The Danger of Walking with Socks: Evidence from Kinematic Analysis in People with Progressive Multiple Sclerosis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Gait Analysis
2.3. sEMG Recording
2.4. Clinical Assessment
2.5. Statistics
3. Results
3.1. Subjects Demographics
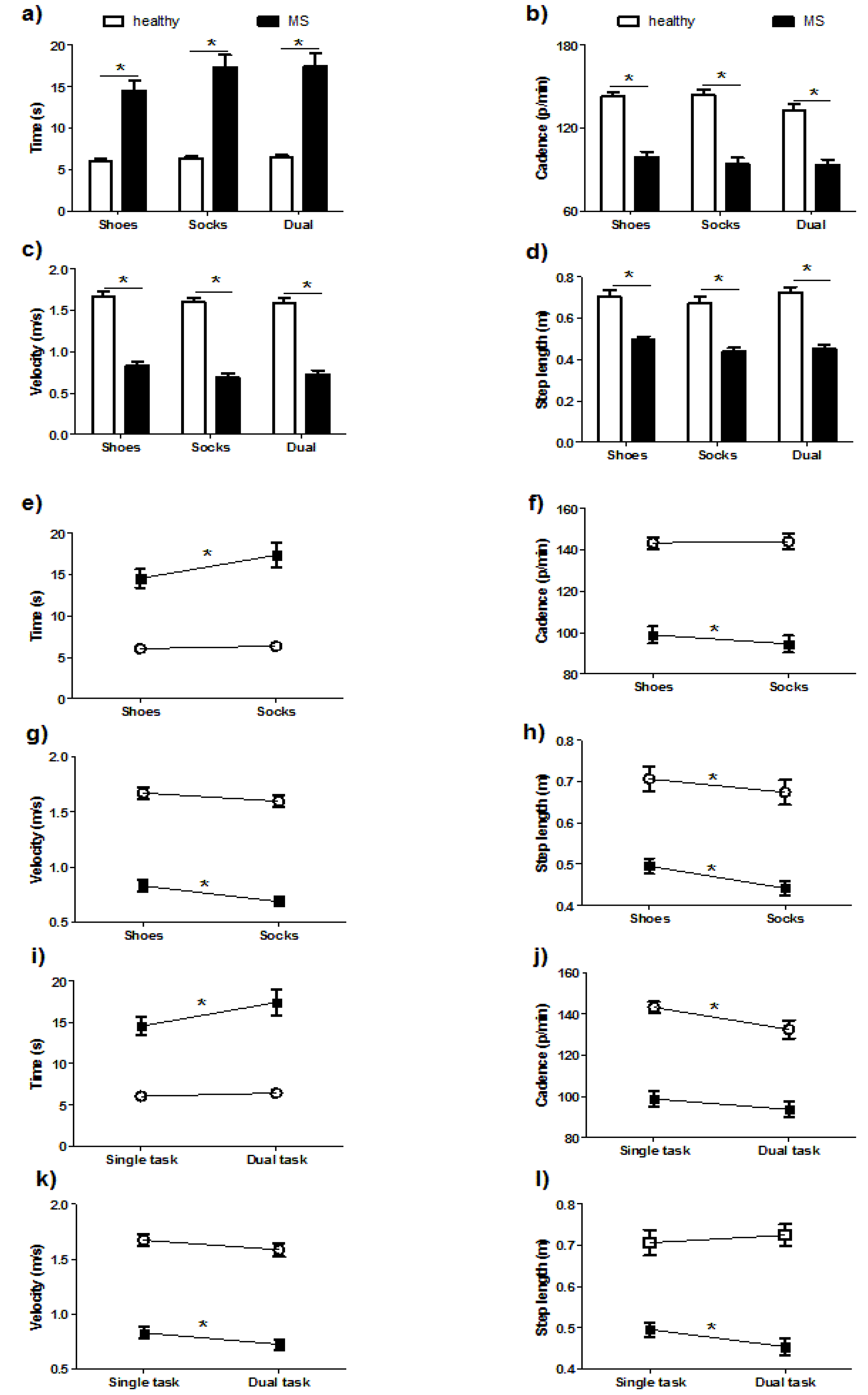
3.2. Comparisons of Spatiotemporal Parameters
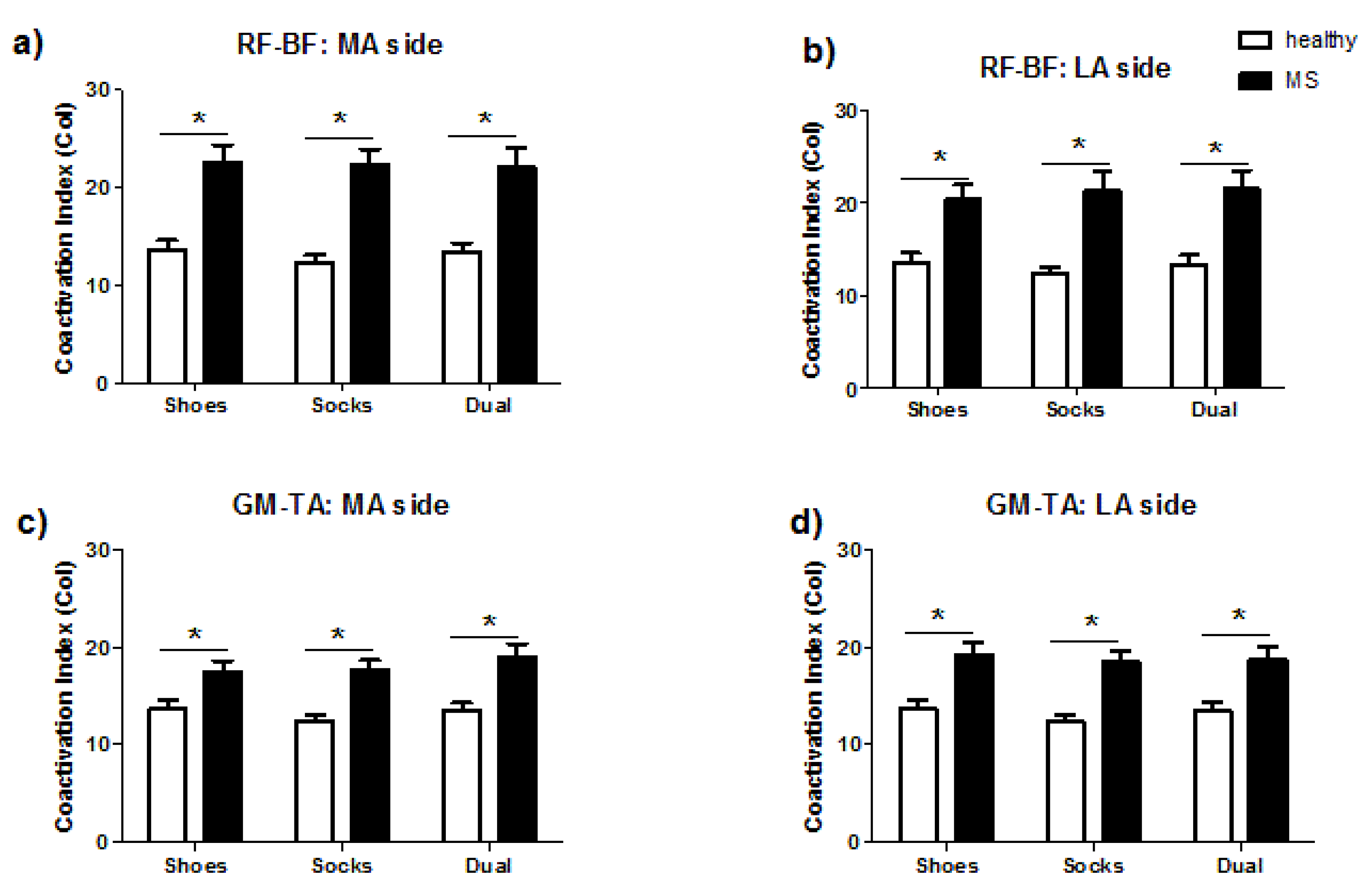
3.3. Comparisons of Coactivation Index
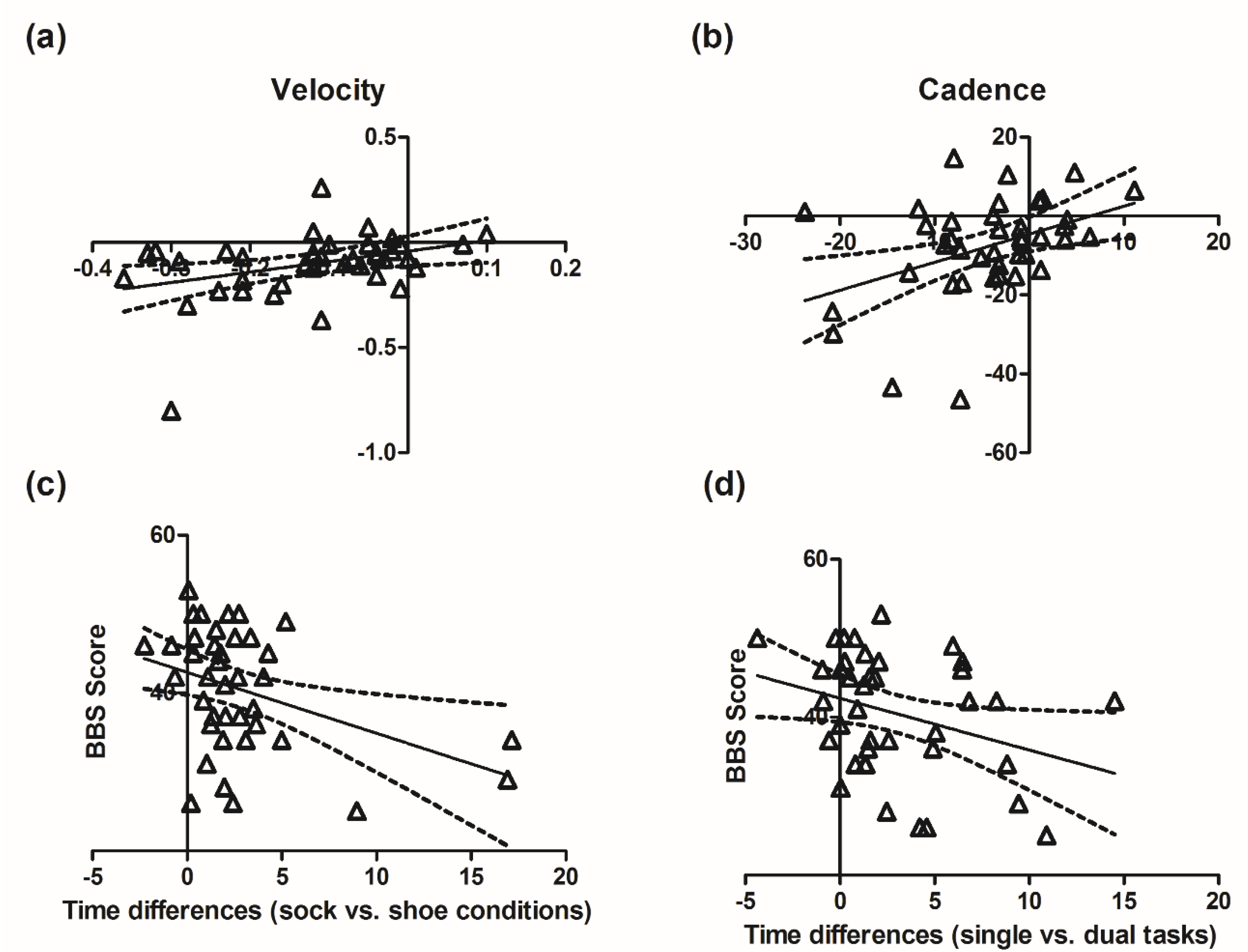
3.4. Correlations among Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lassmann, H.; Bruck, W.; Lucchinetti, C.F. The immunopathology of multiple sclerosis: An overview. Brain Pathol. 2007, 17, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee on Multiple Sclerosis. Current Status and Strategies for the Future. Multiple Sclerosis: Current Status and Strategies for the Future; Joy, J.E., Johnston, R.B., Jr., Eds.; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Heesen, C.; Böhm, J.; Reich, C.; Kasper, J.; Goebel, M.; Gold, S.M. Patient perception of bodily functions in multiple sclerosis: Gait and visual function are the most valuable. Mult. Scler. J. 2008, 14, 988–991. [Google Scholar] [CrossRef] [PubMed]
- Kalron, A.; Givon, U. Gait characteristics according to pyramidal, sensory and cerebellar EDSS subcategories in people with multiple sclerosis. J. Neurol. 2016, 263, 1796–1801. [Google Scholar] [CrossRef] [PubMed]
- Lizama, L.E.C.; Khan, F.; Lee, P.V.; Galea, M.P. The use of laboratory gait analysis for understanding gait deterioration in people with multiple sclerosis. Mult. Scler. J. 2016, 22, 1768–1776. [Google Scholar] [CrossRef]
- Shanahan, C.J.; Boonstra, F.M.C.; Lizama, L.E.C.; Strik, M.; Moffat, B.A.; Khan, F.; Kilpatrick, T.; Van Der Walt, A.; Galea, M.P.; Kolbe, S.C. Technologies for Advanced Gait and Balance Assessments in People with Multiple Sclerosis. Front. Neurol. 2018, 8, 708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vítečková, S.; Horáková, H.; Poláková, K.; Krupička, R.; Růžička, E.; Brožová, H. Agreement between the GAITRite® System and the Wearable Sensor BTS G-Walk® for measurement of gait parameters in healthy adults and Parkinson’s disease patients. PeerJ 2020, 8, e8835. [Google Scholar] [CrossRef]
- Etemadi, Y. Dual task cost of cognition is related to fall risk in patients with multiple sclerosis: A prospective study. Clin. Rehabil. 2016, 31, 278–284. [Google Scholar] [CrossRef]
- Larsen, E.R.; Mosekilde, L.; Foldspang, A. Correlates of falling during 24 h among elderly Danish community residents. Prev. Med. 2004, 39, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Menz, H.B.; Morris, M.E.; Lord, S.R. Footwear Characteristics and Risk of Indoor and Outdoor Falls in Older People. Gerontology 2006, 52, 174–180. [Google Scholar] [CrossRef]
- Kelsey, J.L.; Procter-Gray, E.; Nguyen, U.-S.D.T.; Li, W.; Kiel, D.P.; Hannan, M.T. Footwear and falls in the home among older individuals in the MOBILIZE Boston Study. Footwear Sci. 2010, 2, 123–129. [Google Scholar] [CrossRef]
- Coote, S.; Sosnoff, J.J.; Gunn, H. Fall Incidence as the Primary Outcome in Multiple Sclerosis Falls-Prevention Trials: Recommendation from the International MS Falls Prevention Research Network. Int. J. MS Care 2014, 16, 178–184. [Google Scholar] [CrossRef] [Green Version]
- Leone, C.; Patti, F.; Feys, P. Measuring the cost of cognitive-motor dual tasking during walking in multiple sclerosis. Mult. Scler. J. 2014, 21, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- ICH Harmonised Tripartite Guideline: Guideline for Good Clinical Practice. J. Postgrad. Med. 2001, 47, 199–203.
- Unnithan, V.B.; Dowling, J.J.; Frost, G.; Ayub, B.V.; Bar-Or, O. Cocontraction and phasic activity during GAIT in children with cerebral palsy. Electromyogr. Clin. Neurophysiol. 1996, 36, 487–494. [Google Scholar] [PubMed]
- Bohannon, R.W.; Smith, M.B. Interrater Reliability of a Modified Ashworth Scale of Muscle Spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef]
- Hermans, G.; Clerckx, B.; Vanhullebusch, T.; Segers, J.; Vanpee, G.; Robbeets, C.; Casaer, M.P.; Wouters, P.; Gosselink, R.; Berghe, G.V.D. Interobserver agreement of medical research council sum-score and handgrip strength in the intensive care unit. Muscle Nerve 2011, 45, 18–25. [Google Scholar] [CrossRef]
- Toomey, E.; Coote, S. Between-Rater Reliability of the 6-Minute Walk Test, Berg Balance Scale, and Handheld Dynamometry in People with Multiple Sclerosis. Int. J. MS Care 2013, 15, 1–6. [Google Scholar] [CrossRef]
- Hobart, J.C.; Riazi, A.; Lamping, D.L.; Fitzpatrick, R.; Thompson, A.J. Measuring the impact of MS on walking ability: The 12-Item MS Walking Scale (MSWS-12). Neurology 2003, 60, 31–36. [Google Scholar] [CrossRef]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef]
- Hobart, J.C.; Riazi, A.; Thompson, A.J.; Styles, I.M.; Ingram, W.; Vickery, P.J.; Warner, M.; Fox, P.J.; Zajicek, J. Getting the measure of spasticity in multiple sclerosis: The Multiple Sclerosis Spasticity Scale (MSSS-88). Brain 2005, 129, 224–234. [Google Scholar] [CrossRef] [Green Version]
- Farrar, J.T.; Troxel, A.B.; Stott, C.; Duncombe, P.; Jensen, M.P. Validity, reliability, and clinical importance of change in a 0–10 numeric rating scale measure of spasticity: A post hoc analysis of a randomized, double-blind, placebo-controlled trial. Clin. Ther. 2008, 30, 974–985. [Google Scholar] [CrossRef]
- Guzzo, A.; Meggiolaro, A.; Mannocci, A.; Tecca, M.; Salomone, I.; La Torre, G. Conley Scale: Assessment of a fall risk prevention tool in a General Hospital. J. Prev. Med. Hyg. 2015, 56, E77–E87. [Google Scholar]
- Ottenbacher, K.J.; Hsu, Y.; Granger, C.V.; Fiedler, R.C. The reliability of the functional independence measure: A quantitative review. Arch. Phys. Med. Rehabil. 1996, 77, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Berg, K.O.; Wood-Dauphinee, S.L.; Williams, J.I.; Maki, B. Measuring balance in the elderly: Validation of an instrument. Can. J. Public Health 1992, 83, S7–S11. [Google Scholar]
- Boudarham, J.; Hameau, S.; Zory, R.; Hardy, A.; Bensmail, D.; Roche, N. Coactivation of Lower Limb Muscles during Gait in Patients with Multiple Sclerosis. PLoS ONE 2016, 11, e0158267. [Google Scholar] [CrossRef]
- Papagiannis, G.I.; Triantafyllou, A.I.; Roumpelakis, I.M.; Zampeli, F.; Eleni, P.G.; Koulouvaris, P.; Papadopoulos, E.C.; Papagelopoulos, P.J.; Babis, G.C. Methodology of surface electromyography in gait analysis: Review of the literature. J. Med. Eng. Technol. 2019, 43, 59–65. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | PwPMS (n = 40) | HC (n = 15) |
|---|---|---|
| Gender (M/F) | 20 / 20 | 4 / 9 |
| Age (years) | 50.9 ± 9.8 | 52.7 ± 4.4 |
| BMI | 24.0 ± 4.6 | 24.0 ± 2.2 |
| EDSS | 5.5 ± 1.1 | - |
| More Affected Side (R/L) | 23 / 17 | - |
| MAS (more affected side) | 2.4 ± 2.0 | - |
| MRC scale (more affected side) | 13.1 ± 3.2 | - |
| MSWS-12 | 38.6 ± 9.7 | - |
| FSS | 39.5 ± 15.0 | - |
| MSSS-88 | 188.6 ± 52.7 | - |
| Conley scale | 2.9 ± 1.8 | - |
| Barthel scale | 88.4 ± 10.3 | - |
| FIM | 112.5 ± 9.0 | - |
| BBS | 40.5 ± 7.7 | - |
| NRS | 3.9 ± 2.6 | - |
| Variables | Conditions | EDSS | MSWS-12 | FSS | MSSS-88 | Conley | Barthel | FIM | BBS | NRS |
|---|---|---|---|---|---|---|---|---|---|---|
| Time | shoes | 0.48 ** | 0.22 | −0.23 | −0.01 | −0.07 | −0.11 | −0.40 * | −0.40 * | 0.05 |
| (N = 40) | socks | 0.50 ** | 0.22 | −0.27 | −0.04 | −0.08 | −0.01 | −0.35 | −0.32 | 0.06 |
| DT | 0.40 * | 0.15 | −0.16 | 0.03 | −0.16 | −0.00 | −0.39 * | −0.29 | −0.03 | |
| Cadence | shoes | −0.49 ** | −0.20 | 0.31 | 0.08 | 0.11 | 0.08 | 0.33 | 0.36 | 0.07 |
| (N = 40) | socks | −0.50 ** | −0.21 | 0.32 | 0.06 | 0.13 | 0.02 | 0.33 | 0.35 | 0.07 |
| DT | −0.43 ** | −0.13 | 0.15 | −0.09 | 0.14 | −0.07 | 0.29 | 0.27 | 0.16 | |
| Velocity | shoes | −0.48 ** | −0.22 | 0.23 | 0.02 | 0.06 | 0.10 | 0.41 ** | 0.40 * | −0.05 |
| (N = 40) | socks | −0.50 ** | −0.20 | 0.27 | 0.03 | 0.11 | 0.03 | 0.40 * | 0.36 | −0.07 |
| DT | −0.42 ** | −0.13 | 0.18 | 0.01 | 0.11 | 0.06 | 0.42 ** | 0.34 | −0.08 | |
| Step | shoes | −0.27 | −0.03 | 0.24 | 0.13 | 0.08 | 0.06 | 0.32 | 0.24 | −0.13 |
| Length | socks | −0.18 | −0.06 | 0.14 | 0.03 | −0.01 | −0.04 | 0.11 | 0.04 | −0.21 |
| (N = 40) | DT | −0.15 | −0.08 | 0.11 | 0.02 | 0.12 | 0.03 | 0.30 | 0.14 | −0.13 |
| Variables | Conditions | EDSS | MSWS-12 | FSS | MSSS-88 | Conley | Barthel | FIM | BBS | NRS |
|---|---|---|---|---|---|---|---|---|---|---|
| RF-BF MA | shoes | 0.38 | 0.06 | −0.27 | −0.03 | −0.10 | −0.13 | −0.30 | −0.15 | −0.41 |
| (N = 31) | socks | 0.42 * | −0.10 | −0.50 ** | −0.11 | −0.18 | −0.02 | −0.14 | −0.12 | −0.30 |
| DT | 0.48 ** | −0.04 | −0.38 | −0.13 | −0.05 | 0.05 | −0.08 | 0.02 | −0.35 | |
| RF-BF LA | shoes | 0.12 | −0.28 | −0.46 | −0.21 | −0.09 | −0.02 | −0.13 | 0.02 | −0.22 |
| (N = 22) | socks | 0.21 | 0.07 | −0.55 * | −0.18 | 0.03 | −0.05 | −0.12 | 0.02 | −0.02 |
| DT | 0.26 | −0.32 | −0.41 | −0.13 | −0.08 | −0.01 | −0.00 | 0 | −0.05 | |
| GM-TA MA | shoes | 0.13 | −0.04 | 0.02 | 0.16 | −0.06 | 0.20 | −0.03 | 0.10 | 0.17 |
| (N = 40) | socks | 0.07 | 0.02 | −0.01 | 0.07 | 0.06 | 0.14 | −0.08 | 0.01 | 0.13 |
| DT | 0.17 | −0.02 | 0.01 | 0.02 | −0.05 | 0.22 | −0.07 | 0.01 | 0.12 | |
| GM-TA LA | shoes | 0.22 | 0.07 | −0.09 | 0.07 | 0.11 | 0.12 | −0.34 | −0.39 | 0.18 |
| (N = 40) | socks | 0.16 | 0.10 | 0.13 | 0.18 | 0.33 | 0 | −0.28 | −0.30 | 0.22 |
| DT | 0.02 | −0.10 | −0.11 | −0.01 | 0.22 | 0.03 | −0.14 | −0.18 | 0.27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, S.-C.; Dalla Costa, G.; Pisa, M.; Gregoris, L.; Leccabue, G.; Congiu, M.; Comi, G.; Leocani, L. The Danger of Walking with Socks: Evidence from Kinematic Analysis in People with Progressive Multiple Sclerosis. Sensors 2020, 20, 6160. https://doi.org/10.3390/s20216160
Huang S-C, Dalla Costa G, Pisa M, Gregoris L, Leccabue G, Congiu M, Comi G, Leocani L. The Danger of Walking with Socks: Evidence from Kinematic Analysis in People with Progressive Multiple Sclerosis. Sensors. 2020; 20(21):6160. https://doi.org/10.3390/s20216160
Chicago/Turabian StyleHuang, Su-Chun, Gloria Dalla Costa, Marco Pisa, Lorenzo Gregoris, Giulia Leccabue, Martina Congiu, Giancarlo Comi, and Letizia Leocani. 2020. "The Danger of Walking with Socks: Evidence from Kinematic Analysis in People with Progressive Multiple Sclerosis" Sensors 20, no. 21: 6160. https://doi.org/10.3390/s20216160