Results
3.1. Participants
3.2. Proportion of Complete Datasets
3.3. Does Lab-Based and Real-World Gait Assessment Produce Similar Signatures of Gait Impairment?
3.3.1. Lab-Based Gait Assessment
3.3.2. Real-World Gait
3.3.3. Associations between Lab-Based and Real-World Gait
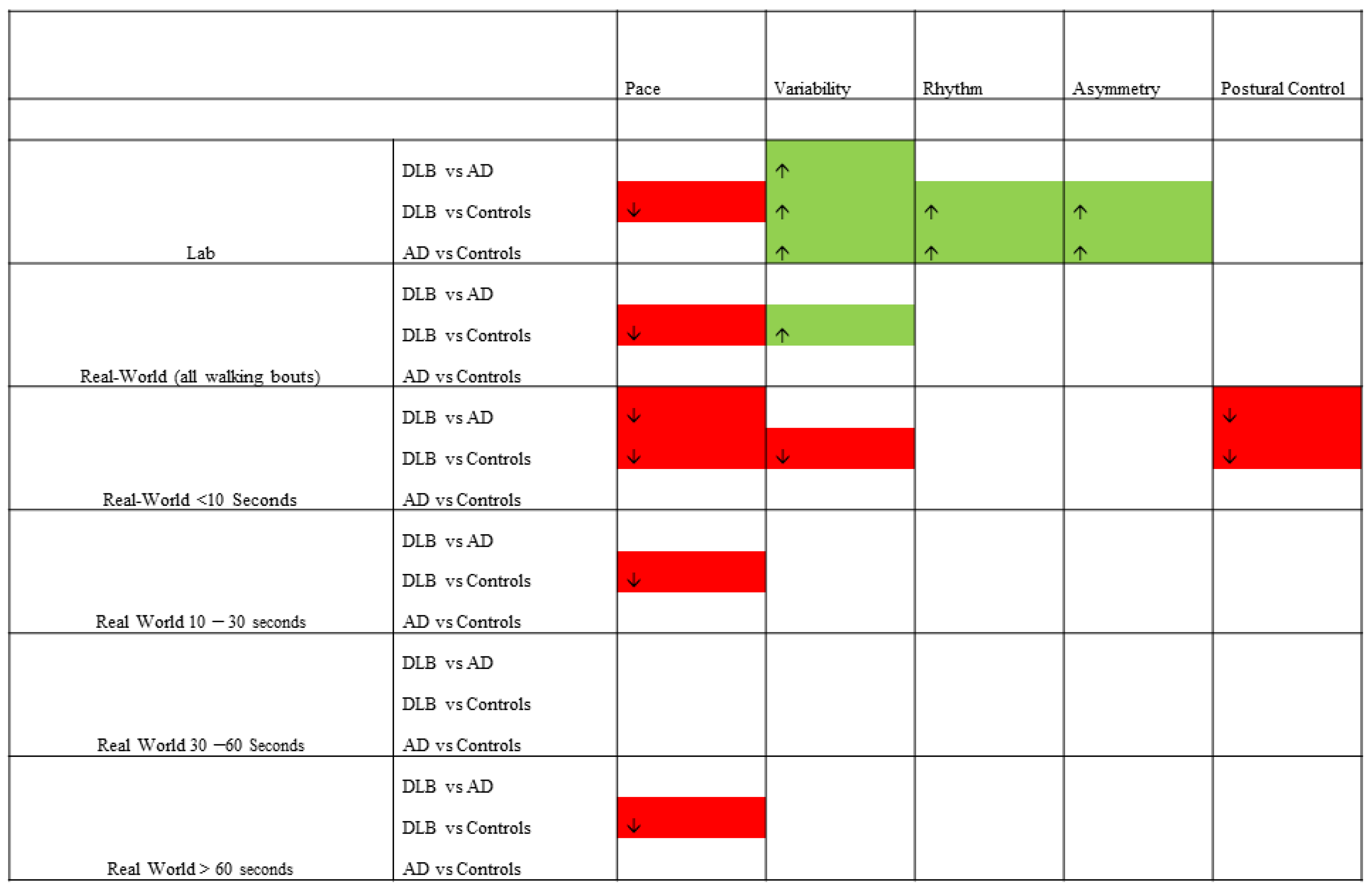
3.4. Do Discrete Bout Lengths Impact Discriminative Signatures of Gait Impairment in the Real World?
4. Discussion
4.1. The Impact of Environment on Gait
4.2. Challenges and Future Directions for the Application of Wearable Technology to Assess Real-World Gait
4.3. Strengths and Limitations of the Current Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Del Din, S.; Elshehabi, M.; Galna, B.; Hobert, M.A.; Warmerdam, E.; Suenkel, U.; Brockmann, K.; Metzger, F.; Hansen, C.; Berg, D.; et al. Gait analysis with wearables predicts conversion to Parkinson disease. Ann. Neurol. 2019, 86, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Del Din, S.; Godfrey, A.; Galna, B.; Lord, S.; Rochester, L. Free-living gait characteristics in ageing and Parkinson’s disease: Impact of environment and ambulatory bout length. J. Neuroeng. Rehabilit. 2016, 13, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mc Ardle, R.; Galna, B.; Donaghy, P.; Thomas, A.; Rochester, L. Do Alzheimer’s and Lewy body disease have discrete pathological signatures of gait? Alzheimer’s Dement. 2019, 15, 1367–1377. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.A.; Hickey, A.; Lord, S.; Del Din, S.; Godfrey, A.; Rochester, L. Comprehensive measurement of stroke gait characteristics with a single accelerometer in the laboratory and community: A feasibility, validity and reliability study. J. Neuroeng. Rehabilit. 2017, 14, 130. [Google Scholar] [CrossRef] [PubMed]
- Rochester, L.; Galna, B.; Lord, S.; Msc, D.M.; Eglon, G.; Chinnery, P.F. Gait impairment precedes clinical symptoms in spinocerebellar ataxia type 6. Mov. Disord. 2014, 29, 252–255. [Google Scholar] [CrossRef] [PubMed]
- Galna, B.; Lord, S.; Burn, D.J.; Rochester, L. Progression of gait dysfunction in incident Parkinson’s disease: Impact of medication and phenotype. Mov. Disord. 2015, 30, 359–367. [Google Scholar] [CrossRef]
- Morris, R.; Lord, S.; Bunce, J.; Burn, D.; Rochester, L. Gait and cognition: Mapping the global and discrete relationships in ageing and neurodegenerative disease. Neurosci. Biobehav. Rev. 2016, 64, 326–345. [Google Scholar] [CrossRef]
- Del Din, S.; Galna, B.; Godfrey, A.; Bekkers, E.M.J.; Pelosin, E.; Nieuwhof, F.; Mirelman, A.; Hausdorff, J.M.; Rochester, L. Analysis of Free-Living Gait in Older Adults With and Without Parkinson’s Disease and With and Without a History of Falls: Identifying Generic and Disease-Specific Characteristics. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2019, 74, 500–506. [Google Scholar] [CrossRef]
- Weiss, A.; Herman, T.; Giladi, N.; Hausdorff, J.M. Objective assessment of fall risk in Parkinson’s disease using a body-fixed sensor worn for 3 days. PLoS ONE 2014, 9, e96675. [Google Scholar] [CrossRef] [Green Version]
- Weiss, A.; Herman, T.; Giladi, N.; Hausdorff, J.M. New evidence for gait abnormalities among Parkinson’s disease patients who suffer from freezing of gait: Insights using a body-fixed sensor worn for 3 days. J. Neural Transm. 2015, 122, 403–410. [Google Scholar] [CrossRef]
- Lord, S.; Galna, B.; Yarnall, A.J.; Coleman, S.; Burn, D.; Rochester, L. Predicting first fall in newly diagnosed P arkinson’s disease: Insights from a fall-naïve cohort. Mov. Disord. 2016, 31, 1829–1836. [Google Scholar] [CrossRef] [PubMed]
- Buckley, C.; Alcock, L.; McArdle, R.; Rehman, R.Z.U.; Del Din, S.; Mazzà, C.; Yarnall, A.J.; Rochester, L. The Role of Movement Analysis in Diagnosing and Monitoring Neurodegenerative Conditions: Insights from Gait and Postural Control. Brain Sci. 2019, 9, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beauchet, O.; Launay, C.; Montero-Odasso, M.; Annweiler, C.; Allali, G. Anti-dementia drugs-related changes in gait performance while single and dual tasking in patients with Alzheimer disease: A meta-analysis. Curr. Alzheimer Res. 2015, 12, 761–771. [Google Scholar] [CrossRef] [PubMed]
- Mc Ardle, R.; Morris, R.; Hickey, A.; Del Din, S.; Koychev, I.; Gunn, R.N.; Lawson, J.; Zamboni, G.; Ridha, B.; Sahakian, B.J.; et al. Gait in Mild Alzheimer’s Disease: Feasibility of Multi-Center Measurement in the Clinic and Home with Body-Worn Sensors: A Pilot Study. J. Alzheimer’s Dis. 2018, 63, 331–341. [Google Scholar] [CrossRef]
- Del Din, S.; Godfrey, A.; Mazza, C.; Lord, S.; Rochester, L. Free-living monitoring of Parkinson’s disease: Lessons from the field. Mov. Disord. 2016, 31, 1293–1313. [Google Scholar] [CrossRef]
- Orendurff, M.S.; Schoen, J.A.; Bernatz, G.C.; Segal, A.D.; Klute, G.K. How humans walk: Bout duration, steps per bout, and rest duration. J. Rehabilit. Res. Dev. 2008, 45, 1077–1089. [Google Scholar] [CrossRef]
- Gold, M.; Amatniek, J.; Carillo, M.C.; Cedarbaum, J.M.; Hendrix, J.A.; Miller, B.B.; Robillard, J.M.; Rice, J.J.; Soares, H.; Tome, M.B.; et al. Digital technologies as biomarkers, clinical outcomes assessment, and recruitment tools in Alzheimer’s disease clinical trials. Alzheimer’s Dement. 2018, 4, 234–242. [Google Scholar] [CrossRef]
- Mc Ardle, R.; Del Din, S.; Galna, B.; Thomas, A.; Rochester, L. Differentiating dementia disease subtypes with gait analysis: Feasibility of wearable sensors? Gait Posture 2020, 76, 372–376. [Google Scholar] [CrossRef]
- McKeith, I.G. Author response: Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology 2018, 90, 300. [Google Scholar] [CrossRef] [Green Version]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimers disease: Recommendations from the NIAAA workgroups on diagnostic guidelines for Alzheimers disease. Alzheimer’s Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litvan, I.; Goldman, J.G.; Tröster, A.I.; Schmand, B.A.; Weintraub, D.; Petersen, R.C.; Mollenhauer, B.; Adler, C.H.; Marder, K.; Williams-Gray, C.H.; et al. Diagnostic criteria for mild cognitive impairment in Parkinson’s disease: Movement Disorder Society Task Force guidelines. Mov. Disord. 2012, 27, 349–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donaghy, P.C.; Taylor, J.-P.; O’Brien, J.T.; Barnett, N.; Olsen, K.; Colloby, S.J.; Lloyd, J.; Petrides, G.; McKeith, I.G.; Thomas, A.J. Neuropsychiatric symptoms and cognitive profile in mild cognitive impairment with Lewy bodies. Psychol. Med. 2018, 48, 2384–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, E.; O’Brien, J.T.; Donaghy, P.; Morris, C.; Barnett, N.; Olsen, K.; Martin-Ruiz, C.; Taylor, J.-P.; Thomas, A.J. Peripheral inflammation in prodromal Alzheimer’s and Lewy body dementias. J. Neurol. Neurosurg. Psychiatry 2017, 89, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Hickey, A.; Del Din, S.; Rochester, L.; Godfrey, A. Detecting free-living steps and walking bouts: Validating an algorithm for macro gait analysis. Physiol. Meas. 2017, 38, N1–N15. [Google Scholar] [CrossRef]
- Del Din, S.; Godfrey, A.; Rochester, L. Validation of an accelerometer to quantify a comprehensive battery of gait characteristics in healthy older adults and Parkinson’s disease: Toward clinical and at home use. IEEE J. Biomed. Health Inform. 2016, 20, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, A.; Del Din, S.; Barry, G.; Mathers, J.; Rochester, L. Instrumenting gait with an accelerometer: A system and algorithm examination. Med. Eng. Phys. 2015, 37, 400–407. [Google Scholar] [CrossRef]
- Zijlstra, W.; Hof, A.L. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 2003, 18, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Perneger, T.V. What’s wrong with Bonferroni adjustments. BMJ 1998, 316, 1236–1238. [Google Scholar] [CrossRef]
- Rothman, K.J. No adjustments are needed for multiple comparisons. Epidemiology 1990, 1, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Nicholson, T.R.J.; Cutter, W.; Hotopf, M. Assessing mental capacity: The Mental Capacity Act. BMJ 2008, 336, 322–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darweesh, S.K.; Licher, S.; Wolters, F.J.; Koudstaal, P.J.; Ikram, M.K. Quantitative gait, cognitive decline, and incident dementia: The Rotterdam Study. Alzheimer’s Dement. 2019, 15, 1264–1273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twardzik, E.E.; Duchowny, K.; Gallagher, A.; Alexander, N.; Strasburg, D.; Colabianchi, N.; Clarke, P. What features of the built environment matter most for mobility? Using wearable sensors to capture real-time outdoor environment demand on gait performance. Gait Posture 2019, 68, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Espay, A.J.; Bonato, P.; Nahab, F.B.; Maetzler, W.; Dean, J.M.; Klucken, J.; Eskofier, B.M.; Merola, A.; Horak, F.; Lang, A.E.; et al. Technology in Parkinson’s disease: Challenges and opportunities. Mov. Disord. 2016, 31, 1272–1282. [Google Scholar] [CrossRef] [Green Version]
- Khandelwal, S.; Wickström, N. Evaluation of the performance of accelerometer-based gait event detection algorithms in different real-world scenarios using the MAREA gait database. Gait Posture 2017, 51, 84–90. [Google Scholar] [CrossRef]
- Patterson, M.; Whelan, D.F.; Reginatto, B.; Caprani, N.; Walsh, L.; Smeaton, A.F.; Inomata, A.; Caulfield, B. Does external walking environment affect gait patterns? In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 27–31 August 2014; Volume 2014, pp. 2981–2984. [Google Scholar]
- Wang, W.; Adamczyk, P.G. Analyzing Gait in the Real World Using Wearable Movement Sensors and Frequently Repeated Movement Paths. Sensors 2019, 19, 1925. [Google Scholar] [CrossRef] [Green Version]
- Weiss, A.; Brozgol, M.; Dorfman, M.; Herman, T.; Shema, S.; Giladi, N.; Hausdorff, J.M. Does the Evaluation of Gait Quality During Daily Life Provide Insight Into Fall Risk? A Novel Approach Using 3-Day Accelerometer Recordings. Neurorehabilit. Neural Repair 2013, 27, 742–752. [Google Scholar] [CrossRef]
- Mc Ardle, R.; Del Din, S.; Donaghy, P.; Galna, B.; Thomas, A.; Rochester, L. Factors That Influence Habitual Activity in Mild Cognitive Impairment and Dementia. Gerontology 2019, 66, 197–208. [Google Scholar] [CrossRef] [Green Version]
- Mancini, M.; Weiss, A.; Herman, T.; Hausdorff, J.M. Turn Around Freezing: Community-Living Turning Behavior in People with Parkinson’s Disease. Front. Neurol. 2018, 9, 18. [Google Scholar] [CrossRef] [Green Version]
- Teipel, S.; König, A.; Hoey, J.; Kaye, J.; Krüger, F.; Robillard, J.M.; Kirste, T.; Babiloni, C. Use of nonintrusive sensor-based information and communication technology for real-world evidence for clinical trials in dementia. Alzheimer’s Dement. 2018, 14, 1216–1231. [Google Scholar] [CrossRef]
- Paillard, T.; Noé, F.; Bru, N.; Couderc, M.; Debove, L. The impact of time of day on the gait and balance control of Alzheimer’s patients. Chrono. Int. 2016, 33, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Bertoli, M.; Cereatti, A.; Trojaniello, D.; Avanzino, L.; Pelosin, E.; Del Din, S.; Rochester, L.; Ginis, P.; Bekkers, E.M.J.; Mirelman, A.; et al. Estimation of spatio-temporal parameters of gait from magneto-inertial measurement units: Multicenter validation among Parkinson, mildly cognitively impaired and healthy older adults. Biomed. Eng. Online 2018, 17, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Differences between All Groups | |||||
|---|---|---|---|---|---|
| Controls | AD | DLB | F/X2 | P | |
| N | 25 | 32 | 28 | ||
| Age | 74 ± 9 | 77 ± 6 | 76 ± 6 | 0.9 | 0.405 |
| Gender (m/f) | 11/14 D | 15/17 D | 22/6 A,C | 8.3 (138) * | 0.015 |
| Height (m) | 1.67 ± 0.10 | 1.67 ± 0.11 | 1.70 ± 0.10 | 1.5 † | 0.464 |
| Weight (kg) | 75.6 ± 16.4 | 72.3 ± 12.2 | 78.0 ± 12.8 | 2.4 † | 0.300 |
| BMI | 26.83 ± 4.33 | 26.03 ± 4.62 | 27.24 ± 4.82 | 0.1 | 0.833 |
| Faller (Yes/No) | 5/19 A,D | 15/17 C | 17/11 C | 8.5 * | 0.014 |
| NART | 122 ± 3 A,D | 117 ± 6 C | 115 ± 6 C | 23.3 † | <0.001 |
| sMMSE (0–30) | 29 ± 1 A,D | 23 ± 4 C | 24 ± 4 C | 44.5 † | <0.001 |
| ACE-III (0–100) | 96 ± 3 A,D | 72 ± 13 C | 73 ± 18 C | 50.0 † | <0.001 |
| CDR (0–3) | 0 ± 0 A,D | 0.8 ± 0.3 C | 0.8 ± 0.3 C | 70.0 | <0.001 |
| UPDRS (0–108) | 2 ± 3 A,D | 7 ± 6 C,D | 23 ± 15 C,A | 43.2 † | <0.001 |
| CIRS-G | 5 ± 3 A,D | 8 ± 4 C | 10 ± 4 C | 21.8 † | <0.001 |
| GDS | 1 ± 1 A,D | 4 ± 3 C | 5 ± 3 C | 29.2 † | <0.001 |
| ABC | 93 ± 10 A,D | 80 ± 18 C | 81 ± 17 C | 12.9 † | 0.002 |
| BADLS | 0 ± 0 A,*,D | 9 ± 7 C | 13 ± 6 C | 43.8 † | <0.001 |
| Lab-Based Gait | Controls | AD | DLB | F | p | Sig | Real-World Gait | Controls | AD | DLB | F | p | Sig |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | 25 | 32 | 28 | 25 | 32 | 28 | |||||||
| Mean step count | 109 | 115 | 11 | 99,224 | 78,794 | 72,482 | |||||||
| Pace | Pace | ||||||||||||
| Step Velocity (m/s) | 1.02 ± 143 | 0.90 ± 0.17 | 0.92 ± 0.13 | 9.05 | 0.014 | Step Velocity (m/s) | 1.08 ± 0.08 | 1.02 ± 0.11 | 0.98 ± 0.10 | 7.2 | 0.001 | b | |
| Step Length (m) | 0.55 ± 0.08 | 0.52 ± 0.08 | 0.54 ± 0.065 | 1.7 | 0.193 | Step Length (m) | 0.61 ± 0.04 | 0.58 ± 0.05 | 0.56 ± 0.05 | 7.2 | 0.001 | b | |
| Step Time SD (s) | 0.026 ± 0.015 | 0.043 ± 0.025 | 0.062 ± 0.045 | 9.1 | <0.001 | a,b | Step Time SD (s) | 0.166 ± 0.014 | 0.175 ± 0.018 | 0.177 ± 0.016 | 4.8 | 0.010 | b |
| Swing Time SD (s) | 0.021 ± 0.009 | 0.042 ± 0.024 | 0.053 ± 0.030 | 12.8 | <0.001 | a,b | Swing Time SD (s) | 0.140 ± 0.012 | 0.146 ± 0.015 | 0.152 ± 0.014 | 5.0 | 0.009 | b |
| Stance Time SD (s) | 0.027 ± 0.013 | 0.048 ± 0.027 | 0.065 ± 0.042 | 10.7 | <0.001 | a,b | Stance Time SD (s) | 0.177 ± 0.016 | 0.187 ± 0.019 | 0.193 ± 0.018 | 5.2 | 0.007 | b |
| Variability | Variability | ||||||||||||
| Step Length SD (m) | 0.043 ± 0.019 | 0.060 ± 0.026 | 0.082 ± 0.034 | 13.4 | <0.001 | a,b,c | Step Length SD (m) | 0.149 ± 0.017 | 0.147 ± 0.013 | 0.153 ± 0.008 | 1.5 | 0.226 | |
| Step Vel SD (m/s) | 0.084 ± 0.032 | 0.107 ± 0.045 | 0.142 ± 0.057 | 10.6 | <0.001 | b | Step Vel SD (m/s) | 0.359 ± 0.033 | 0.358 ± 0.033 | 0.369 ± 0.037 | 0.8 | 0.445 | |
| Rhythm | Rhythm | ||||||||||||
| Step Time (s) | 0.543 ± 0.048 | 0.576 ± 0.056 | 0.594 ± 0.060 | 5.8 | 0.004 | b | Step Time (s) | 0.594 ± 0.030 | 0.604 ± 0.024 | 0.603 ± 0.030 | 1.1 | 0.333 | |
| Swing Time (s) | 0.387 ± 0.041 | 0.423 ± 0.053 | 0.441 ± 0.064 | 7.0 | 0.002 | a,b | Swing Time (s) | 0.445 ± 0.029 | 0.458 ± 0.026 | 0.457 ± 0.028 | 0.9 | 0.396 | |
| Stance Time (s) | 0.699 ± 0.059 | 0.727 ± 0.067 | 0.744 ± 0.066 | 3.3 | 0.042 | Stance Time (s) | 0.743 ± 0.034 | 0.754 ± 0.025 | 0.752 ± 0.035 | 1.9 | 0.150 | ||
| Asymmetry | Asymmetry | ||||||||||||
| Step Time Asy (s) | 0.024 ± 0.016 | 0.034 ± 0.023 | 0.034 ± 0.019 | 2.3 | 0.112 | Step Time Asy (s) | 0.093 ± 0.008 | 0.099 ± 0.013 | 0.095 ± 0.008 | 2.7 | 0.073 | ||
| Swing Time Asy (s) | 0.021 ± 0.012 | 0.039 ± 0.029 | 0.034 ± 0.020 | 5.2 | 0.007 | a,b | Swing Time Asy (s) | 0.086 ± 0.008 | 0.090 ± 0.011 | 0.089 ± 0.009 | 1.8 | 0.179 | |
| Stance Time Asy (s) | 0.021 ± 0.012 | 0.039 ± 0.027 | 0.034 ± 0.019 | 4.7 | 0.011 | Stance Time Asy (s) | 0.095 ± 0.008 | 0.100 ± 0.013 | 0.096 ± 0.010 | 2.4 | 0.096 | ||
| Postural Control | Postural Control | ||||||||||||
| Step Length Asy (m) | 0.067 ± 0.039 | 0.104 ± 0.070 | 0.088 ± 0.061 | 2.7 | 0.076 | Step Length Asy (m) | 0.086 ± 0.007 | 0.089 ± 0.012 | 0.082 ± 0.010 | 3.4 | 0.040 |
| <10 s Bouts | 10–30 s Bouts | |||||||
|---|---|---|---|---|---|---|---|---|
| Controls | AD | DLB | (p) | Controls | AD | DLB | (p) | |
| Bouts per day | 359 ± 102 | 356 ± 151 | 339 ± 126 | 0.723 | 199 ± 59 | 195 ± 70 | 186 ± 74 | 0.697 |
| Steps per day | 1775 ± 546 | 1763 ± 735 | 1784 ± 700 | 0.992 | 3694 ± 1093 | 3660 ± 1314 | 3583 ± 1424 | 0.950 |
| Pace | ||||||||
| Step Velocity (m/s) | 0.91 ± 0.06 | 0.89 ± 0.09 | 0.86 ± 0.08 | 0.062 | 1.01 ± 0.06 | 0.98 ± 0.09 | 0.96 ± 0.09 | 0.019 † |
| Step Length (m) | 0.53 ± 0.02 | 0.52 ± 0.03 | 0.49 ± 0.03 | ≤0.001 † | 0.58 ± 0.03 | 0.56 ± 0.04 | 0.54 ± 0.04 | 0.001 † |
| Swing SD (s) | 0.170 ± 0.013 | 0.169 ± 0.012 | 0.170 ± 0.012 | 0.951 | 0.156 ± 0.012 | 0.155 ± 0.015 | 0.160 ± 0.015 | 0.336 |
| Step Time SD (s) | 0.206 ± 0.013 | 0.207 ± 0.01 | 0.205 ± 0.014 | 0.564 † | 0.183 ± 0.014 | 0.184 ± 0.016 | 0.189 ± 0.018 | 0.702 † |
| Stance SD (s) | 0.220 ± 0.013 | 0.220 ± 0.014 | 0.220 ± 0.014 | 0.881 † | 0.195 ± 0.014 | 0.196 ± 0.016 | 0.202 ± 0.020 | 0.263 |
| Variability (SD) | ||||||||
| Step Velocity SD (m/s) | 0.384 ± 0.027 | 0.376 ± 0.044 | 0.370 ± 0.042 | 0.276 † | 0.380 ± 0.030 | 0.372 ± 0.039 | 0.379 ± 0.042 | 0.588 |
| Step Length SD (m) | 0.163 ± 0.007 | 0.158 ± 0.009 | 0.156 ± 0.009 | 0.009 † | 0.153 ± 0.009 | 0.151 ± 0.009 | 0.153 ± 0.008 | 0.548 † |
| Rhythm | ||||||||
| Step Time (ms) | 0.616 ± 0.022 | 0.614 ± 0.029 | 0.602 ± 0.025 | 0.107 | 0.618 ± 0.027 | 0.618 ± 0.030 | 0.610 ± 0.030 | 0.476 |
| Swing (ms) | 0.472 ± 0.023 | 0.471 ± 0.029 | 0.461 ± 0.023 | 0.163 † | 0.473 ± 0.028 | 0.476 ± 0.32 | 0.468 ± 0.029 | 0.560 |
| Stance (ms) | 0.764 ± 0.024 | 0.763 ± 0.031 | 0.750 ± 0.030 | 0.131 † | 0.767 ± 0.028 | 0.765 ± 0.030 | 0.758 ± 0.035 | 0.516 |
| Asymmetry | ||||||||
| Step Time Asy (ms) | 0.162 ± 0.012 | 0.170 ± 0.021 | 0.160 ± 0.013 | 0.086 † | 0.072 ± 0.007 | 0.075 ± 0.012 | 0.072 ± 0.009 | 0.573 † |
| Swing Asy (ms) | 0.123 ± 0.010 | 0.127 ± 0.017 | 0.122 ± 0.012 | 0.765 † | 0.067 ± 0.007 | 0.070 ± 0.011 | 0.067 ± 0.009 | 0.526 † |
| Stance Asy (ms) | 0.165 ± 0.011 | 0.171 ± 0.019 | 0.162 ± 0.014 | 0.132 † | 0.073 ± 0.007 | 0.076 ± 0.012 | 0.073 ± 0.009 | 0.565 † |
| Postural Control | ||||||||
| Step Length Asy (m) | 0.121 ± 0.010 | 0.121 ± 0.015 | 0.110 ± 0.014 | 0.002 † | 0.081 ± 0.008 | 0.080 ± 0.013 | 0.073 ± 0.012 | 0.014 † |
| 30–60 s bouts | >60 s bouts | |||||||
| Controls | AD | DLB | (p) | Controls | AD | DLB | (p) | |
| Bouts per day | 42 ± 15 | 38 ± 16 | 36 ± 19 | 0.311 | 26 ± 12 | 18 ± 8 | 16 ± 11 | 0.011 |
| Steps per day | 2105 ± 715 | 1846 ± 788 | 1783 ± 956 | 0.334 | 6601 ± 3621 | 4228 ± 2956 | 3205 ± 2786 | 0.001 |
| Pace | ||||||||
| Step Velocity (m/s) | 1.05 ± 0.06 | 1.01 ± 0.08 | 1.00 ± 0.11 | 0.112 | 1.15 ± 0.11 | 1.08 ± 0.13 | 1.05 ± 0.13 | 0.010 |
| Step Length (m) | 0.60 ± 0.03 | 0.58 ± 0.04 | 0.57 ± 0.04 | 0.019 † | 0.63 ± 0.06 | 0.60 ± 0.06 | 0.59 ± 0.06 | 0.044 |
| Swing SD (s) | 0.149 ± 0.010 | 0.151 ± 0.015 | 0.155 ± 0.018 | 0.283 | 0.114 ± 0.019 | 0.125 ± 0.025 | 0.129 ± 0.025 | 0.069 |
| Step Time SD (s) | 0.175 ± 0.012 | 0.179 ± 0.019 | 0.183 ± 0.022 | 0.263 | 0.137 ± 0.024 | 0.149 ± 0.033 | 0.153 ± 0.032 | 0.119 |
| Stance SD (s) | 0.186 ± 0.013 | 0.190 ± 0.021 | 0.195 ± 0.023 | 0.225 | 0.147 ± 0.027 | 0.161 ± 0.036 | 0.153 ± 0.032 | 0.110 |
| Variability (SD) | ||||||||
| Step Velocity SD (m/s) | 0.366 ± 0.030 | 0.364 ± 0.037 | 0.372 ± 0.042 | 0.706 | 0.316 ± 0.054 | 0.320 ± 0.063 | 0.329 ± 0.058 | 0.719 |
| Step Length SD (m) | 0.150 ± 0.011 | 0.148 ± 0.012 | 0.151 ± 0.010 | 0.702 † | 0.132 ± 0.028 | 0.133 ± 0.025 | 0.138 ± 0.020 | 0.534 † |
| Rhythm | ||||||||
| Step Time (ms) | 0.614 ± 0.027 | 0.615 ± 0.025 | 0.612 ± 0.036 | 0.934 | 0.570 ± 0.042 | 0.588 ± 0.031 | 0.594 ± 0.39 | 0.161 † |
| Swing (ms) | 0.466 ± 0.026 | 0.470 ± 0.025 | 0.467 ± 0.034 | 0.876 | 0.419 ± 0.035 | 0.437 ± 0.027 | 0.443 ± 0.036 | 0.023 |
| Stance (ms) | 0.763 ± 0.029 | 0.764 ± 0.026 | 0.761 ± 0.042 | 0.920 | 0.719 ± 0.050 | 0.737 ± 0.036 | 0.746 ± 0.044 | 0.194 † |
| Asymmetry | ||||||||
| Step Time Asy (ms) | 0.040 ± 0.005 | 0.042 ± 0.007 | 0.043 ± 0.006 | 0.327 † | 0.023 ± 0.006 | 0.027 ± 0.006 | 0.027 ± 0.007 | 0.040 † |
| Swing Asy (ms) | 0.036 ± 0.005 | 0.038 ± 0.006 | 0.038 ± 0.006 | 0.206 † | 0.021 ± 0.005 | 0.025 ± 0.006 | 0.025 ± 0.006 | 0.022 † |
| Stance Asy (ms) | 0.040 ± 0.005 | 0.042 ± 0.007 | 0.042 ± 0.007 | 0.410 † | 0.023 ± 0.005 | 0.027 ± 0.006 | 0.026 ± 0.007 | 0.017 † |
| Postural Control | ||||||||
| Step Length Asy (m) | 0.048 ± 0.006 | 0.50 ± 0.010 | 0.047 ± 0.009 | 0.308 † | 0.026 ± 0.007 | 0.031 ± 0.015 | 0.032 ± 0.009 | 0.040 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mc Ardle, R.; Del Din, S.; Donaghy, P.; Galna, B.; Thomas, A.J.; Rochester, L. The Impact of Environment on Gait Assessment: Considerations from Real-World Gait Analysis in Dementia Subtypes. Sensors 2021, 21, 813. https://doi.org/10.3390/s21030813
Mc Ardle R, Del Din S, Donaghy P, Galna B, Thomas AJ, Rochester L. The Impact of Environment on Gait Assessment: Considerations from Real-World Gait Analysis in Dementia Subtypes. Sensors. 2021; 21(3):813. https://doi.org/10.3390/s21030813
Chicago/Turabian StyleMc Ardle, Ríona, Silvia Del Din, Paul Donaghy, Brook Galna, Alan J Thomas, and Lynn Rochester. 2021. "The Impact of Environment on Gait Assessment: Considerations from Real-World Gait Analysis in Dementia Subtypes" Sensors 21, no. 3: 813. https://doi.org/10.3390/s21030813